Vitreomacular traction syndrome (VMT) is a vitreoretinal interface disease that develops based on incomplete posterior vitreous detachment (PVD). With aging, the vitreous in front of the macula liquefies and forms a vitreous pocket, but the vitreous cortex present in front of the macula acts as anteroposterior traction due to the progression of posterior vitreous detachment. The posterior vitreous cortex remains abnormally strongly attached to the macula, and the liquefied vitreous pulls the macular attachment site anteroposteriorly, causing morphological and functional changes. When the progression of posterior vitreous detachment stops near the macula, the posterior wall of the posterior vitreous cortex pocket pulls the macula anteroposteriorly, leading to the onset.
It refers to cases where traction causes morphological changes in the retina; cases with no retinal changes or where the vitreous is merely adherent to the macula are considered vitreomacular adhesion (VMA) and are not included in the category of VMT.
VMT includes narrow (idiopathic) type caused by age-related changes in the vitreous, and broad (secondary) type that occurs secondary to uveitis, proliferative diabetic retinopathy, branch retinal vein occlusion, and other retinal vascular diseases.
In 1953, Irvine first reported a related condition as “vitreous tag syndrome,” and in 1967, Jaffe proposed “vitreoretinal traction syndrome” as an independent disease. Later, the disease concept was established through histopathological studies by Reese et al.
The prevalence of isolated VMT is reported to be 22.5 per 100,000 population 1). The prevalence of VMT associated with diabetic retinopathy, diabetic macular edema, and age-related macular degeneration is much higher. VMT can occur at any age and in all races, but aging is the greatest risk factor, with an estimated prevalence of 0.4–2.0% in US adults aged 63 years and older 2). There is a slight tendency for higher incidence in women.
Approximately 80% of cases are accompanied by cystoid macular edema, and most cases are accompanied by an epiretinal membrane. The presence of an epiretinal membrane further strengthens the adhesion between the vitreous and the macula, leading to persistent traction over a long period.
Distinction between vitreomacular adhesion (VMA) and VMT
With the widespread use of OCT, the International Vitreomacular Traction Study Group (IVTS) has proposed OCT-based definitions and classifications.
Vitreomacular adhesion (VMA) is a condition in which there is partial vitreous attachment near the fovea, but no change in retinal morphology. It is often asymptomatic, and VMA alone is not a treatment target.
Vitreomacular traction (VMT) is a condition in which, in addition to VMA, there are changes in foveal morphology (such as distortion of the foveal surface, pseudocyst formation, or elevation of the fovea from the RPE). The absence of a full-thickness macular hole is a necessary condition for VMT.
According to the IVTS classification, cases with an adhesion diameter of 1500 µm or less are classified as focal, and those exceeding 1500 µm as broad. The adhesion width is continuous, ranging from very small pinpoint adhesions to broad adhesions exceeding 1500 µm 8).
Classification by adhesion width:
Classification
Adhesion width
Main features
Focal
≤ 1500 µm
Tends to be associated with cystoid changes. More likely to resolve spontaneously.
VMA is a condition where the vitreous is attached to the macula but the retinal morphology is normal, often asymptomatic and requiring no treatment. VMT is a condition where, in addition to VMA, morphological changes in the retina (distortion, pseudocyst, elevation) occur, which can lead to visual dysfunction. The two are distinguished by OCT examination. Only those with morphological changes in the retina due to traction are diagnosed as VMT, while those with only vitreous adhesion to the macula are distinguished as VMA.
