Retinal detachment (RD) is defined as a condition in which the inner part of the neural retina (sensory retina) from the photoreceptor layer separates from the retinal pigment epithelium (RPE) layer, with subretinal fluid accumulating between them. Embryologically, the neural retina differentiates from the inner layer of the neuroectoderm, while the RPE differentiates from the outer layer, so their attachment is inherently weak, making detachment prone to occur due to various causes.10,20)
When retinal detachment occurs, photoreceptor cells are separated from the oxygen and nutrient supply from the RPE and choroid. Degeneration and shedding of photoreceptor outer segments begin early after onset, and if prolonged, progress to irreversible photoreceptor damage. This time dependency is the basis for the “urgency” of retinal detachment. In particular, when the macula (fovea) detaches, central vision rapidly and severely declines, and visual recovery after surgery tends to be incomplete.
Xiong J, et al. A review of rhegmatogenous retinal detachment: past, present and future. Wien Med Wochenschr. 2025. Figure 3. PMCID: PMC12031774. License: CC BY.
The name rhegmatogenous retinal detachment (RRD) derives from the Greek word “rhegma,” meaning “rent” or “tear.” The annual incidence varies by region but is generally around 10–15 per 100,000 population. A history of retinal detachment in the fellow eye or a family history are risk factors for developing the condition. 7)
Age of onset shows a bimodal distribution:
Young adult peak (20s): Shallow detachment due to atrophic holes within lattice degeneration
As axial length increases, degeneration of the retina and vitreous progresses, and the risk of rhegmatogenous retinal detachment rises stepwise. Compared to emmetropic eyes with axial length less than 24 mm, eyes with axial length of 26 mm or more (equivalent to high myopia) have a 2- to 3-fold higher incidence of peripheral retinal lattice degeneration and atrophic holes. In Japan, the proportion of rhegmatogenous retinal detachment due to macular holes in highly myopic eyes (over -6 diopters) is about 5% of all rhegmatogenous retinal detachments, which is higher than the 0.5-2.0% in Europe and the United States.
Atopic dermatitis (ciliary body tears due to eye rubbing)
Iatrogenic and external risks
After cataract surgery: Large studies suggest that within one year after surgery, about 1 in 500 patients may develop rhegmatogenous retinal detachment or retinal tear; younger age, male sex, myopia, and intraoperative anterior vitrectomy are risk factors1, 17)
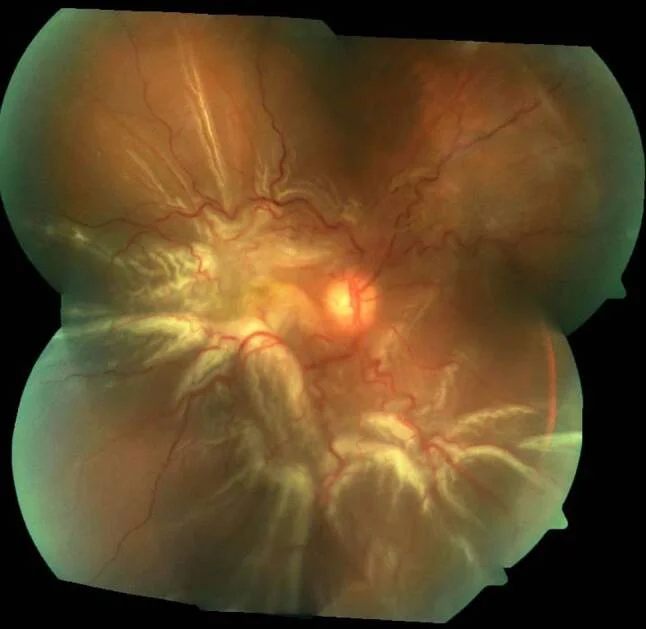
Tractional retinal detachment occurs when incomplete posterior vitreous detachment leads to strong vitreous traction on the retina. It can be broadly classified into two types: fibrovascular membranes containing neovascularization from intraocular proliferative cells and vitreoretinal traction.
Tractional retinal detachment is immobile and has a concave shape. Tent-shaped detachment occurs at the epicenter of neovascularization or along retinal vessels. If adhesion is extensive, it becomes a “tabletop type” (Mount Fuji type). If the detachment is dome-shaped and mobile, suspect combined tractional-rhegmatogenous retinal detachment.
Miyamoto T, et al. A case of tractional retinal detachment associated with congenital retinal vascular hypoplasia in the superotemporal quadrant treated by vitreous surgery. BMC Ophthalmol. 2020. Figure 2. PMCID: PMC7542339. License: CC BY.
