A macular hole (MH) is a full-thickness retinal defect in the macula. The hole is not a loss of retinal tissue but results from traction by the posterior vitreous cortex, creating a small tear that enlarges into a hole. Spontaneous closure is rare, and over time the hole enlarges with degeneration of retinal pigment epithelial cells.
In 1988, Gass first described the four-stage progression of idiopathic macular holes. In 1991, Kelly and Wendel reported the effectiveness of vitrectomy, and in 1995, Brooks reported improved closure rates with concurrent internal limiting membrane peeling. Currently, vitrectomy with ILM peeling and gas tamponade is the standard surgical procedure.
Lamellar macular hole (LMH) is a condition that does not involve a full-thickness defect but rather a partial defect in the inner retinal layers, while the outer retinal layers are preserved. The prevalence is 1.1–3.6%, and it commonly occurs in individuals aged 50–70 years 12). It is important as a related lesion to be differentiated.
A pseudomacular hole is a condition in which the central fovea appears depressed relative to the surrounding epiretinal membrane, and it differs from idiopathic macular hole in that it is not a full-thickness hole.
The incidence of idiopathic macular hole is reported to be 3.14–7.8 per 100,000 population per year 2). In a US population-based study, the incidence was 7.8 per 100,000 per year (8.7 eyes), with a female-to-male ratio of 3.3:1 3). The peak age of onset is in the 60s to 70s, especially the 60s. 72% of patients are female, more than 50% develop the condition between ages 65 and 74, and only 3% are under 55 3).
It is usually unilateral, but the frequency of involvement in the fellow eye is 10–20%. The 5-year risk of fellow eye involvement is 10–15%, reaching up to 28% in the absence of complete posterior vitreous detachment (PVD) 2). Asians have been reported to have a 177% increased risk of iFTMH compared to Caucasians 2). Traumatic cases are more common in young males, in contrast to idiopathic cases.
Macular hole retinal detachment is more common in women with high myopia, accounting for about 5% of retinal detachment cases in Japan, which is higher than the 0.5–2.0% in Western countries.
QDoes macular hole occur in both eyes?
A
The risk of fellow eye involvement after unilateral onset is moderate. In patients without posterior vitreous detachment in the fellow eye, the risk reaches up to 28% over 5 years 2). If the fellow eye has complete posterior vitreous detachment, the risk is low. The timing of onset is not necessarily simultaneous, but about 10–20% of cases develop in both eyes.
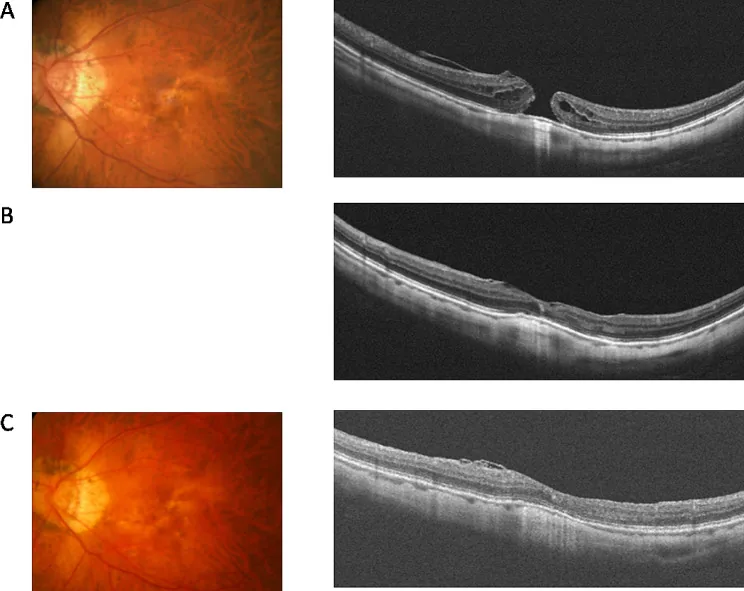
Wu TT, et al. Inverted flap technique versus internal limiting membrane insertion for macular hole in eyes with extremely high myopia. BMC Ophthalmol. 2024. Figure 1. PMCID: PMC11251341. License: CC BY.
