Posterior vitreous detachment (PVD) is a condition in which the posterior vitreous cortex detaches from the retina due to age-related or pathological changes. It refers to the separation of the posterior vitreous cortex from the ILM (internal limiting membrane), and accurate diagnosis of PVD is important for determining the prognosis of vitreoretinal diseases and surgical indications.
It is widely recognized as a physiological phenomenon associated with aging and is the most common cause of “floaters,” one of the most frequent complaints in ophthalmology outpatient clinics.
Age-related PVD increases after age 40 and is frequently observed in the elderly. In myopic eyes, the incidence is even higher, and in highly myopic eyes, partial PVD may occur earlier than in emmetropic eyes and may progress to complete PVD 1,6).
In myopic eyes, PVD tends to occur earlier, and it may develop in the fellow eye within a certain period 1,6). Some PVDs are found incidentally without symptoms 6).
The annual incidence of rhegmatogenous retinal detachment (RRD) is 10 to 18 per 100,000 people 6), and vitreous traction due to PVD is the most common mechanism.
When PVD is complete, a ring-shaped opacity of collagen (Weiss ring, prepapillary glial ring) formed at the time of vitreous detachment from the optic disc is perceived as floaters.
QIs posterior vitreous detachment a disease?
A
Basically, it is a physiological change associated with aging and is not a disease itself. However, because serious complications such as retinal tears and retinal detachment can occur with the onset of PVD, appropriate ophthalmic examination and follow-up at the right time are essential.
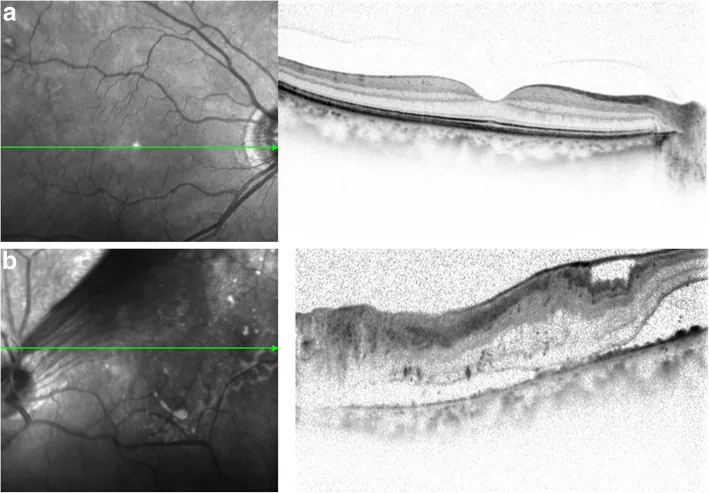
Miyamoto T, et al. A case of tractional retinal detachment associated with congenital retinal vascular hypoplasia in the superotemporal quadrant treated by vitreous surgery. BMC Ophthalmol. 2020. Figure 2. PMCID: PMC7542339. License: CC BY.
The main subjective symptoms that occur at the onset of PVD are shown below. Floaters and photopsia are typical complaints of PVD, and the majority originate from PVD 17).
Floaters: Symptoms of seeing something like mosquitoes, soot, or a ring moving with eye movements against a bright background such as a white wall or window. They are caused by collagen aggregation or Weiss ring formed when the posterior vitreous cortex separates from the ILM1). They are strongly perceived immediately after PVD onset, but as vitreous liquefaction progresses and complete PVD with collapse occurs, the prepapillary glial ring moves away from the retina, and subjective symptoms decrease. Differentiation from the blue field entoptic phenomenon (seeing small bright dots moving randomly in the visual field when looking at a bright blue sky) is necessary. Floaters can also cause a decrease in contrast sensitivity12).
Photopsia: Flashes of light perceived in the peripheral visual field in dark places or during eye movements. Light stimulation occurs in the retina due to vitreous traction on the ILM1). When floaters associated with PVD are accompanied by photopsia, it is judged that strong traction is acting on the retina, and a detailed fundus examination of every corner of the fundus is necessary.