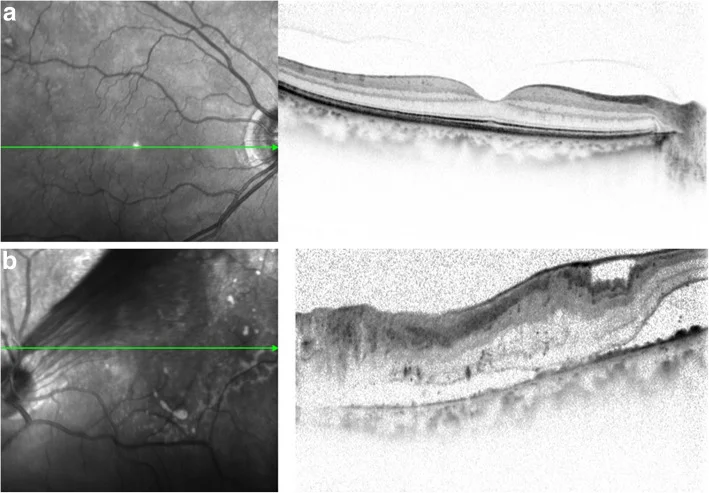
Exudative retinal detachment is a non-rhegmatogenous retinal detachment caused by accumulation of exudative fluid under the retina due to functional disorders of retinal vessels, RPE, choroid, etc. Breakdown of the blood-retinal barrier (BRB) is the final common pathway, and causes are diverse.
Typical clinical features
The detached retina protrudes in a dome shape with a smooth surface
Maggio E, et al. Multimodal imaging findings in a case of severe Central Serous Chorioretinopathy in an uncomplicated pregnancy. BMC Ophthalmol. 2015. Figure 1. PMCID: PMC4688919. License: CC BY.
Traumatic retinal detachment is caused by blunt or perforating ocular trauma. In blunt trauma, retinal detachment occurs in 12% immediately after injury, 30% within 1 month, 50% within 8 months, and 80% within 24 months, according to reports, requiring long-term follow-up. A special type is retinal dialysis caused by trauma.
QDoes retinal detachment heal on its own?
A
It varies greatly by type. Rhegmatogenous and tractional retinal detachments generally do not heal spontaneously. If left untreated, they progressively enlarge and eventually lead to blindness. On the other hand, exudative retinal detachment may resolve spontaneously with treatment of the underlying cause (e.g., VKH or drug-induced). However, if the cause is neoplastic, tumor treatment takes priority. If floaters, photopsia, or visual field defects appear, it is important to see an ophthalmologist promptly without waiting for spontaneous healing.
OCT is an essential examination for confirming the diagnosis of retinal detachment, differentiating its types, planning surgery, and following up postoperatively.
Purpose of examination
Information obtained
Confirmation of presence and extent of macular detachment
Prediction of visual prognosis and determination of surgical indication
Differential diagnosis of disease type
Rhegmatogenous vs exudative (characteristics and morphology of SRF)
Location of proliferative membrane and retinal traction pattern
Postoperative monitoring
Follow-up of retinal reattachment and macular recovery
Structures to observe on OCT and their significance
When reading OCT for preoperative and postoperative evaluation of retinal detachment, pay attention to the following structures. Postoperative ellipsoid zone (EZ) recovery depends on the duration and extent of detachment, and the recovery of EZ length serves as an indicator of postoperative visual acuity. 3,15)
Structure
Meaning of findings
Ellipsoid zone (EZ)
Hyperreflective band at the inner/outer segment junction of photoreceptors. Longer detachment duration leads to more indistinctness/defects → indicator of postoperative visual prognosis
External limiting membrane (ELM)
Hyperreflective band inner to EZ. More protected than EZ; recovery of ELM precedes that of EZ
Subretinal hyperreflective material (SHRM)
PRE cells and inflammatory debris under the detached retina. If it remains after surgery, it can impede EZ recovery.
Characteristics of subretinal fluid (SRF)
In rhegmatogenous detachment, SRF is hypoechoic and homogeneous; in exudative detachment, it may appear dome-shaped with punctate hyperreflectivity.
This is an essential examination when the fundus is not visible (vitreous hemorrhage, cataract, corneal opacity). The probe is applied to the cornea or sclera, and longitudinal, transverse, and axial sections are systematically imaged.
Basic imaging technique
Apply the probe at 10 MHz or higher (ophthalmic high frequency) and observe the dynamics of the ocular wall.