Preoperative OCT clearly shows a full-thickness hole in the macula. Postoperative OCT demonstrates hole closure, making it easy to understand the typical imaging findings of a macular hole.
Untreated full-thickness macular holes often have a poor prognosis. About 40–50% of Stage 1 holes progress to full-thickness holes, and about 50% resolve spontaneously with posterior vitreous detachment3). About 75% of Stage 2 holes progress to Stage 3 or 4 3). In untreated full-thickness macular holes, only 5% maintain visual acuity of 20/50 or better, 55% have 20/100 or worse, and 40% have 20/200 or worse 3). The spontaneous closure rate with observation alone is 2.5–27% (depending on size and duration), and no spontaneous closure occurs in large holes (>400 μm) 2).
The staging system described by Gass in 1995 is still widely used as the standard. Advances in OCT have provided a more detailed understanding of the pathology at each stage.
Stage 1 (Impending/ Occult)
Stage 1A (Impending hole): The fovea is deformed due to posterior vitreous detachment. There is loss of the foveal depression and a yellow spot (100–200 μm) 3). A foveal cystoid space or foveal retinal detachment forms.
Stage 1B (Occult hole): A yellow ring (200–350 μm) is present 3). There is separation of the photoreceptor layer but not yet a full-thickness hole (occult hole).
Natural course: About 50% of Stage 1 holes improve spontaneously.
Stages 2–4 (Full-Thickness Hole)
Stage 2: Full-thickness hole <400 μm. It may be eccentric with a flap 3). The posterior vitreous cortex is connected to the fovea by a flap.
Stage 3: Full-thickness hole ≥400 μm. It is associated with a free pseudo-operculum. Posterior vitreous detachment is incomplete.
Stage 4: Posterior vitreous detachment is complete. A glial ring is observed on ophthalmoscopy. A Weiss ring is present.
In 2013, the International Vitreomacular Traction Study Group (IVTS) established a classification based on OCT findings. Full-thickness macular holes are classified based on the minimum diameter 2).
Category
Minimum Diameter
Small (S)
< 250 μm
Medium (M)
250–400 μm
Large (L)
> 400 μm
Generally, Stage 2 or later and medium or larger holes are considered active surgical indications. The CLOSE Study Group proposed further subclassification of large holes into L (>400–≤550 μm), XL (>550–≤800 μm), XXL (>800–≤1000 μm), and Giant (>1000 μm). Reports indicate that closure rates drop below 90% for holes exceeding 500 μm 2).
Lamellar holes are broadly classified into two types according to Govetto et al.: “degenerative type” and “tractional type” 13). Hubschman et al. further redefined the degenerative type as “LMH” and the tractional type as “ERM foveoschisis (ERMF)” 12).
The degenerative type is characterized by nonlinear cavitation of the inner retina, loss of foveal tissue, and lamellar hole-associated epiretinal proliferation (LHEP). The tractional type is characterized by the presence of a contractile epiretinal membrane and retinal separation at the level of the Henle fiber layer 13). The degenerative type is more likely to involve disruption of the ellipsoid zone (EZ) and tends to have a poorer visual prognosis.
QDoes a Stage 1 macular hole require treatment?
A
Stage 1 is an impending hole that has not yet progressed to a full-thickness hole, and about 50% improve spontaneously 3). Observation is usually recommended. However, because there is a risk of progression, regular follow-up with OCT is important.
The main cause of idiopathic macular hole is vitreomacular traction during the early stages of age-related posterior vitreous detachment (PVD) 2).
In the human eye, there is a physiological liquefied pocket (pre-posterior vitreous cortex pocket: Kishi pocket) anterior to the macula. The cortex forming the posterior wall of the pocket pulls on the macula with aging and contributes to the development of macular holes.