Negative dysphotopsia: A symptom perceived as black flashes rather than white light. It is thought to occur because traction on the optic disc and ILM by the vitreous impairs axonal transport 4). It may appear before the classic photopsia of incomplete PVD 4).
The greater the number of floaters, the higher the risk of complications. When there are 10 or more floaters, the risk of retinal tear is highest1)17). Floaters usually decrease subjectively within about 3 months1). The impact of floaters on quality of life has been reported to be comparable to the utility value before cataract surgery13), so it is important not to underestimate patients’ complaints.
Floaters
Appearance: Worm-like, thread-like, or dot-like floating objects move within the visual field.
Cause: Aggregation of vitreous collagen, formation of Weiss ring (prepapillary glial ring).
Course: Often subjectively improves within about 3 months.
Photopsia
Appearance: White flashes in the peripheral visual field. Often occur in dark environments or with eye movement.
Cause: The vitreous pulls on the internal limiting membrane (ILM), stimulating the retina.
Importance: New photopsia is a sign of increased traction and risk of tear.
Negative Photopsia
Appearance: Black flashes (different from photopsia).
Cause: Vitreous traction at the optic disc → disruption of axonal transport.
The following fundus and vitreous findings are observed.
Weiss ring (prepapillary glial ring): A ring-shaped opacity of collagen floating in front of the optic disc. It indicates completion of PVD. Often not a complete ring; sometimes PVD occurs leaving the glial ring on the disc.
Shafer’s sign (tobacco dust): Tobacco dust-like pigment floating in the anterior vitreous is an important finding suggesting a retinal tear. It originates from retinal pigment epithelial cells; about 80% of cases with tobacco dust or hemorrhage later develop a retinal tear6).
Retinal tear: Occurs in 5.4–8% of PVD cases 6). Horseshoe tears are most common and frequently occur at lattice degeneration in the periphery.
Floaters and photopsia associated with PVD require attention; in PVD accompanied by tobacco dust or hemorrhage in the vitreous gel, a retinal tear should be suspected and examination should proceed accordingly.
Changes in hyalocytes (resident macrophage-like cells at the posterior vitreous cortex interface) are also observed. In en face OCT case reports, hyperreflective dots thought to be hyalocytes increase and show morphological changes in the posterior vitreous cortex of PVD eyes 2). In abnormal PVD, cellular reactions at the vitreoretinal interface may contribute to traction membrane formation.
QWhat should be done if vitreous hemorrhage occurs?
A
Vitreous hemorrhage is likely a sign of a retinal tear. Since the risk of a tear reaches 50–70% in cases with vitreous hemorrhage, promptly see an ophthalmologist for examination with indirect ophthalmoscopy or B-scan ultrasound. Once the hemorrhage clears, the fundus can be examined; until then, it is advisable to maintain rest.
In addition, OCT-based stage classification shows a stepwise progression from Stage 1 (paramacular PVD) to Stage 4 (complete PVD). The progression from partial PVD (Stages 1–3) to complete PVD peaks in the 50s to 60s. The AAO PPP 2024 also adopts a nearly identical four-stage classification: Stage 1 = paramacular separation with foveal adhesion remaining, Stage 2 = complete macular separation, Stage 3 = extensive separation with optic disc adhesion remaining, and Stage 4 = complete PVD 6). These stages do not necessarily progress linearly 6).
Shallow PVD is broadly divided into two types: those without thickening and contraction of the posterior vitreous cortex and those with it. Shallow PVD with thickening and contraction is seen in vitreomacular traction syndrome (VMT) and diabetic retinopathy, and often coexists with ERM. Those without thickening and contraction are classified as either an early stage of age-related PVD or perifoveal shallow PVD associated with macular hole.
The state of PVD (complete/partial/no PVD) greatly influences the prognosis of related diseases.
Diabetic retinopathy: If complete PVD is present, it does not progress to proliferative retinopathy. In no PVD or partial PVD, retinal neovascularization may occur and progress to tractional retinal detachment.
Epiretinal membrane (ERM): 80–95% of ERM cases are thought to occur after PVD 7). Partial PVD without shrinkage (M) type worsens the prognosis of ERM and DME.
