Optical Coherence Tomography (OCT) is a diagnostic imaging device that uses near-infrared light interference to non-invasively obtain cross-sectional images of the fundus and anterior segment of the eye. Its resolution is approximately 2–5 μm, about 100 times that of ophthalmic ultrasound. It enables high-resolution evaluation of the fine structures of the retina and optic nerve, aiding in early detection and monitoring of various eye diseases.
Introduced by Huang et al. in 1991, OCT rapidly spread in ophthalmology. Today, it is a standard examination for retinal diseases, glaucoma, anterior segment diseases, and neuro-ophthalmology. The insurance reimbursement is 187 points for three-dimensional fundus image analysis.
OCT has three main generations. Their characteristics are shown below.
TD-OCT (1st Generation)
Wavelength: 810 nm
Speed: 400 A-scans/sec
Axial resolution: Approximately 10 μm
The first-generation method uses a movable reference mirror to change the optical path length and acquire cross-sectional images. It has now been largely replaced by SD-OCT.
SD-OCT (2nd Generation)
Wavelength: 840 nm
Speed: 40,000–100,000 A-scans/sec
Axial resolution: 3–7 μm
The second-generation method uses a spectrometer and Fourier transform to acquire depth information all at once. It is the current clinical standard. It enables precise evaluation of the macula and optic nerve head. Representative models: Cirrus (Carl Zeiss), Spectralis (Heidelberg), RS-3000 (Nidek), 3D-OCT (Topcon).
SS-OCT (3rd Generation)
Wavelength: 1050 nm
Speed: 100,000–400,000 A-scans/second
Axial resolution: approximately 5 μm