When the patient moves the eye: the retina moves as a highly reflective rigid membrane (confirming attachment to the posterior wall), the vitreous sways softly (positive aftermovement), and proliferative membranes show intermediate movement.
Confirming attachment to the posterior wall at the optic disc identifies complete retinal detachment (V-shaped or T-shaped).
Finding
Significance
Confirmation of total retinal detachment
Attachment to posterior wall at optic disc → determines ERG and surgical indication
Ultra-widefield laser fundus cameras (OptosSS, Clarijs, etc.) capture 80–200° of the peripheral retina (near the ora serrata) in a single shot.
Detects peripheral tears and lattice degeneration that are often missed with conventional fundus photography (45°)
Useful for objective documentation of tear location and extent before surgery (improves surgical planning accuracy)
Can monitor for new peripheral tears or detachments during postoperative follow-up
However, confirmation of small tears (<0.5 DD) requires combined use with scleral depressed fundus examination; absence of a tear on UWF images does not rule it out
However, small tears may not be detected by fundus camera, so combined use with scleral depressed fundus examination is essential
QWhy is OCT or ultrasound needed in addition to fundus examination?
A
Fundus examination (indirect ophthalmoscopy) is excellent for assessing the location and shape of tears, but OCT can quantitatively evaluate the presence, extent, and type of macular detachment. When the fundus is not visible due to vitreous hemorrhage, B-mode ultrasound becomes indispensable. Particularly in tractional retinal detachment, preoperative mapping of proliferative membranes with ultrasound is important for surgical planning.
Cryopexy and scleral buckle (silicone material) are applied externally to create an indentation at the tear site and reattach the retina.
Indications: Young patients, no posterior vitreous detachment, simple peripheral tears
Advantages: Preserves the lens, maintains eye shape close to natural state
Disadvantages: Not suitable for complex cases or proliferative changes
Pars Plana Vitrectomy (PPV)
The vitreous is removed, fluid-gas exchange is performed to flatten and reattach the retina, and laser photocoagulation closes the tear.
Indications: Middle-aged and elderly patients, PVD, complex tears, vitreous hemorrhage, PVRAdvantages: Can manage complex pathology, direct visualization
Disadvantages: Accelerates cataract progression, requires postoperative positioning
Pneumatic Retinopexy (PR)
Inject expanding gas into the eye to close the tear and reattach the retina. Can be performed as an outpatient procedure.
Indications: Single tear confined to the upper half
Advantages: No hospitalization required, minimally invasive
Disadvantages: Limited applicable cases, slightly lower success rate than other procedures
Middle-aged/elderly, with PVD, deep tear, multiple tears, with PVR → Vitrectomy is indicated
The anatomical success rate of initial surgery is reported to be 80–90% or higher in many studies, but the superiority between procedures depends on patient background (tear location, PVR, presence of intraocular lens, etc.)10, 14)
Many cases achieve final reattachment after multiple surgeries, but the duration of macular detachment and the presence of PVR greatly affect visual function prognosis7, 18)
Postoperative management and precautions for gas tamponade
After intravitreal gas tamponade, postural restriction (usually prone or head tilt) is required for several days to 2 weeks to keep the gas pressing against the retinal break. After the gas is absorbed, the intraocular cavity is refilled with fluid.
Gas type
Intraocular retention time
Expansion ratio
Approximate postural restriction period
Air
5–7 days
No expansion
3–5 days
20% SF₆
10–14 days
Approximately 2 times
5–10 days
14% C₃F₈
6–8 weeks
Approximately 4 times
10–14 days
Contraindications during the period when gas remains
Air travel / high-altitude climbing: Decreased external air pressure causes gas expansion, leading to a rapid increase in intraocular pressure and ocular circulatory disturbance (risk of blindness). Air travel is prohibited until the gas disappears, and ophthalmologic confirmation is mandatory before boarding.
MRI examination: Previously used gases were ferromagnetic, but currently used intraocular gases (SF₆, C₃F₈) are non-magnetic and pose low direct risk. However, the magnetic field environment during postural restrictions is a concern, so confirm with the attending physician during postoperative management.
Nitrous oxide (laughing gas) anesthesia: Nitrous oxide dissolves into intraocular gas, causing rapid gas expansion and increased intraocular pressure. During general anesthesia while gas remains, be sure to inform the anesthesiologist not to use nitrous oxide.