The development of PVD involves a dual mechanism of vitreous “liquefaction” and “weakening of adhesion between the posterior vitreous cortex and the ILM” 1).
Liquefaction (syneresis): The vitreous is a gel composed of type II collagen fibers and hyaluronic acid (HA), with water accounting for 98–99% 1). Hyaluronic acid retains large amounts of water, increasing viscosity and maintaining the gel structure of the vitreous. With aging, collagen fibers aggregate and rearrange; by age 50, 25% of the vitreous is liquefied, and by age 80, 62% 1). Expansion of liquefied pockets makes the posterior vitreous cortex detach more easily from the ILM.
Weakening of adhesion: Degeneration of adhesion molecules (such as fibronectin) between the posterior vitreous cortex and the ILM reduces adhesive strength 1). PVD occurs when both liquefaction and adhesion weakening are present.
The posterior wall of the posterior vitreous cortex pocket (Kishi pocket) gradually detaches from the perifoveal area with aging (Stage 1), then becomes parafoveal PVD (Stage 2). Subsequently, the pocket detaches from the fovea (Stage 3), and finally detaches from the optic disc, leading to complete PVD (Stage 4).
Aging: The greatest risk factor. Prevalence increases sharply from 24% at ages 50–59 to 87% at ages 80–90 1).
High myopia: Vitreous degeneration accelerates with axial elongation, and early changes may occur in the 20s. Onset is about 10 years earlier than in emmetropic eyes 1). Even low myopia (1–3 D) increases the risk of rhegmatogenous retinal detachment (RRD) by 4 times, and over −3 D by 10 times 15). More than half of nontraumatic RRD occurs in myopic eyes 15).
After cataract surgery: The incidence of RRD within 1 year after cataract surgery is 0.21% (approximately 1 in 500) 20). 20–40% of all RRDs occur after cataract surgery 6). Nd:YAG laser posterior capsulotomy increases the risk of RRD by 4 times (especially in myopic eyes) 6).
History of RRD in the fellow eye: The risk of RRD in the fellow eye after non-traumatic RRD is approximately 10% 6).
The diagnosis of PVD involves a combination of several examinations. In particular, a detailed fundus examination to check for the presence of retinal tears is most important.
This is the first step in diagnosing whether floaters are physiological or pathological. The vitreous is observed using a slit-lamp microscope and a non-contact biconvex lens. Set the slit beam width narrow and the illumination intensity to maximum, and observe dynamically while paying attention to the movement of the vitreous.
The presence of a prepapillary glial ring (Weiss ring) is used as an indicator to confirm the presence of PVD, and the type of PVD (complete/partial) is classified based on the continuity of the posterior vitreous cortex with the retina.
If PVD is present and no obvious vitreous opacities other than the prepapillary glial ring are observed, it can be diagnosed as physiological floaters.
If tobacco dust, hemorrhage, or flare is observed, the entire fundus should be thoroughly examined.
The prepapillary glial ring is often not a complete ring, and sometimes PVD occurs leaving the glial ring on the optic disc.
Indirect ophthalmoscopy with scleral depression: Standard examination for direct observation of the peripheral fundus. Confirms the presence of retinal tears, lattice degeneration, and vitreous hemorrhage. AAO PPP recommends peripheral examination with scleral depression in PVD cases 6).
Optical coherence tomography (OCT): Noninvasively visualizes the positional relationship between the posterior vitreous cortex and the ILM. The stage of PVD can be assessed using the Kakehashi classification (Stages 0–4) 1). The clinical utility of PVD staging using circumpapillary OCT and macular volume OCT has also been reported 6).
Wide-field fundus photography: Useful for improving the detection rate of peripheral retinal tears 6).
En face OCT: Enables en face evaluation of hyalocyte distribution at the posterior vitreous cortex interface. It has been reported that hyperreflective spots, considered to be hyalocytes, can be evaluated by en face OCT in PVD eyes 2).
In patients presenting with floaters and photopsia, the most important step is to differentiate between physiological changes and pathological conditions.
Minor fibrous vitreous opacities or floaters associated with age-related PVD are called physiological floaters and do not require treatment. In contrast, floaters associated with retinal tears, retinal detachment, vitreous hemorrhage, or uveitis are pathological floaters and require active treatment.