Third-generation method using a swept-source laser and dual-balanced detector. The longer wavelength provides excellent visualization of deep structures such as the choroid. An advantage is that EDI-OCT is not required.
EDI-OCT (Enhanced Depth Imaging OCT): An imaging mode that sets the zero-delay line toward the choroid to visualize the choroid in detail. Also available with SD-OCT.
OCTA (OCT Angiography): A technique that detects brightness changes (decorrelation signals) between multiple B-scans to noninvasively visualize blood flow in vessels. It does not require contrast agents and is widely used as an alternative to fluorescein angiography (FA). The scan area can be selected from 3 mm × 3 mm to 12 mm × 12 mm.
Unified Nomenclature: The former “IS-OS layer” has been renamed the ellipsoid zone (EZ), and the junction between the outer segments and the RPE is now called the interdigitation zone (IZ) (IN-OCT nomenclature).
QIs OCT a painful test?
A
OCT is a noninvasive, non-contact test that is completely painless. Dilation eye drops may be needed, but the test only involves shining light and does not touch the cornea or retina. The examination usually takes only a few minutes.
Thin slices for fine structure confirmation (e.g., macular hole)
Radial scan
PCV polyp detection, evaluation of extrafoveal lesions
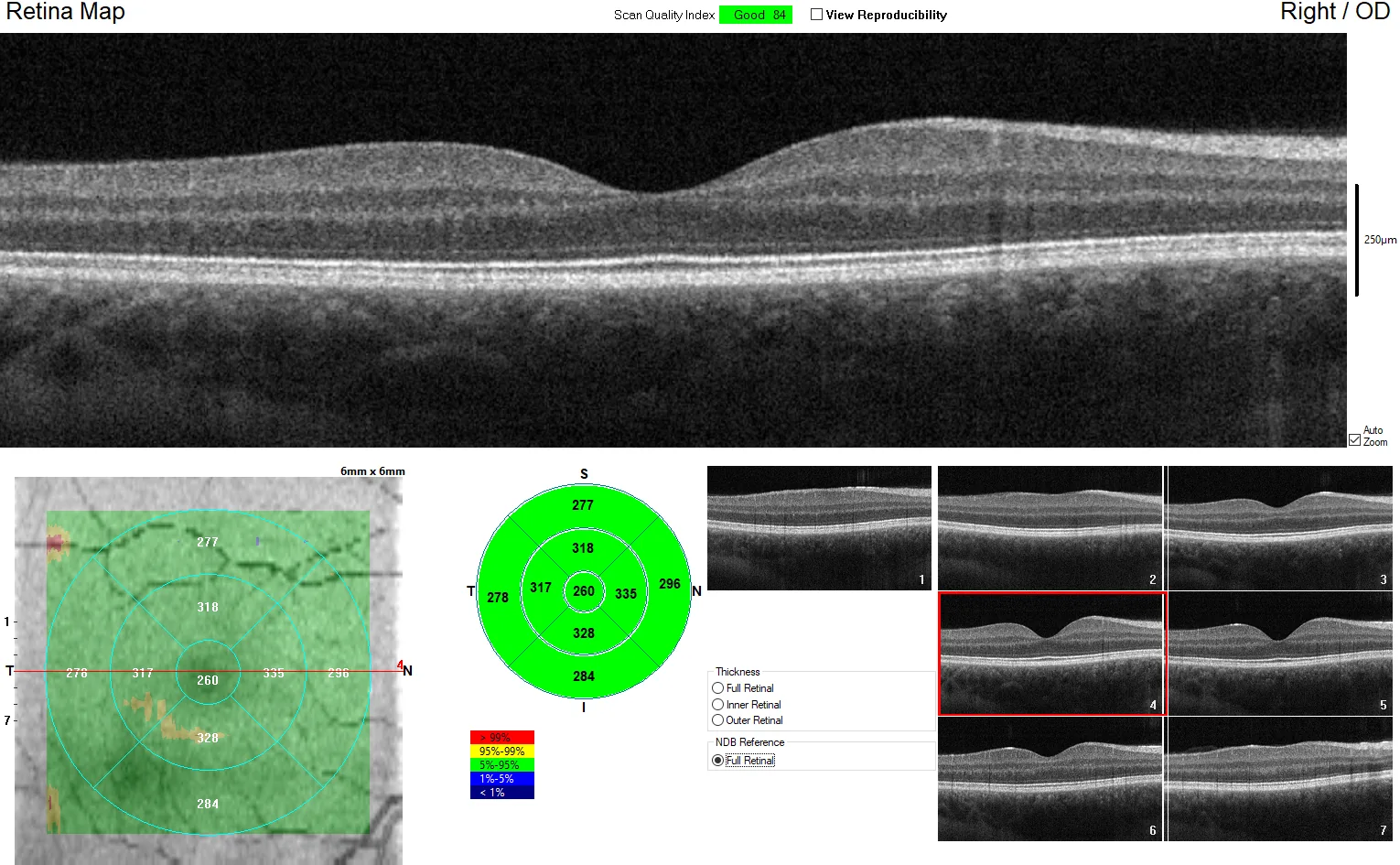
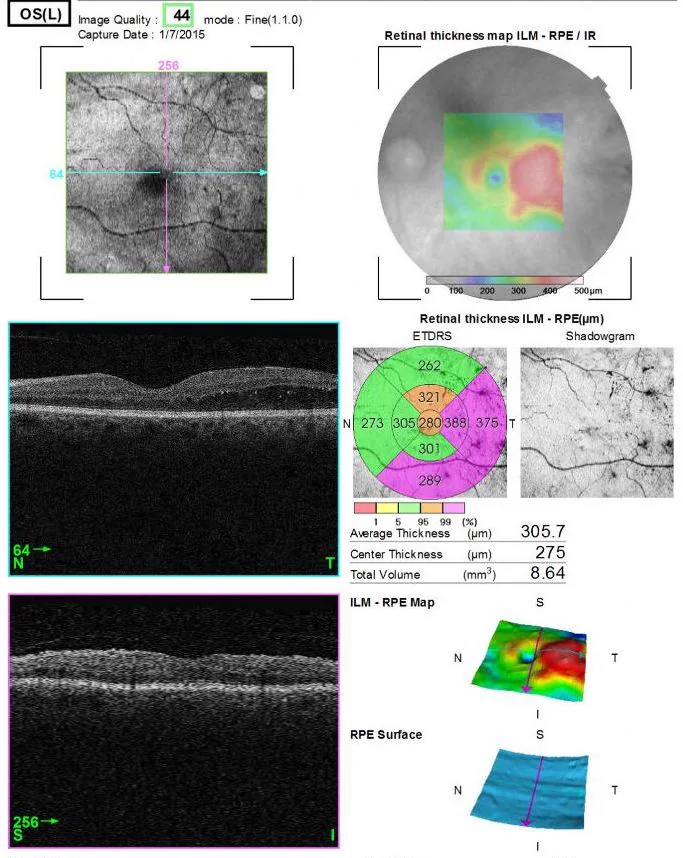
Macular map
Retinal thickness map. Treatment effect assessment for diabetic macular edema and RVO
Glaucoma analysis (cpRNFL/GCA)
RNFL thickness, GCL+IPL thickness. Glaucoma diagnosis and progression assessment
Imaging sites are broadly divided into posterior segment OCT (macula, peripapillary area, periphery) and anterior segment OCT (AS-OCT; cornea, anterior chamber, angle).