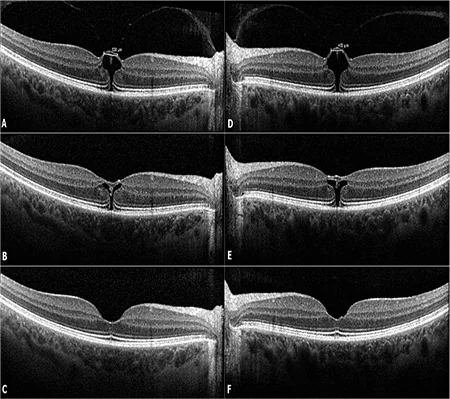
Özdemir HB, et al. Pneumatic Vitreolysis for the Treatment of Vitreomacular Traction Syndrome. Turk J Ophthalmol. 2019. Figure 1. PMCID: PMC6761384. License: CC BY.
Vitreomacular traction (VMT) observed on OCT of the right eye (A) and left eye (D) was released by pneumatic vitreolysis in the right eye (B) after 3 days and in the left eye (E) within 2 days, with recovery of normal retinal structure at 1 month (C, F). This corresponds to the vitreomacular traction discussed in the section “2. Main Symptoms and Clinical Findings”.
Slit-lamp biomicroscopy reveals vitreous adherent to the macula with surrounding posterior vitreous detachment. A taut, semitransparent membrane attached to the fovea may be observed. Fundus findings may include an epiretinal membrane, central serous chorioretinopathy-like macular detachment or edema, or macular hole-like appearance. Ophthalmoscopically, a transparent membrane on the macular retina may be seen, and retinal vessels may be tortuous due to traction.
The main findings confirmed by OCT are shown below.
VMT Findings
Loss/deformation of foveal depression: The normal concave shape of the fovea becomes flattened or distorted.
Pseudocyst/cystoid changes: Fluid accumulation within the macula with tissue pillars representing Müller cells. Present in 81% of VMT eyes. Cystoid changes can involve the entire macula and are attributed to the anteroposterior traction characteristic of VMT, unlike the tangential traction of ERM8).
Elevation of the fovea from the RPE: Direct evidence of anterior traction by the posterior vitreous cortex.
Thickening/hyperreflectivity of the posterior vitreous cortex: Visualized as a hyperreflective band located anterior to the retina.
Associated Findings
Epiretinal membrane (ERM): Present in 40–65% of VMT eyes. The presence of an ERM prevents spontaneous resolution of VMA and enhances traction 8).
Tractional macular schisis/macular detachment: Occurs in severe cases.
Full-thickness macular hole: The most severe complication. Continued traction can progress to a macular hole.
Fluorescein angiography may show macular hyperfluorescence, cystoid macular edema, and leakage at the optic disc. If posterior vitreous detachment is present at the disc, disc leakage does not occur. On FA, dye leakage from capillaries may be seen in the late phase, with dye pooling in cystoid spaces 8).
Yamada and Kishi reported two types of vitreous traction profiles in VMT. The V-shaped type (detachment both temporal and nasal to the fovea, with attachment only at the fovea) has good postoperative outcomes, while the J-shaped or arcuate type (residual attachment also nasal to the fovea) tends to have poor outcomes due to progression to macular hole or atrophy postoperatively.
In VMT/ERM eyes, vitreopapillary traction (VPT) may be present, where the vitreous remains attached around the optic disc. VPT is diagnosed by OCT and may be confused with disc edema or, in bilateral cases, papilledema. VPT has been suggested to be associated with visual loss and ischemic optic neuropathy8).
QWhat is the risk of progression from VMT to macular hole?
A
If traction persists, it may progress to a full-thickness macular hole. There are reports of cases leading to severe vision loss (hand motion level). On the other hand, if it is focal and not associated with an epiretinal membrane, spontaneous release may occur, so observation or surgical intervention is chosen based on the severity of symptoms and findings. Since a macular hole may develop during observation, regular OCT follow-up is important.
With aging, the vitreous gel undergoes liquefaction (synchysis) and condensation (syneresis), leading to posterior vitreous detachment (PVD). In normal PVD, the vitreous detaches uniformly from the retina, but in anomalous PVD, detachment and adhesion release occur asynchronously, resulting in VMT.