If tobacco dust, hemorrhage, or flare is observed, it should be considered pathological, and a thorough fundus examination should be performed. In cases of PVD combined with photopsia, consider the possibility of strong traction on the retina and perform a detailed fundus examination. In PVD accompanied by tobacco dust or hemorrhage within the vitreous gel, proceed with examination assuming that “there is a retinal tear somewhere.”
Note that the blue field entoptic phenomenon, in which small bright dots move randomly within the visual field when looking at a bright blue light such as the sky, is different from floaters. It is caused by leukocytes flowing through retinal capillaries and does not require treatment.
Floaters associated with age-related PVD generally do not require active treatment; observation is the standard approach1)18). Physiological floaters do not require treatment. In many cases, floaters subjectively improve within 3 months as patients adapt.
Pathological floaters (caused by retinal tear, retinal detachment, vitreous hemorrhage, uveitis, etc.) require treatment of the underlying condition. No preventive measures for PVD have been established. There is no effective way to prevent vitreous liquefaction, PVD, or RRD6).
When a tear is confirmed, prompt closure is necessary. Retinal vitreous diseases associated with PVD are indications for surgical treatments such as laser photocoagulation, buckling surgery, and vitrectomy.
Laser photocoagulation: Create 2–3 rows of burns around the horseshoe tear to seal it. It is considered superior to cryopexy1). If the tear cannot be surrounded by laser or cryopexy, extend treatment to the ora serrata6). The most common cause of treatment failure is inadequate treatment, especially insufficient treatment of the anterior edge 6). At least half of untreated symptomatic horseshoe tears progress to RRD, but treatment can reduce the RRD risk to less than 5% 6).
Retinal cryopexy: Selected for cases where laser is difficult (e.g., peripheral tears).
Scleral buckling surgery: Surgical treatment for retinal detachment associated with PVD. Cochrane SR comparing PPV vs SB showed no significant difference in anatomical and visual outcomes (low to very low evidence) 6). Over 95% of uncomplicated RRD can be repaired (may require multiple surgeries) 6).
Vitrectomy: Surgical treatment for vitreoretinal diseases associated with PVD. It is also established as a standard surgical treatment for symptomatic floaters1).
Vitreous surgery (PPV): Selected when symptoms significantly impair QOL. It can remove Weiss rings and vitreous opacities 1). A prospective study by Sebag et al. (2014) confirmed its safety and efficacy 11). Nguyen et al. (2022) reported that PPV improves contrast sensitivity in multifocal pseudophakic eyes with floaters19). However, attention should be paid to complications such as infection, retinal detachment, and cataract progression.
YAG laser vitreolysis: In a RCT by Shah et al. (2017) (JAMA Ophthalmol), the YAG vitreolysis group had significantly higher symptom improvement rates compared to the sham group 10). However, for the overall treatment of floaters, it is stated that “there is no consensus on management and insufficient evidence” (AAO PPP 2024) 6), and the Cochrane SR (Kokavec et al. 2017) also concluded that comparative evidence is insufficient 14).
QOL impact: Wagle et al. (2011) reported that the utility value of floaters is comparable to that before cataract surgery 13). Garcia et al. (2016) reported decreased contrast sensitivity after PVD 12).
QCan floaters be cured with surgery?
A
When symptoms significantly impair quality of life, vitrectomy (PPV) or YAG laser vitreolysis are options. PPV can remove Weiss rings and vitreous opacities, and its safety and efficacy have been confirmed in prospective studies 11). Regarding YAG vitreolysis, an RCT (Shah 2017) showed significant improvement compared to sham 10), but both treatments are still being established as standard therapy, and indications should be carefully considered. Reports indicate that the impact of floaters on QOL is comparable to that before cataract surgery 13), so it is important not to underestimate patients’ complaints.