Fixate on the fixation light and align toward the pupil in front.
Start with a cross scan through the fovea.
Add a scan mode appropriate for the disease.
For poor fixation, use an external fixation light or have another person assist with fixation.
Mydriasis is generally not required, but in cases of moderate or greater cataract or small pupil, it is performed under dilation.
In foveal scans, it is important to visualize slices where the foveal depression is present and the inner retinal layers are not seen. In macular diseases, the center may shift due to poor fixation, and understanding the normal retinal structure leads to improved examination and diagnostic skills.
3. Indications and Findings in Retinal and Macular Diseases
Wies6014. Spectral Domain OCT - Macula Cross-Sections. Wikimedia Commons, 2013. Figure 1. Source ID: commons:File:Spectral_Domain_OCT_-_Macula_Cross-Sections.png. License: CC BY-SA 4.0.
Tomographic image (cross-section) of a healthy macula in a 24-year-old male captured by SD-OCT, visualizing the foveal depression and the normal 13-layer retinal structure from the internal limiting membrane (ILM) to the RPE/choroid. Corresponds to the normal retinal layer structure discussed in the section “Indications and Findings in Retinal and Macular Diseases.”
The normal layer structure on foveal scans (from inner to outer) consists of the following 13 layers:
Jmarchn. Macular edema LE Man 61years Diabetic. Wikimedia Commons, 2015. Figure 1. Source ID: commons:File:Macular_edema_LE_Man_61years_Diabetic.jpg. License: CC BY-SA 3.0.
OCT image of diabetic macular edema (DME) in the left eye of a 61-year-old patient with type 2 diabetes, confirming retinal thickening and cystoid spaces in the macula. Corresponds to the representative OCT findings of diabetic macular edema discussed in the section “Indications and Findings in Retinal and Macular Diseases.”
Macular hole is visualized as a full-thickness defect of the retina. SD-OCT is the most sensitive and specific test for diagnosing macular holes1).
Epiretinal membrane (ERM) is recognized as a hyperreflective layer on the internal limiting membrane2). Regarding postoperative visual acuity, it has been reported that 80% of cases achieve an improvement of two or more lines on the visual acuity chart after vitrectomy2).
Diabetic macular edema: Quantitative measurement of retinal thickness by OCT is an indicator for initiating and retreatment decisions for anti-VEGF therapy3). DRIL (Disorganization of Retinal Inner Layers) is important as a marker of poor visual prognosis.
RVO: OCT enables quantitative assessment of macular edema and detection of vitreoretinal interface changes4).
AMD: RPE detachment is classified into serous, fibrovascular, and drusenoid pigment epithelial detachment, and CNVM can be classified into type 1 (sub-RPE), type 2 (supra-RPE), and type 3 (retinal neovascularization)5).
Mirror artifact: Due to incorrect setting of the imaging range, the actual image is inverted and displayed overlapping.
Vignetting: Signal attenuation at the periphery. Depends on the incident angle of the illumination light.
Out-of-range error: Structures outside the set depth range are folded back and displayed.
Patient Factors
Blink artifact: Blinking during imaging causes horizontal gaps.
Eye movement: Poor fixation causes image misalignment or distortion.
Misalignment: Due to head position changes during scanning.
Software Factors
Segmentation error: The automatic layer segmentation algorithm misidentifies retinal layers. This occurs frequently in lesions, severe cataracts, or high myopia.
This can be addressed by manual correction or rescanning. If the signal strength index (SS) is less than 6, consider re-examination.
QAre there diseases that cannot be detected by OCT?