The vitreous is most firmly attached to the retina at the thinnest part of the internal limiting membrane (ILM). Posteriorly, attachment is strong around the optic disc, macula (fovea and perifoveal area within 1500 µm diameter), and along major retinal vessels. This provides the anatomical basis for persistent foveal attachment in VMT.
Medication (pilocarpine): Bilateral VMT cases have been reported with pilocarpine 1% eye drops 1). Pilocarpine may cause anterior movement of the vitreous base via ciliary muscle contraction, enhancing anteroposterior traction in eyes with pre-existing VMA. Cases of traction release with persistent VMA after pilocarpine discontinuation have also been reported 1).
This test plays a central role in the diagnosis and evaluation of VMT. OCT is considered the de facto standard for diagnosing, classifying, and monitoring ERM and VMT 8). It noninvasively visualizes the vitreomacular interface, allowing detailed observation of the width of traction and retinal changes. The following OCT findings are required for the diagnosis of VMT.
Vitreous attachment within 3 mm of the fovea in the macular region
Acute angle between the posterior hyaloid membrane and the retinal surface
Changes in foveal contour or retinal morphology (e.g., deformation of the foveal surface, intraretinal structural changes such as pseudocyst formation, elevation of the foveal retina from the retinal pigment epithelium)
Assessment of whether the attachment width is ≤1500 µm (focal) or >1500 µm (broad) is important for determining treatment strategy. SD-OCT can also evaluate the status of the outer retinal layers (external limiting membrane, photoreceptor ellipsoid zone) and is useful for prognosis prediction.
The “cotton ball sign” (a round or diffuse hyperreflective area between the inner segment/outer segment junction and the photoreceptor terminal at the foveal center) may be an indicator of anterior traction on the fovea.
Using a fundus contact lens or high-magnification indirect ophthalmoscopy, the macula is evaluated for puckering, edema, and tractional changes. Slit-lamp fundus examination confirms the vitreous adherent to the macula and the surrounding posterior vitreous detachment.
Clinical diagnosis is possible with slit-lamp fundus examination and fluorescein angiography, but the standard for definitive diagnosis of VMT is OCT. OCT allows detailed evaluation of traction width, retinal morphological changes, and associated findings, and is essential for determining treatment strategy. In particular, accurate assessment of adhesion width (focal vs. broad) is only possible with OCT.
For cases where symptoms are mild and the risk of VMT release is considered to outweigh the benefits, observation is the first choice. Spontaneous resolution is reported in 11–40% of cases in meta-analyses 3). For focal VMT (≤1500 µm), spontaneous resolution is reported in 23–47% over 1–2 years 8). Focal VMT without epiretinal membrane tends to resolve spontaneously 3).
Cases with minimal retinal changes may remain unchanged for years, while those with small adhesion points may detach spontaneously. Therefore, it is necessary to closely monitor the type and course. In cases without epiretinal membrane, spontaneous posterior vitreous detachment may occur, releasing the traction. For patients without strong subjective symptoms, observation for a period is acceptable. Regular OCT follow-up is required to monitor progression to macular hole.
On the other hand, eyes with cystoid changes at baseline require caution regarding prognosis. In a study of 53 eyes, 81% of eyes with cystoid changes showed a visual acuity decline of 2 lines or more at 60 months 8).
This is the most reliable method for treating VMT. Simple vitrectomy and macular membrane peeling are performed. Adhesion at the macula is strong, so it is removed slowly while observing the retinal attachment. In most cases, vitrectomy is indicated to release vitreous traction on the macula.
Once the diagnosis is clear, early surgery is recommended before the development of macular hole or irreversible changes. Particular caution is needed in cases with extensive vitreoretinal adhesion, as the adhesion is strong. If a macular hole develops during observation or if surgery is delayed, postoperative cystoid macular edema may lead to a macular hole.