The vitreous is a gel-like transparent tissue that occupies about 80% of the eye’s volume, composed of 98-99% water 1). The remaining 1-2% consists mainly of hyaluronic acid (HA) and type II collagen fibers, which form a network structure maintaining the gel state. Hyaluronic acid retains large amounts of water, increasing viscosity and maintaining the vitreous gel structure. The posterior vitreous cortex adheres to the ILM, with an adhesion layer of fibronectin and other proteins between them.
The retina and vitreous are particularly strongly adherent at the following sites:
Vitreous base: The strongest adhesion site. Vitreous fibers run perpendicularly into the basement membrane of the ciliary body.
Wieger ligament: Adhesion between the posterior lens capsule and the anterior vitreous.
Normal PVD occurs through a process where “liquefaction precedes and adhesion weakens evenly.” In contrast, in anomalous PVD (vitreoretinal traction), even though liquefaction progresses, adhesion weakening is uneven, causing the vitreous to continue exerting strong local traction on the ILM1).
Vitreoschisis: A condition where the posterior vitreous cortex splits into inner and outer layers, with the outer layer remaining on the ILM. It contributes to vitreoretinal interface diseases (macular hole, epiretinal membrane, VMT) 2).
Role of hyalocytes: Resident macrophage-like cells at the posterior vitreous cortex interface. They may become activated with anomalous PVD and participate in the formation of tractional membranes (epiretinal membranes) 2).
Alsahaf et al. (2025) reported three cases of negative dysphotopsia4). It was hypothesized that vitreous traction on the optic disc pulls on Elschnig’s membrane and the ILM, impairing axonal transport in ganglion cells and leading to negative dysphotopsia (ND). In Case 1, after 6 months of ND, a complete PVD and retinal tear were found, and laser treatment was performed. In Case 2, after 5 months of ND, the condition progressed to rhegmatogenous retinal detachment, requiring vitrectomy.
Physiological PVD and physiological floaters do not require treatment. Symptoms are strongly perceived immediately after PVD onset, but after complete PVD, the Weiss ring moves away from the retina, and subjective symptoms decrease. Floaters usually diminish subjectively within about 3 months 1). Long-term prospective observation also shows that early management at the time PVD is recognized serves as the first line of defense against RRD 18).
Acute PVD without initial tear: approximately 2% develop a delayed tear within a few weeks 6)
Symptomatic PVD with tear at initial visit: 5–14% develop additional tears during long-term follow-up 6)
Approximately 80% of cases with vitreous pigment cells or hemorrhage subsequently developed tears 6)
Coffee et al. (2007) meta-analysis clarified the incidence and clinical features of delayed tears after symptomatic PVD 8)
Seider et al. (2022) prospectively examined complications of acute PVD 9)
Jindachomthong et al. (2023) reported the incidence and risk factors of delayed tears after acute symptomatic PVD 16)
Vangipuram et al. (2023) analyzed the timing of delayed retinal lesions in patients presenting with acute PVD using the IRIS® Registry 21)
QIf diagnosed with PVD, are regular check-ups necessary?
A
Even without an initial tear, about 2% develop a delayed tear within a few weeks, so a follow-up visit at 4–6 weeks is recommended 6). Especially if vitreous hemorrhage or pigment cells (tobacco dust) are present, follow-up every 1–2 weeks is necessary. Thereafter, it is generally recommended to visit as needed when symptoms change. Please seek prompt evaluation if new floaters increase, photopsia intensifies, visual field defects appear, or a curtain-like shadow is perceived.
Vitreous cortex components and activated hyalocytes remaining on the ILM after completion of PVD serve as a basis for epiretinal membrane (ERM) formation. It has been reported that 80–95% of ERM occur after PVD7), and OCT evaluation of the macula during PVD follow-up contributes to early detection of the disease.
Quantitative evaluation of hyalocytes using en face OCT may help predict the risk of vitreoretinal interface diseases (epiretinal membrane, VMT, macular hole). It has been reported that cells considered to be hyalocytes can be visualized and quantified by en face OCT in eyes with PVD 2), and cellular reactions at the vitreoretinal interface are attracting attention as a new research target.