A
OCT has excellent diagnostic accuracy for diseases of the macula and posterior pole, but is not suitable for detecting peripheral retinal lesions (e.g., lattice degeneration, retinal tears). In addition, image quality and diagnostic reliability decrease when cataracts or vitreous opacities are severe. Wide-angle fundus photography or indirect ophthalmoscopy is used for peripheral lesions.
SD-OCT is a non-contact, non-invasive imaging technique that objectively evaluates structural damage in glaucoma, and its high utility in glaucoma diagnosis is recognized 6). It is particularly useful in diagnosing preperimetric glaucoma, as it can detect structural changes before visual field defects appear 6)7).
Measurement principle: Quantifies the thickness between the internal limiting membrane (ILM) and the RNFL boundary.
TSNIT map: Displays RNFL thickness on a 3.4 mm diameter circle centered on the optic nerve head, in the order T (temporal) → S (superior) → N (nasal) → I (inferior) → T (temporal).
Normal pattern: Shows a bimodal peak in the superior and inferior directions (reflecting the anatomical distribution of arcuate nerve fiber bundles) 6).
Glaucoma detection ability: Mean RNFL thickness has a sensitivity of 83% and specificity of 88% (at the 5% level). At the 1% level, specificity is 100% and sensitivity is 65%.
ONH Parameters
Optic nerve head analysis: Automatically delineates the optic disc, cup, and rim.
Bruch’s membrane reference: Defines the disc margin at the Bruch’s membrane opening and calculates the shortest distance to the ILM.
Indicators with high diagnostic ability: Vertical rim thickness, rim area, and vertical cup-to-disc ratio have the highest diagnostic performance 7).
BMO-MRW: Rim width assessment based on Bruch’s membrane opening with excellent reproducibility6)
Ganglion Cell Analysis (GCA)
Measurement target: Combined thickness of the ganglion cell layer (GCL) and inner plexiform layer (IPL) around the macula
Names by device: Cirrus: GCIPL (GCL+IPL), Optovue: GCC (RNFL+GCL+IPL)
Useful parameters: Minimum, inferotemporal sector, and average are most diagnostically useful6)7)
Floor effect: Macular parameters show floor effect later than RNFL thickness, useful for advanced stage assessment6)
Comparison with the normative database is useful, but attention must be paid to false positives and false negatives due to the following factors.
High myopia: Temporal shift of the RNFL bundle may cause normal eyes to be judged as “thinned”. The longer the axial length, the thinner the RNFL tends to be measured6)
Media opacity: Cataract leads to underestimation of RNFL thickness. Reports indicate RNFL thickness increases by 4.8–9.3% after cataract surgery
Segmentation errors: More likely in cases of tilted disc, scleral staphyloma, peripapillary atrophy, and epiretinal membrane
Eye movement and blinking: Can be improved with eye tracking function
There are two approaches for determining glaucoma progression: event analysis and trend analysis.
Event analysis: Progression is determined when follow-up measurements exceed a threshold from baseline.
Trend analysis: The rate of change over time (μm/year) is calculated using regression analysis to determine progression.
Cirrus GPA integrates both approaches7). The test-retest variability for average RNFL thickness is 3.89 μm, and a reproducible decrease of 4 μm or more suggests a statistically significant change.
In advanced glaucoma, RNFL thickness plateaus and rarely falls below 50 μm due to residual non-neural tissues such as glial tissue and blood vessels6)7). This “floor effect” reduces the clinical utility of SD-OCT in end-stage disease, making visual field testing the primary method for progression assessment. Macular parameters (GCIPL) exhibit a later floor effect than RNFL thickness, thus maintaining some utility even in advanced stages6).
QHow should SD-OCT evaluation be performed in highly myopic eyes?
A
In highly myopic eyes, comparison with a normative database has limitations. Because the RNFL bundle shifts temporally, it may be judged as “thinning” even in normal eyes. In such cases, longitudinal comparison using each patient’s own baseline is effective. Evaluate progressive thinning across a series of SD-OCT scans. Note that even in healthy individuals, RNFL thickness decreases by approximately 0.52 μm per year due to aging, so this natural decline must be considered.
OCT is rapidly expanding in neuro-ophthalmology9). Peripapillary RNFL (cpRNFL) thickness and macular GCIPL (ganglion cell layer + inner plexiform layer) are key parameters, and changes may be detected before the onset of obvious clinical signs or visual dysfunction9).