Indications for surgery:
Severe subjective symptoms (metamorphopsia or visual impairment affecting daily life)
High risk of irreversible progression over long-term course
The best treatment outcomes have been reported, with VMT release rate of 100% and macular hole closure rate of 95% 2). In systematic reviews and meta-analyses, vitrectomy was significantly superior to ocriplasmin (enzymatic vitreolysis) in VMT release rate (RR=0.48, 95% CI 0.38–0.62) and macular hole closure rate (RR=0.49, 95% CI 0.30–0.81) 2). Postoperative visual improvement was also greater than with ocriplasmin (SMD=0.38, 95% CI 0.03–0.73) 2).
Postoperative visual acuity after PPV improved from preoperative logMAR 0.67 to 0.42 in a meta-analysis (259 eyes), with 33% improving by 2 or more lines, while 21% remained unchanged or worsened 8). On average, about 80% of patients gain 2 or more lines of visual improvement 8).
When complicated by epiretinal membrane or macular hole, internal limiting membrane (ILM) peeling is standard. ILM is stained with brilliant blue dye or other dyes and peeled. In cases with macular hole, the closure rate after ILM peeling with C3F8 gas tamponade is over 95% 4). A systematic review (13 studies) found no significant difference in visual outcomes with or without ILM peeling, but ILM peeling reduced ERM recurrence rate 8). A recent RCT (213 eyes) showed a recurrence rate of 0% in the active ILM peeling group versus 19.6% in the non-peeling group 8).
In a report of an 83-year-old man with VMT complicated by macular hole (grade 1b), a full-thickness macular hole (422 µm) developed after posterior vitreous cortex detachment during vitrectomy, but a second vitrectomy with ILM peeling (brilliant blue dye) and 14% C3F8 gas tamponade improved vision to 20/120 and restored foveal morphology at 6 weeks 4).
Preoperative anatomical morphology affects surgical outcomes. Focal VMT (V-shaped traction profile) tends to have greater postoperative visual improvement than broad or J-shaped traction 4).
This is a minimally invasive treatment in which an expansile gas such as C3F8 (perfluoropropane) or SF6 (sulfur hexafluoride) is injected into the vitreous cavity to release VMT through gas buoyancy and mechanical force. C3F8 is used at 0.3 mL.
“Drinking bird maneuver”: a postoperative technique of repeatedly tilting the head forward and backward to promote mixing of the gas bubble and vitreous fluid, improving the VMT release rate.
Meta-analysis showed that PV had a significantly higher VMT release rate compared with ocriplasmin (RR=0.49, 95% CI 0.35–0.70), and no significant difference in visual improvement compared with PPV2). VMT release rates were reported as 46% (ocriplasmin), 68% (PV), and 100% (vitrectomy) 2).
In a DRCR Network RCT, macular VMT was released in 78% of the C3F8 gas injection group versus 9% in the sham group. However, the incidence of retinal detachment and tears was unexpectedly higher in the gas injection group, leading to early termination due to safety concerns 8). Caution is still needed regarding the safety of this treatment.
Ocriplasmin is a recombinant protease with activity against fibronectin and laminin, which are components of the vitreoretinal interface. A single intravitreal injection of 125 µg promotes VMA resolution. Its efficacy is not very favorable, with effectiveness reported in about 20% of cases.
In the MIVI-TRUST and OASIS clinical trials, the VMA resolution rate was significantly superior to placebo (RR=3.61, 95% CI 1.99–6.53)3), but the VMT resolution rate was inferior compared to vitrectomy. In Phase III (MIVI-TRUST), VMA resolution was achieved in 27% of the ocriplasmin group versus 10% in the placebo group (P<0.001)7). The use of ocriplasmin is controversial and has not been widely adopted in clinical practice7). It was withdrawn from the market in 20205), and availability varies by region and facility.
QIs ocriplasmin still available for use?