Relationship between spontaneous separation of epiretinal membrane and PVD
Matsui et al. (2025) reported a 53-year-old woman with spontaneous separation of Stage 3 epiretinal membrane associated with an eye without PVD 5). The spontaneous separation rate of epiretinal membrane is usually 1-3%, but in eyes without PVD it is as high as 13.4%, far exceeding the 0.47-1.5% in eyes with existing PVD. OCT findings showed a decrease in epiretinal membrane thickness from 408 μm to 267 μm. It was suggested that vitreoschisis occurs at the adhesion site between the epiretinal membrane and the ILM in eyes without PVD, possibly involved in the mechanism of spontaneous separation.
Negative photopsia (dark flashes) is not distinguished from classic photopsia, and diagnosis may be delayed 4). In a case report by Alsahaf et al. (2025), a patient experienced negative photopsia before PVD progression, which later progressed to a tear and rhegmatogenous retinal detachment4). The clinical importance of recognizing negative photopsia as a specific complaint has been pointed out.
PVD and spontaneous closure of myopic macular hole
Chen et al. (2023) reported a case of spontaneous closure of a myopic macular hole without PVD 3). The spontaneous closure rate of myopic macular holes is reported to be 6.2% (3.5% in some reports), and elucidating the mechanism by which spontaneous closure occurs despite persistent vitreous traction in cases without PVD is a future challenge.
Attempts are underway to pharmacologically cleave the adhesion between the vitreous and ILM by injecting enzyme preparations such as ocriplasmin into the vitreous cavity 1). It has been approved in some countries for vitreomacular traction syndrome (VMT), but its position as a standard treatment has not been established.
An RCT by Shah et al. (2017) (JAMA Ophthalmol) showed that the YAG vitreolysis group had a significantly higher symptom improvement rate than the sham group 10). On the other hand, a Cochrane SR (Kokavec et al. 2017) concluded that the comparative evidence for YAG vitreolysis vs PPV is insufficient 14), and consensus formation on floaters treatment remains a future challenge.
Garcia et al. (2016) reported that high-frequency contrast sensitivity significantly decreases after PVD 12). Nguyen et al. (2022) showed that contrast sensitivity improves after PPV in patients with floaters in multifocal pseudophakic eyes 19), and quantitative assessment of the functional impact of floaters is gaining attention.
Johnson MW. Posterior vitreous detachment: evolution and complications of its early stages. Am J Ophthalmol. 2010;149(3):371-382.e1. doi:10.1016/j.ajo.2009.11.022.
Ahsanuddin S, Rahimy E, Chai R, et al. 3-D OCT imaging of hyalocytes in partial posterior vitreous detachment and vaso-occlusive retinal disease. Am J Ophthalmol Case Rep. 2023;30:101836. doi:10.1016/j.ajoc.2023.101836. PMCID: PMC10139967.
Fang-Ting Chen. SPONTANEOUS CLOSURE OF MYOPIC MACULAR HOLE TWICE WITHOUT POSTERIOR VITREOUS DETACHMENT. RETINAL Cases & Brief Reports. 2022;17(5):554-556. doi:10.1097/icb.0000000000001235.
Alsahaf M, Brookes M, Shanmuganathan V, Williamson TJ. Black Flashes (Dysphotopsia) As A Symptom of Vitreo-Papillary Traction in Evolving Posterior Vitreous Detachment - An Optical Coherence Tomography Case Series. Am J Ophthalmol Case Rep. 2025;39:102362. doi:10.1016/j.ajoc.2025.102362.
Matsui C, Nishida S, Takase H. Spontaneous peeling of epiretinal membrane without posterior vitreous detachment. Cureus. 2025;17(10):e95850.
American Academy of Ophthalmology. Posterior Vitreous Detachment, Retinal Breaks, and Lattice Degeneration Preferred Practice Pattern. AAO; 2024.
American Academy of Ophthalmology. Idiopathic Epiretinal Membrane and Vitreomacular Traction Preferred Practice Pattern. AAO; 2024.
Coffee RE, Westfall AC, Davis GH, Mieler WF, Holz ER. Symptomatic posterior vitreous detachment and the incidence of delayed retinal breaks: case series and meta-analysis. American journal of ophthalmology. 2007;144(3):409-413. doi:10.1016/j.ajo.2007.05.002. PMID:17583667.