Optic neuritis and multiple sclerosis (MS): RNFL and GCIPL thinning are established biomarkers9). Even MS patients without ocular symptoms show cpRNFL reduction, and postmortem studies have confirmed optic nerve demyelination in 99% of MS patients. cpRNFL thickness correlates with best-corrected visual acuity, contrast sensitivity, color vision, and brain atrophy.
NMOSD is characterized by severe optic atrophy, and the frequency of microcystic macular edema is significantly higher (about 40% in AQP4-positive cases) than in MS (5%)9). In MOG-IgG-associated optic neuritis, GCIPL is relatively preserved, whereas in AQP4-IgG-associated optic neuritis, it is markedly lost9).
Optic disc drusen (ODD) detection: EDI-OCT is the gold standard9). ODD appears as a hyporeflective structure with a hyperreflective rim located above the lamina cribrosa, and has superior detection ability for buried drusen compared to B-scan ultrasound, autofluorescence, and CT. PHOMS (peripapillary hyperreflective ovoid mass-like structures) should be distinguished from ODD as a separate phenomenon9).
Compressive optic neuropathy: Preoperative RNFL thickness ≥70 μm is a significant predictor of postoperative visual acuity and visual field improvement9), and preoperative OCT evaluation is used for prognosis prediction.
Because segmentation algorithms and normative databases differ between devices, numerical comparisons between different devices are not possible. Use of the same device is recommended for longitudinal evaluation9).
OCT is based on the principle of the Michelson interferometer. Near-infrared light (wavelength 840–1050 nm) is split into a measurement beam and a reference beam, which are directed to the sample (fundus) and a reference mirror, respectively. The interference pattern (interferogram) generated when the reflected light from both is recombined is used to calculate the reflection intensity at each depth. The reflection intensity profile along the depth direction is called an A-scan, and a B-scan (tomographic image) is formed by arranging A-scans laterally.
TD-OCT (time-domain): A movable mirror on the reference arm is mechanically moved to sequentially change the optical path length, acquiring reflection intensity at each depth one by one. Due to speed limitations, clinical use is now largely obsolete.
SD-OCT (spectral-domain): The reference mirror is fixed, and the reflected light is spectrally dispersed by a diffraction grating or other spectrometer. By applying Fourier transform to the obtained spectrum, information from all depths is acquired simultaneously. Imaging speed is dramatically improved and noise is reduced.
SS-OCT (Swept-Source OCT): Combines a laser light source that rapidly sweeps wavelengths with a dual-balanced detector, and performs Fourier transform on the time-series acquired spectrum. By using a long wavelength near 1050 nm, penetration into the RPE and choroid is enhanced, making it excellent for visualizing deep structures.
OCTA: Repeats multiple B-scans at the same location and extracts brightness changes (decorrelation) between scans as blood flow signals. It can separate and display the superficial capillary plexus, deep capillary plexus, outer retina, and choriocapillaris by depth.
In glaucoma and optic nerve diseases, the following three layers are preferentially evaluated9).
RNFL (Retinal Nerve Fiber Layer): Contains the axons of retinal ganglion cells (RGCs).
GCL (Ganglion Cell Layer): Contains the cell bodies of RGCs.
IPL (Inner Plexiform Layer): Contains synapses between RGC dendrites and bipolar cell axons.
With RGC damage, the RNFL is lost. Approximately 50% of all RGCs are concentrated in the central 20° area of the macula, and even in early glaucoma, about 50% of RGCs may have disappeared6). SD-OCT evaluates the loss of RGC axons by RNFL thickness, and GCA evaluates thinning of the inner layers including cell bodies.
QWhat is the difference between SD-OCT and SS-OCT?
A
The main difference lies in the wavelength used and the ability to visualize deep structures. SD-OCT uses the 840 nm band, while SS-OCT uses the 1050 nm band. Since 1050 nm is less scattered by melanin pigment and penetrates the RPE more easily, SS-OCT is superior for observing the choroid and sclera. Additionally, the imaging speed of SS-OCT exceeds that of SD-OCT, making wide-angle scanning easier. On the other hand, axial resolution is about 5–7 μm for both, with no significant difference.