A
Ocriplasmin (Jetrea) is a pharmacological vitreolysis agent approved by the US FDA in 2012, and is recommended by NICE guidelines for cases without epiretinal membrane and with macular hole diameter ≤400 µm. However, it was withdrawn from the market in 2020, and availability varies by region and facility. Its VMT resolution rate is inferior to vitrectomy, and there are concerns about its side effect profile. See the section “Latest Research and Future Prospects” for details.
Age-related changes in the vitreous progress in the following order.
Synchysis: Aggregation of collagen fibers and separation from hyaluronic acid lead to the formation of liquid pockets within the vitreous.
Syneresis: Volume reduction due to liquefaction causes traction on retinal attachment sites through the condensed posterior vitreous cortex.
Progression of posterior vitreous detachment (PVD): Detachment proceeds in the order: perifoveal (temporal to nasal) → superior and inferior vascular arcades → fovea → mid-periphery → optic disc.
When PVD progresses normally, separation between the vitreous and retina occurs evenly. However, in “abnormal PVD” where traction and detachment are asynchronous, adhesion at the fovea persists until the end, resulting in VMT.
The smaller the adhesion diameter, the higher the traction stress per unit area, leading to greater foveal deformation 5).
Focal type (approximately 500 µm adhesion): Prone to elevation and traction of the foveal neurosensory retina and intraretinal cystoid changes 5).
Broad type (approximately 1500 µm adhesion): Causes broader macular elevation, sometimes with macular retinal detachment. Intraretinal cystoid changes are less common compared to the focal type 5).
When PVD is incomplete, the elastic properties of the remaining posterior vitreous exert static anterior traction on the fovea. Additionally, dynamic traction from eye movements adds to this, with dynamic traction considered more important than static traction in VMT. Severe cases may involve retinoschisis or retinal detachment.
Epiretinal membrane is present in 40–65% of VMT eyes and exacerbates VMT through two mechanisms 5).
Short-term: Strengthens vitreomacular adhesion and prevents spontaneous detachment.
Long-term: Adds anterior traction through proliferation and contraction of fibrous cells.
Histopathologically, ERM contains vitreous collagen, and the firm attachment of ERM to the ILM plays a role in fixing residual vitreous adhesion to the macula8).
Regarding the mechanism of ERM formation, in addition to the conventional theory that RPE cells and glial cells migrate to the retinal surface through microbreaks in the ILM, a new hypothesis has been proposed that residual cells of the posterior vitreous cortex are activated into myofibroblasts, leading to membrane formation and contraction without requiring ILM breaks 8).
Histologically, even in cases where no epiretinal membrane is observed ophthalmoscopically, cells centered on myofibroblasts are attached to the vitreous side of the internal limiting membrane. In cases with membranous tissue, it has been reported that myofibroblasts and fibrous astrocytes are contained within the tissue, similar to idiopathic epiretinal membrane.
Histopathology of VMT specimens shows fibrocellular proliferation consisting of fibrous astrocytes, myofibroblasts, fibrocytes, and RPE cells, forming a “double membrane” that bridges the posterior vitreous interface and the retinal interface. Two types of epiretinal membranes are identified by transmission electron microscopy. The presence or absence of vitreoschisis is thought to determine these two types.
7. Latest Research and Future Perspectives (Research Stage Reports)
Ocriplasmin (Jetrea; 125 µg single intravitreal injection) is a recombinant protease consisting of the catalytic domain of human plasmin, which promotes VMA resolution by dissolving protein components at the vitreoretinal interface.
In a meta-analysis by Chen et al. (55 studies, 4,159 cases), ocriplasmin treatment was significantly superior to placebo in VMA resolution rate at 28 days (RR=3.61, 95% CI 1.99–6.53), macular hole closure rate (RR=3.84, 95% CI 1.62–9.08), and ≥3-line BCVA improvement at 6 months (RR=1.97, 95% CI 1.08–3.57) 3). Pooled analysis of cohort studies showed VMA resolution rate of 50% (95% CI 47–53%) and macular hole closure rate of 36% (95% CI 32–39%) 3).