Seider MI, Nomides REK, Hahn P, et al. Complications of acute posterior vitreous detachment. Ophthalmology. 2022;129:67-72.
Shah CP, Heier JS. YAG Laser Vitreolysis vs Sham YAG Vitreolysis for Symptomatic Vitreous Floaters: A Randomized Clinical Trial. JAMA ophthalmology. 2017;135(9):918-923. doi:10.1001/jamaophthalmol.2017.2388. PMID:28727887; PMCID:PMC5710539.
Sebag J, Yee KM, Wa CA, Huang LC, Sadun AA.. Vitrectomy for floaters: prospective efficacy analyses and retrospective safety profile. Retina. 2014;34(6):1062-1068. doi:10.1097/iae.0000000000000065. PMID:24296397.
Garcia GA, Khoshnevis M, Yee KMP, Nguyen-Cuu J, Nguyen JH, Sebag J. Degradation of Contrast Sensitivity Function Following Posterior Vitreous Detachment. American journal of ophthalmology. 2016;172:7-12. doi:10.1016/j.ajo.2016.09.005. PMID:27633841.
Wagle AM, Lim WY, Yap TP, Neelam K, Au Eong KG. Utility values associated with vitreous floaters. American journal of ophthalmology. 2011;152(1):60-65.e1. doi:10.1016/j.ajo.2011.01.026. PMID:21570045.
Kokavec J, Wu Z, Sherwin JC, Ang AJ, Ang GS. Nd:YAG laser vitreolysis versus pars plana vitrectomy for vitreous floaters. The Cochrane database of systematic reviews. 2017;6(6):CD011676. doi:10.1002/14651858.CD011676.pub2. PMID:28570745; PMCID:PMC6481890.
Risk factors for idiopathic rhegmatogenous retinal detachment. The Eye Disease Case-Control Study Group. Am J Epidemiol. 1993;137(7):749-757. PMID:8484366.
Jindachomthong KK, Cabral H, Subramanian ML, Ness S, Siegel NH, Chhablani J, et al. Incidence and Risk Factors for Delayed Retinal Tears after an Acute, Symptomatic Posterior Vitreous Detachment. Ophthalmology. Retina. 2023;7(4):318-324. doi:10.1016/j.oret.2022.10.012. PMID:36307014.
Boldrey EE. Risk of retinal tears in patients with vitreous floaters. American journal of ophthalmology. 1983;96(6):783-7. doi:10.1016/s0002-9394(14)71924-5. PMID:6660267.
Byer NE.. Natural history of posterior vitreous detachment with early management as the premier line of defense against retinal detachment. Ophthalmology. 1994;101(9):1503-13; discussion 1513-4. doi:10.1016/s0161-6420(94)31141-9. PMID:8090453.
Nguyen JH, Yee KMP, Nguyen-Cuu J, Mamou J, Sebag J. Vitrectomy Improves Contrast Sensitivity in Multifocal Pseudophakia With Vision Degrading Myodesopsia. American journal of ophthalmology. 2022;244:196-204. doi:10.1016/j.ajo.2022.05.003. PMID:35562070.
Morano MJ, Khan MA, Zhang Q, Halfpenny CP, Wisner DM, Sharpe J, Li A, Tomaiuolo M, et al. Incidence and Risk Factors for Retinal Detachment and Retinal Tear after Cataract Surgery: IRIS® Registry (Intelligent Research in Sight) Analysis. Ophthalmology science. 2023;3(4):100314. doi:10.1016/j.xops.2023.100314. PMID:37274012; PMCID:PMC10239011.
Vangipuram G, Li C, Li S, Liu L, Harrison LD, Lum F, Shah GK. Timing of Delayed Retinal Pathology in Patients Presenting with Acute Posterior Vitreous Detachment in the IRIS® Registry (Intelligent Research in Sight). Ophthalmology. Retina. 2023;7(8):713-720. doi:10.1016/j.oret.2023.04.004. PMID:37080486.
Copy the article text and paste it into your preferred AI assistant.
Article copied to clipboard
Open an AI assistant below and paste the copied text into the chat box.