The high-speed, wide-angle scanning capability of SS-OCT at 1050 nm wavelength has advanced the evaluation of the pachychoroid disease spectrum. The assessment accuracy for central serous chorioretinopathy, polypoidal choroidal vasculopathy (PCV), and perifoveal telangiectasia, including choroidal thickening (pachydysm), has improved, contributing to the elucidation of pathology. Additionally, attempts are being made to evaluate tomographic images of wide areas including the peripheral retina in the same scan as the macula.
Automated diagnostic AI for glaucoma, AMD, and DME has been developed, and improvements in diagnostic accuracy have been reported. Deep learning-based OCT image analysis is enabling improved segmentation accuracy and automated report generation, which are being put into practical use6)7).
Longitudinal studies are needed to establish the usefulness of OCT as a screening and monitoring tool for neurodegenerative diseases such as Alzheimer’s disease and Parkinson’s disease9). RNFL and GCIPL thinning in patients with REM sleep behavior disorder (RBD) is attracting attention as a surrogate marker for prodromal Parkinson’s disease9).
Clinical application of ultra-high-resolution OCT, polarization-sensitive OCT, and adaptive optics OCT
Improvement of longitudinal comparison accuracy through inter-device standardization6)7)
Simultaneous evaluation of structure and blood flow by integration with OCTA
Incorporation of OCT into MS diagnostic criteria (McDonald criteria): In the current criteria (2017 revision), the optic nerve is not listed as a DIS site, but improved sensitivity by incorporating asymptomatic optic nerve lesions has been reported, and research is underway to expand its use for proving DIS and DIT in future revisions9)
Flaxel CJ, Adelman RA, Bailey ST, Fawzi A, Lim JI, Vemulakonda GA, et al. Idiopathic Macular Hole Preferred Practice Pattern®. Ophthalmology. 2020;127(2):P184-P222. doi:10.1016/j.ophtha.2019.09.026. PMID:31757499.
Flaxel CJ, Adelman RA, Bailey ST, Fawzi A, Lim JI, Vemulakonda GA, et al. Idiopathic Epiretinal Membrane and Vitreomacular Traction Preferred Practice Pattern®. Ophthalmology. 2020;127(2):P145-P183. doi:10.1016/j.ophtha.2019.09.022. PMID:31757497.
Lim JI, Kim SJ, Bailey ST, et al. Diabetic Retinopathy Preferred Practice Pattern. Ophthalmology. 2025 Apr;132(4):P75-P162. doi:10.1016/j.ophtha.2024.12.020. PMID:39918521.
Kovach JL, Bailey ST, Kim SJ, Lim JI, Vemulakonda GA, Ying GS, et al. Retinal Vein Occlusions Preferred Practice Pattern®. Ophthalmology. 2025;132(4):P303-P343. doi:10.1016/j.ophtha.2024.12.025. PMID:39918523.
Vemulakonda GA, Bailey ST, Kim SJ, Kovach JL, Lim JI, Ying GS, et al. Age-Related Macular Degeneration Preferred Practice Pattern®. Ophthalmology. 2025;132(4):P1-P74. doi:10.1016/j.ophtha.2024.12.018. PMID:39918524.
Gedde SJ, Vinod K, Wright MM, et al. Primary Open-Angle Glaucoma Preferred Practice Pattern. Ophthalmology. 2021 Jan;128(1):P71-P150. doi:10.1016/j.ophtha.2020.10.022. PMID:34933745.
Gedde SJ, Lind JT, Wright MM, Chen PP, Muir KW, Vinod K, Li T, Mansberger SL; American Academy of Ophthalmology Preferred Practice Pattern Glaucoma Panel. Primary Open-Angle Glaucoma Suspect Preferred Practice Pattern. Ophthalmology. 2021 Jan;128(1):P151-P192. doi:10.1016/j.ophtha.2020.10.023. PMID:33189698.
Lo C, Vuong LN, Micieli JA. Recent advances and future directions on the use of optical coherence tomography in neuro-ophthalmology. Taiwan journal of ophthalmology. 2021;11(1):3-15. doi:10.4103/tjo.tjo_76_20. PMID:33767951; PMCID:PMC7971436.
Copy the article text and paste it into your preferred AI assistant.
Article copied to clipboard
Open an AI assistant below and paste the copied text into the chat box.