The process of development is as follows:
With aging, the vitreous liquefies, and a liquefied pocket (pocket) forms anterior to the posterior vitreous cortex.
The posterior vitreous membrane detaches from the retina around the fovea (perifoveal PVD).
At the fovea, vitreous adhesion is physiologically strong, so adhesion is maintained.
Anteroposterior traction concentrates on the fovea.
Separation of the Müller cell cone and photoreceptors occurs, leading to the formation of intraretinal cysts 2).
If traction persists, the ILM and ELM rupture, resulting in a full-thickness hole 2).
The extent of outer retinal defect correlates with the range and intensity of vitreomacular traction; broader adhesion leads to more extensive photoreceptor loss 2). When glial repair attempts fail, glial cells migrate and contract on the ILM at the hole margin, enlarging the hole through tangential traction 2).
When blunt trauma is applied to the eye, anteroposterior compression and equatorial expansion occur simultaneously. This deformation concentrates tangential traction on the macula, tearing the foveal tissue and forming a hole. In young individuals, the vitreous is firmly attached to the retina (no PVD), so external force is easily transmitted directly to the macula via the vitreous 14). Approximately 85% of TMH cases show no posterior vitreous detachment.
High-power lasers, such as accidental exposure to laser pointers, can also be a cause.
OCT is the gold standard for diagnosis and management of macular holes 3). It allows detailed evaluation of the retinal structure at the macular hole. The following information can be obtained:
Confirmation of full-thickness hole and measurement of minimum linear diameter (MLD): Select the OCT slice with the widest cross-section and measure the minimum width at the middle of the hole. This has good reproducibility and is the standard in clinical practice and research 2).
Evaluation of subretinal fluid and cystoid changes
Status of the ellipsoid zone (EZ)
To exclude a pseudohole, OCT should confirm that there is no full-thickness retinal defect in the depressed area. It is important to perform a volume scan and examine continuously.
As basic examinations at the first visit, in addition to OCT, best-corrected visual acuity (BCVA), intraocular pressure (IOP), and peripheral retinal examination (screening for tears) should be performed 3).
Detailed fundus examination under mydriasis is fundamental. In full-thickness macular holes, a grayish macular rim (reflecting subretinal fluid accumulation), yellow deposits at the hole base, and RPE changes are observed.
Watzke-Allen test (slit beam sign): When a thin slit beam is directed at the macular hole, the patient perceives the slit beam as distorted inward at the fixation point. If the center of the slit beam appears narrowed or broken, it suggests a macular hole; if only distorted, it is likely a pseudohole. Positive in full-thickness holes, negative in pseudoholes.
The following diseases require differentiation. All are distinguished from macular hole by the absence of full-thickness retinal defect on OCT.
Pseudohole: A cylindrical depression of the fovea due to contraction of an epiretinal membrane. Visual acuity is relatively good, and the Watzke-Allen test is negative. If visual acuity is good and there are no subjective symptoms, surgery is generally not performed and the patient is observed.
Lamellar macular hole (LMH): Partial defect of the inner retinal layers. The outer retinal layers are preserved.
ERM foveoschisis (ERMF): Separation at the level of Henle fiber layer due to contractile ERM. A new concept that should be distinguished from pseudohole and LMH 12).
QHow to differentiate pseudohole from full-thickness macular hole?
A
OCT allows easy differentiation. In pseudohole, there is no full-thickness retinal defect, and foveal depression due to epiretinal membrane is observed. The Watzke-Allen test is negative in pseudohole and positive in full-thickness hole. It is important to confirm the absence of full-thickness retinal defect in the depressed area on OCT and to verify continuously with volume scan.
Treatment for macular hole is vitreous surgery. There is no medical therapy. In patients aged 50 years or older, cataract surgery is often performed simultaneously.