Periods of high risk for postoperative redetachment
Redetachment is often detected from the early postoperative period to several months, with PVR and new or missed retinal breaks being the main causes. Instruct patients to seek immediate medical attention if symptoms (increased floaters, reappearance of visual field defects) occur, and continue regular postoperative follow-up. 19, 22)
Management of Proliferative Vitreoretinopathy (PVR)
PVR is a serious complication of rhegmatogenous retinal detachment and the major cause of failure to achieve retinal reattachment. As a result of an excessive wound healing process of the detached retina, proliferative membranes composed of RPE cells, glial cells, fibroblast-like cells, and macrophages form on the retina, under the retina, and within the vitreous. Membrane contraction fixes the detached retina.
Occurs in 5–10% of cases postoperatively19)
Onset: begins 2–3 weeks after surgery, completes by 6–8 weeks
1983 Retina Society Classification (old classification): Grade A–D
Retina Society Classification (old classification, 1983)
Grade
Findings
A
Vitreous opacity (pigment clumps, pigment granules in the vitreous, pigment clumps on the retina)
In 1991, Machemer et al. proposed a new classification. The new classification considers anterior PVR and subretinal lesions, describing the extent of lesions using clock hours. 11)Rhegmatogenous retinal detachment with PVR often requires vitrectomy combined with removal of proliferative membranes, long-acting gas or silicone oil tamponade, and may require multiple surgeries. 7, 19)
In recent years, more facilities have chosen PPV as the initial treatment, leading to an increase in cases of anterior PVR. PVR developing after vitrectomy progresses rapidly and requires early reoperation.
The principle of treating tractional retinal detachment is to remove traction via vitrectomy. Proliferative membranes are managed using membrane peeling and vitreous scissors, with thorough endophotocoagulation and peripheral vitreous shaving. If a combined break is present, fluid-gas exchange is added following the approach for rhegmatogenous retinal detachment.
Preoperative anti-VEGF drug administration may be used in tractional retinal detachment surgery associated with proliferative diabetic retinopathy to regress neovascularization and reduce intraoperative bleeding. However, because contraction of fibrovascular membranes may worsen traction, careful judgment of surgical timing and indications is required. 5)
Treatment of exudative retinal detachment is primarily based on treating the underlying cause, and direct surgical reattachment of the retina is rarely performed. Inflammatory, vascular, and neoplastic causes should be identified, and appropriate medical and ophthalmic treatments selected accordingly. 21)
Cause
Main Treatment
Vogt-Koyanagi-Harada disease
Systemic corticosteroids are the mainstay; for recurrent or persistent cases, immunosuppressive agents may be considered (VKH is a representative inflammatory cause of exudative retinal detachment). 2, 21)
Rhegmatogenous retinal detachment is the most common type of retinal detachment and is one of the representative ophthalmic emergencies. The main subtypes include:
Flap tear (horseshoe tear) type: The retina is torn due to PVD. It accounts for about 30% of rhegmatogenous retinal detachments in phakic eyes, and causes rapid progression and high bullous detachment.
Atrophic hole type: A round hole due to atrophy within lattice degeneration. Common in young people and myopic eyes, presenting with low-lying localized detachment and slow progression.
Giant tear type: A tear of 90 degrees (1 quadrant) or more. Predisposed in high myopia with lattice degeneration. The tear edge rolls, and vitrectomy using liquid perfluorocarbon (PFC), which is heavier than water, is used for reattachment.
Macular hole type: More common in women with high myopia, accounting for about 5% of rhegmatogenous retinal detachments in Japan (higher than 0.5–2.0% in Western countries). Vitrectomy including internal limiting membrane (ILM) peeling is the standard procedure.
Proliferative diabetic retinopathy is the most common cause. Contraction of fibrovascular membranes containing new blood vessels leads to tent-shaped retinal detachment. Initially localized to the periphery, it causes rapid vision loss when it extends to the macula.
Retinopathy of prematurity (Stage 4/5): Traction from fibrovascular proliferative membranes in the peripheral retina extends to the posterior surface of the lens
Ischemic retinal diseases such as sickle cell disease, Eales disease, and retinal vein occlusion: traction from ischemic proliferative membranes7, 8)
Non-rhegmatogenous, non-tractional subretinal fluid accumulation. Shifting fluid with positional change is characteristic. In VKH, multiple bilateral dome-shaped detachments occur in the acute phase, and spontaneous resolution can be expected with appropriate immunosuppressive therapy. For neoplastic causes, tumor evaluation and treatment take priority.