Predictors of treatment effect (ocriplasmin):
Absence of epiretinal membrane is associated with higher treatment efficacy (VMA resolution rate: 58% without ERM, 34% with ERM) 3)
Cases with macular hole (MH) have a higher VMA resolution rate (58%) 3)
VMA diameter <506 µm, age <73 years, female sex tend to have higher VMA release rate 3)
Phase III subgroup analysis showed higher VMA release rate in patients aged <65 years, without ERM, phakic, and VMA ≤1500 µm 7)
In a Cochrane review, up to 20% of the treatment group required additional PPV within 6 months 7). The use of ocriplasmin is controversial and has not achieved widespread clinical adoption 7). Since its market withdrawal in 2020, availability is limited 5).
In a systematic review and meta-analysis by Quiroz-Reyes et al. (2023), randomized trials comparing PPV and gas injection (PV) showed that PPV was superior in VMT release rate and macular hole closure rate, but there was no significant difference in postoperative BCVA improvement (SMD = -0.15, 95% CI -0.47 to 0.16) 2). There have been cases where an RCT of PV with C3F8 was terminated early due to safety concerns (retinal detachment, retinal tear) 2, 8), and the safety of this treatment requires ongoing evaluation.
A meta-analysis comparing simultaneous phacovitrectomy and staged surgery found no significant differences in complications, visual acuity, or refractive outcomes 8). Since nuclear cataract frequently progresses after PPV in phakic eyes, it is recommended to discuss the indication for simultaneous surgery with the patient preoperatively.
Ashby et al. reported a case of a 66-year-old woman whose VMT resolved after a flight simulator experience (2025) 5). It is hypothesized that multidirectional forces from the simulator’s three-dimensional acceleration contributed to separation at the VMA interface. Visual acuity improved from 20/60 to 20/25 at long-term follow-up. However, impending macular hole findings were transiently observed after VMT release, indicating that full-thickness macular hole formation is a potential risk 5). A temporal association with spontaneous VMT resolution cannot be ruled out, and this is not an established treatment.
Rios Gonzalez et al. reported a case of a 69-year-old man who developed bilateral VMT 6 weeks after starting 1% pilocarpine eye drops (for glaucoma treatment), and VMT resolved with persistent VMA 8 weeks after discontinuation (2023)1). With the spread of new pilocarpine formulations (1.25%, etc.) for presbyopia treatment, there is concern about the risk of inducing or exacerbating VMT, and it has been proposed to perform posterior segment examination and OCT before starting treatment in cases with incomplete PVD1).
Current Status and Challenges of Patient-Reported Outcomes (QOL Assessment)
A systematic review of patient-reported outcome measures (PROMs) in vitreomacular interface diseases (VMID) identified 17 types of VMID-specific PROMs from 86 studies, but current PROMs have the following issues6):
Limited content coverage and insufficient or unverified psychometric quality
NEI VFQ-25 is most commonly used, but concurrent validity in VMID shows mixed results; the color vision scale has a small effect size, while the near vision scale shows relatively good responsiveness6)
None of the PROMs have been validated by Rasch analysis, so interval scaling is not guaranteed6)
Patient consultation was not conducted during the development of VMID-specific PROMs (failing to meet FDA and EMA requirements)
Overlap between PROMs and QOL issues identified in qualitative studies was limited to only 9 items (reading, driving, night driving, fear of surgery, metamorphopsia, diplopia, concerns about communication with healthcare providers, inconvenience of posturing, and sleep disturbance due to posturing)6). QOL issues reported by patients with VMID include visual problems such as metamorphopsia, central vision impairment, and reading difficulty, as well as emotional well-being (optimism, frustration, anxiety, stress, hope), social well-being (obtaining social support, maintaining interactions with friends and family), and coping strategies (ignoring, distraction, trust in doctors, prayer/meditation, acceptance, practical tools, social support, symptom monitoring). Current PROMs do not adequately cover these aspects6). In the future, development of VMID-specific PROMs through patient-participatory content development and rigorous psychometric validation including Rasch analysis is needed.