Standard procedure: vitrectomy + internal limiting membrane peeling + gas tamponade
Internal limiting membrane (ILM) peeling: The ILM is visualized with brilliant blue G (BBG) or triamcinolone and peeled with forceps. BBG is a mixture of 0.025% BBG and 4% polyethylene glycol, which has a high specific gravity and settles onto the ILM surface for staining simply by injecting from the vial 3). ICG (indocyanine green) is also used, but high concentration and prolonged exposure should be avoided 3).
Fluid-air exchange: The fluid in the vitreous cavity is replaced with air.
Gas tamponade: Air (lasting a few days), SF₆ (2–3 weeks), C₂F₆ (4–5 weeks), C₃F₈ (6–8 weeks), or silicone oil (requires removal) are used 3). In a UK survey (2018), the most commonly used gas was C₂F₆ (47%), followed by SF₆ (33%), C₃F₈ (19%), and air (1%) 2).
Postoperative positioning: The patient maintains a face-down position for about 3 days so that the gas contacts the hole.
A meta-analysis of 5,480 cases (Rahimy 2016) showed a closure rate difference of 98.82% in the ILM peeling group vs. 92.88% in the non-peeling group (P<0.0001), and the reopening rate was significantly reduced (25% → 0%) 3). A meta-analysis of 4 RCTs (317 cases, Stage 2–4) also showed a reduced need for additional surgery in the ILM peeling group, and a larger area of ILM peeling was associated with less metamorphopsia3). ILM peeling is cost-effective, and a cost-effectiveness analysis based on RCTs showed that ILM peeling was superior to non-peeling over 6 months 3).
The closure rate with the standard procedure is 91–98%3). In the RCOphth meta-analysis, the surgery group had a visual acuity advantage of 0.16 logMAR (95% CI −0.23 to −0.09) compared to the observation group, and the odds ratio for hole closure was 31.4 (95% CI 14.9–66.3), clearly demonstrating the effectiveness of surgery 2). In UK real-world data (1,483 eyes), the closure rate was 95.7%, VA improved from 0.78 to 0.42 logMAR (approximately 4 lines improvement), and 64.2% improved by 0.3 logMAR or more 2).
The median postoperative visual acuity is approximately 20/40 (0.5), with visual improvement sustained for up to 3 years and maintained for 5–10 years 3). Since BCVA worsens by 0.008 logMAR for each 1-month increase in symptom duration (≈1 ETDRS letter loss every 2 months), early surgical intervention is important 3) (12 RCTs, IPD meta-analysis of 940 eyes). When disease duration exceeds 2–3 years, the closure rate drops to 63% and visual prognosis becomes poor 3). Shorter disease duration and smaller hole size are associated with higher closure rates and better visual prognosis.
A Cochrane review of 8 RCTs including 709 eyes found no significant difference in hole closure rates between prone and non-prone groups. Even for large holes (≥400 μm), the closure rate was 94% in the prone group vs. 84% in the non-prone group; for small holes, it was 100% vs. 96%. A meta-analysis (251 cases, 5 RCTs) suggests that prone positioning is unnecessary for holes <400 μm but beneficial for holes ≥400 μm 3). A UK survey (2018) reported that 82% of surgeons still recommend positioning restrictions, with durations varying: 1 day (19%), 2–4 days (30%), 5–6 days (23%), and ≥1 week (9%) 2).
Large macular holes (>400 μm), long-standing cases, and secondary holes associated with high myopia, trauma, or inflammation are considered refractory.
Inverted ILM flap technique:
This technique is applied to large holes ≥1/3 disc diameter or primary non-closure cases. The ILM peeled to the edge of the hole is inverted and placed over or into the hole. In reoperations, a free ILM flap obtained from outside the macula can be placed into the hole to promote closure. A systematic review of 4 small RCTs suggests that this technique may provide better BCVA improvement than standard ILM peeling (low evidence) and superior closure rates (moderate evidence) 3).
ILM flap without gas tamponade (Szeto 2025):
This gasless technique uses a temporal ILM flap (in 92.9% of cases) and perfluorocarbon liquid (PFCL) to unfold and stabilize the flap 16).