Blunt trauma (ocular contusion) can lead to retinal detachment within weeks to months after injury, so long-term follow-up is essential.
Retinal Dialysis: A full-thickness tear along the ora serrata, often occurring after trauma in young males. It is commonly located in the inferotemporal quadrant and is often asymptomatic due to slow progression.
Choroidal Rupture and Retinal Concussion (Berlin Edema): Posterior pole edema and hemorrhage immediately after blunt trauma. Photoreceptor damage may be permanent.
In children, scleral buckling is preferred over adults because sutures hold well and the eye has high compliance. In particular, for ROP Stage 4A, encircling band is the first choice to reduce traction on proliferative membranes.
Since the silicone band used for buckling may become constrictive as the eye grows, removal within 6 months is recommended.
For tractional retinal detachment due to ROP, surgical indications should be considered at a specialized facility during Stage 4A. In Stage 4B/5, anatomical and visual outcomes tend to be poor, and decisions are made individually, including whether to preserve the crystalline lens. 13)
In Stickler syndrome, if genetic diagnosis is confirmed, 360° laser prophylactic coagulation is recommended.
Retinoschisis: The retina splits at the inner or outer plexiform layer. Unlike retinal detachment, there is no separation from the RPE. It is differentiated by OCT, fluorescein angiography, and ERG.
Association with glaucoma: In rhegmatogenous retinal detachment, Schwartz syndrome (secondary open-angle glaucoma due to outer segment debris) may occur; in retinal detachment with choroidal detachment, hypotony is observed. Exudative retinal detachment may be complicated by secondary glaucoma from the underlying cause.
Anatomical prognosis: With appropriate surgery, anatomical reattachment of the retina is achieved in over 95% of cases. The primary success rate is approximately 90% or higher, and the final reattachment rate including multiple surgeries reaches about 98%.
Functional prognosis (visual acuity)
Macular involvement
Visual acuity prognosis
Macula-on
Maintenance of vision close to preoperative visual acuity can be expected
Macula-off
Postoperative visual acuity is 0.5 or less in about half of cases, and visual field defects and metamorphopsia often remain
Improvement can be expected with treatment of the underlying disease, but if RPE atrophy or organic damage to photoreceptors occurs, visual recovery becomes incomplete. In VKH, early treatment of the first episode yields a good prognosis, but recurrent cases may develop chronic changes such as sunset glow fundus and Dalen-Fuchs nodules. In neoplastic exudative retinal detachment, tumor control determines the prognosis.
QHow soon after retinal detachment surgery can one return to daily life?
A
It depends on the surgical procedure and the presence of complications. With scleral buckling, hospitalization is about 1–2 weeks, and postural restrictions are almost unnecessary. With vitrectomy, postoperative gas tamponade requires postural restrictions (prone or lateral position) for several days to 2 weeks. While gas remains, avoid low-pressure environments such as air travel or mountain climbing. Visual recovery may take several months after retinal reattachment, especially in cases with macular detachment, requiring follow-up for 6 months to 1 year.
QI have high myopia. How often should I have regular checkups to prevent retinal detachment?
Retinal detachment in children is less common than in adults, but it is important that the underlying diseases differ. Hereditary diseases such as retinopathy of prematurity (ROP), familial exudative vitreoretinopathy (FEVR), Stickler syndrome, and Norrie disease are common, requiring different management from simple rhegmatogenous detachment. Pediatric eyes have high scleral elasticity, and scleral buckling surgery is often more effective than in adults. In ROP, tractional detachment is predominant, and surgery at Stage 4A is the best indication. The silicone band used for buckling must be removed within 6 months because it can cause constriction as the eye grows.
Flaxel CJ, Adelman RA, Bailey ST, Fawzi A, Lim JI, Vemulakonda GA, Ying GS. Posterior Vitreous Detachment, Retinal Breaks, and Lattice Degeneration Preferred Practice Pattern®. Ophthalmology. 2020;127(1):P146-P181. doi:10.1016/j.ophtha.2019.09.027. PMID:31757500.
Goto H, Mochizuki M, Yamaki K, et al. Epidemiological survey of intraocular inflammation in Japan. Jpn J Ophthalmol. 2007;51(1):41-44. doi:10.1007/s10384-006-0383-4.
Urner-Bloch U, Urner M, Stieger P, Galliker N, Winterton N, Zubel A, Moutouh-de Parseval L, Dummer R, et al. Transient MEK inhibitor-associated retinopathy in metastatic melanoma. Annals of oncology : official journal of the European Society for Medical Oncology. 2014;25(7):1437-1441. doi:10.1093/annonc/mdu169. PMID:24864047.