QIs there a prospect of establishing less invasive treatments in the future?
A
Pharmacologic vitreolysis (ocriplasmin) and gas injection (pneumatic vitreolysis) continue to be studied as minimally invasive treatments with low postoperative management burden. However, at present, the rates of VMT release and macular hole closure are lower than those of vitrectomy, and the effect is limited, especially in cases of broad VMT or concurrent epiretinal membrane. Optimal treatment selection based on individual patient characteristics (adhesion width, presence of epiretinal membrane, symptom severity, patient QOL assessment) is expected to be further refined in the future. Standardization of patient-reported outcomes (PROs) is also an important research topic for appropriate evaluation of treatment efficacy.
Rios Gonzalez R, Villegas VM, Blasini M. Bilateral vitreomacular traction syndrome associated with topical pilocarpine 1% ophthalmic solution. American journal of ophthalmology case reports. 2023;30:101834. doi:10.1016/j.ajoc.2023.101834. PMID:37181418; PMCID:PMC10172709.
Quiroz-Reyes MA, Quiroz-Gonzalez EA, Quiroz-Gonzalez MA, Lima-Gomez V.. Pneumatic vitreolysis versus vitrectomy for the treatment of vitreomacular traction syndrome and macular holes: complication analysis and systematic review with meta-analysis of functional outcomes. Int J Retina Vitreous. 2023;9(1):33. doi:10.1186/s40942-023-00472-x. PMID:37316932; PMCID:PMC10268451.
Chen X, Li M, You R, Wang W, Wang Y. Efficacy and Safety of Ocriplasmin Use for Vitreomacular Adhesion and Its Predictive Factors: A Systematic Review and Meta-Analysis. Frontiers in medicine. 2021;8:759311. doi:10.3389/fmed.2021.759311. PMID:35096864; PMCID:PMC8793778.
Tayyab M, Iqbal K, Abid MA, Ur Rahman F, Tayyab HA.. Surgical Outcome of Vitreomacular Traction Associated With Macular Hole. Cureus. 2022;14(12):e32620. doi:10.7759/cureus.32620. PMID:36654612; PMCID:PMC9841474.
Ashby N, Kaftan T, Ohlhausen M, Kim S, McGill E, Yeh S. Resolution of Vitreomacular Traction Following a Commercial Flight Simulator Experience. Journal of vitreoretinal diseases. 2025;9(6):24741264251366407. doi:10.1177/24741264251366407. PMID:40881458; PMCID:PMC12373645.
Woudstra-de Jong JE, Busschbach JJ, Manning-Charalampidou SS, Vingerling JR, Pesudovs K. Assessment of patient-reported outcomes in vitreomacular interface disorders: A systematic literature review. Surv Ophthalmol. 2024. doi:10.1016/j.survophthal.2024.08.004.
Flaxel CJ, Adelman RA, Bailey ST, Fawzi A, Lim JI, Vemulakonda GA, Ying GS. Idiopathic Epiretinal Membrane and Vitreomacular Traction Preferred Practice Pattern®. Ophthalmology. 2020;127(2):P145-P183. doi:10.1016/j.ophtha.2019.09.022. PMID:31757497.
Bailey ST, Vemulakonda GA, Kim SJ, Kovach JL, Lim JI, Ying GS, Flaxel CJ, American Academy of Ophthalmology Preferred Practice Pattern Retina/Vitreous Committee. Idiopathic Epiretinal Membrane and Vitreomacular Traction Preferred Practice Pattern®. Ophthalmology. 2025;132(4):P197-P233. doi:10.1016/j.ophtha.2024.12.019. PMID:39918520.
Copy the article text and paste it into your preferred AI assistant.
Article copied to clipboard
Open an AI assistant below and paste the copied text into the chat box.