Szeto et al. (2025) reported a gasless technique for large holes (including >30% with high myopia, MLD ≥500 μm) 16). The closure rate was comparable between the gasless group (94.1%) and conventional group (95.2%) (P=0.812). Early postoperative visual acuity was significantly better in the gasless group (at 1 week and 1 month). The rate of foveal gliosis was lower in the gasless group (4.9% vs. 20.0%, P=0.043). OCT evaluation was possible from the day after surgery, and there was no patient burden from positioning restrictions 16).
Surgical techniques using other biomaterials (Romano 2025)1):
Human amniotic membrane (hAM): used as a scaffold. Meta-analysis shows benefit for refractory MH. Closure rate 57–100%.
Autologous retinal full-thickness transplant (ART): transplants peripheral retina. Meta-analysis by Hanai 2024 shows closure rate 94%. Used for recurrent and large holes.
Mesenchymal stem cells (MSC): closure in 6 of 7 cases.
Nerve growth factor (NGF): MH closure rate 100%, EZ/ELM recovery also better in NGF group.
Song et al. (2024) reported surgical outcomes for 8 eyes with macular hole associated with retinitis pigmentosa6). Hole closure was achieved in all eyes that underwent ILM peeling; ILM free flap transplantation was used for large holes. Postoperative visual acuity improved in 1 eye and remained stable in 7 eyes.
In the natural course, visual acuity decreases to 0.1 or less in many cases. Surgery achieves hole closure in over 90% of cases and improves visual acuity. However, metamorphopsia often persists. If the hole does not close after initial surgery, reoperation with extended ILM peeling or autologous ILM transplantation is considered.
Because spontaneous closure is possible (10–67%), initial management after injury is a period of observation. Spontaneous closure is thought to occur when glial cells bridge the defect. Younger patients have a relatively higher spontaneous closure rate due to greater glial cell proliferative capacity.
If spontaneous closure does not occur, vitrectomy (PPV) with internal limiting membrane (ILM) peeling is the gold standard14). Closure rates of 82–96% have been reported14). Although the efficacy of ILM peeling is not fully established, the same surgical technique as for idiopathic holes is used. Postoperatively, gas tamponade (SF₆ or C₃F₈) is performed, and prone positioning is required. For large or refractory holes, ILM flap technique or amniotic membrane transplantation are options14).
In a meta-analysis by Zhou et al. (2021), comparing closure rates between PPV and spontaneous closure, the surgical group showed significantly higher closure rates 15). Prolonged waiting may reduce closure rates and, even if closure occurs, visual recovery may be insufficient.
Vitrectomy for traumatic macular holes due to blunt trauma has been reported to achieve closure rates of over 90%. Visual improvement depends on hole closure and the presence and location of other injuries besides the macular hole.
Treatment of Macular Hole Retinal Detachment (High Myopia)
In high myopia, a macular hole may progress to retinal detachment. The standard procedure is vitrectomy with internal limiting membrane peeling and gas (or silicone oil) tamponade. Even if posterior vitreous detachment appears to have occurred, vitreous cortex remains attached to the retina over a wide area. Residual vitreous cortex is removed under triamcinolone visualization, and the internal limiting membrane is peeled for 2–3 disc diameters using vital dye. The reattachment rate is about 70%, lower than that for typical rhegmatogenous retinal detachment (over 90%).
Observation:
Many LMHs remain stable over time, and asymptomatic idiopathic cases do not require treatment. Regular OCT follow-up is performed to monitor structural changes.
LHEP-sparing surgery:
Surgery is considered when there is symptomatic visual decline, progressive metamorphopsia, or worsening foveal profile. Recently, techniques that preserve or embed the LHEP without peeling have gained attention.