Zhao LQ, Zhu H, Zhao PQ, Hu YQ. A systematic review and meta-analysis of clinical outcomes of vitrectomy with or without intravitreal bevacizumab pretreatment for severe diabetic retinopathy. Br J Ophthalmol. 2011;95(9):1216-1222. doi:10.1136/bjo.2010.189514. PMID: 21278146; PMCID: PMC3161500.
Mackeen LD. Bilateral retinal detachment in preeclampsia. Am J Obstet Gynecol. 1997;177(4):948-949. 6)
Xiong J, Mehta N, Sandhu S, et al. A review of rhegmatogenous retinal detachment: past, present and future. Wien Med Wochenschr. 2025;175:146-160. PMCID: PMC12031774. 7)
Hayreh SS. Ocular vascular occlusive disorders: natural history of visual outcome. Prog Retin Eye Res. 2014;41:1-25. doi:10.1016/j.preteyeres.2014.04.001. PMID: 24769221. 8)
Akiba J. Prevalence of posterior vitreous detachment in high myopia. Ophthalmology. 1993;100(9):1384-8. doi:10.1016/s0161-6420(93)31471-5. PMID:8371928.
Yan X, Xu M, Su F. Surgical managements for rhegmatogenous retinal detachment: A network meta-analysis of randomized controlled trial. PloS one. 2024;19(11):e0310859. doi:10.1371/journal.pone.0310859. PMID:39541379; PMCID:PMC11563380.
Machemer R, Aaberg TM, Freeman HM, Irvine AR, Lean JS, Michels RM. An updated classification of retinal detachment with proliferative vitreoretinopathy. American journal of ophthalmology. 1991;112(2):159-65. doi:10.1016/s0002-9394(14)76695-4. PMID:1867299.
Denu RA, Nair S, Patel S, et al. Vogt-Koyanagi-Harada-Like Uveitis Secondary to Pembrolizumab in Metastatic Gastric Cancer: A Case Report and Review of the Literature. Case Rep Oncol. 2024;17(1):1071-1086. doi:10.1159/000541133. PMID: 39474530. 12)
Özdemir Zeydanlı E, Özdek Ş, Küçükbalcı T. Surgical Outcomes of Rhegmatogenous Retinal Detachment Associated with Regressed Retinopathy of Prematurity. Turk J Ophthalmol. 2024;54(4):223-227. doi:10.4274/tjo.galenos.2024.93464. PMID:39205437. PMCID:PMC11590703. 13)
Sultan ZN, Agorogiannis EI, Iannetta D, Steel D, Sandinha T. Rhegmatogenous retinal detachment: a review of current practice in diagnosis and management. BMJ Open Ophthalmol. 2020;5(1):e000474. doi:10.1136/bmjophth-2020-000474. PMID: 33083551. PMCID: PMC7549457.
Fawzi AA, Lee NG, Cheng L, et al. Recovery of photoreceptor outer segment length and the ellipsoid zone following surgery for rhegmatogenous retinal detachment. Br J Ophthalmol. 2011;95(4):570-573. 15)
Kim J, Ryu SY, Hong JH, Chung EJ. Incidence and risk factors for retinal detachment after cataract surgery in Korea: a nationwide population-based study from 2011 to 2015. Graefes Arch Clin Exp Ophthalmol. 2019;257(10):2193-2202. doi:10.1007/s00417-019-04423-x. PMID: 31388742. 17)
Schwartz SG, Flynn HW. Primary retinal detachment: scleral buckle or pars plana vitrectomy?. Curr Opin Ophthalmol. 2006;17(3):245-50. doi:10.1097/01.icu.0000193097.28798.fc. PMID:16794436. 18)
Pastor JC, de la Rúa ER, Martín F. Proliferative vitreoretinopathy: risk factors and pathobiology. Progress in retinal and eye research. 2002;21(1):127-44. doi:10.1016/s1350-9462(01)00023-4. PMID:11906814.
Wolfensberger TJ. The historical discovery of the retinal detachment. Doc Ophthalmol. 2003;107(1):1-5. 20)
Kunikata H, Nishida K. Long-term follow-up of vitrectomy for recurrent retinal detachment and established proliferative vitreoretinopathy. Jpn J Ophthalmol. 2001;45(6):626-631. 22)
Copy the article text and paste it into your preferred AI assistant.
Article copied to clipboard
Open an AI assistant below and paste the copied text into the chat box.