In a meta-analysis by Yu et al. (2025) of 8 studies, the postoperative BCVA improvement in the LHEP-sparing surgery group was significant at −0.25 logMAR (95% CI −0.30 to −0.21, P<0.00001)11). Compared with conventional peeling, the difference in BCVA improvement was −0.19 logMAR (P<0.0001), favoring the sparing group. The proportion of patients with postoperative EZ restoration was also significantly higher in the sparing group (OR 2.55; 95% CI 1.48 to 4.38)11). No postoperative FTMH formation was reported in the LHEP-sparing group11).
If visual acuity is good and there are no subjective symptoms, surgery is generally not performed and observation is often chosen. If subjective symptoms such as decreased vision or severe metamorphopsia are present, vitrectomy is considered, similar to the treatment of epiretinal membrane. In vitrectomy, the epiretinal membrane and internal limiting membrane are peeled.
Retinal tear: Occurs in 3–17% during or after surgery. Most are found inferiorly3).
Retinal detachment: Occurs in 1–5% postoperatively. Most are due to small inferior flap tears. Most can be repaired without reopening the hole3).
Cataract: Over 80% of phakic eyes develop cataract within a few years after surgery. Cataract surgery is needed at a median of 14 months, and 98% require surgery over a mean follow-up of 91 months3). After cataract surgery, 11% of closed holes reopen, and the risk of reopening is 7 times higher with CME occurrence3).
DONFL (dissociated optic nerve fiber layer): Defect-like findings along nerve fiber bundles may appear several months after ILM peeling. This finding does not suggest visual field defects.
Reopening: Up to 10% of successfully closed holes reopen, but ILM peeling reduces this risk3).
Visual field defect: Previously seen in 20%, but decreased with smaller gauge and low-pressure perfusion3).
Postoperative endophthalmitis: Less than 0.05%3). Rare but serious complication.
QHow soon does vision recover after surgery?
A
Preoperative visual acuity, hole size, and duration of symptoms affect visual prognosis. The median postoperative visual acuity is approximately 20/40 (0.5), with improvement sustained up to 3 years and maintained for 5–10 years 3). Metamorphopsia often persists. Longer duration of symptoms leads to worse prognosis; beyond 2–3 years, the closure rate drops to 63% 3). In traumatic cases, associated injuries besides the macular hole also affect visual prognosis.
The development of idiopathic macular holes is closely related to the early stages of posterior vitreous detachment (PVD) 2). In normal aging, PVD begins around the fovea and progresses in four stages. In Stage 1, the vitreous detaches perifoveally but remains attached at the fovea, and finally in Stage 4, detachment from the optic disc completes the process 2).
Macular holes develop as a pathological condition of PVD Stage 1. Abnormal vitreous attachment persists at the fovea, and dynamic traction from eye movements causes separation between the Müller cell cone and photoreceptors 2). On OCT, this process is observed as intraretinal cysts.
If anteroposterior traction persists, the ILM and ELM break, leading to retinal dehiscence and a full-thickness hole 2).
The exact mechanism by which ILM peeling and gas tamponade during vitrectomy close the hole is not fully understood. Early after ILM peeling, the macula shifts slightly nasally and toward the fovea along nerve fiber bundles. This retinal movement is thought to contribute to approximation of the hole edges.
Recent OCT studies consistently show the involvement of traction in LMH formation. In a study of 50 highly myopic eyes by Hsia et al. (2023), traction was identified in all LMH formation processes 9). Four traction-related formation processes were identified.
Type 1: Avulsion of foveal tissue due to vitreomacular traction. Corresponds to an abortive attempt at FTMH formation 9).
Type 2: Rupture of the inner wall of a parafoveal cyst associated with epiretinal membrane or retinoschisis. Most frequent (64%) 9).
Type 3: Tearing of the roof of a foveal cyst caused by epiretinal membrane or vitreous traction 9).
Type 4: Progressive thinning of the fovea due to sustained traction of the epiretinal membrane without cyst formation. All cases progressed to FTMH and had the worst prognosis 9).
Spontaneous closure of some LMHs has been reported. Catania et al. (2024) reported spontaneous closure in 11 of 187 degenerative cases (5.9%) and 10 of 200 mixed cases (5.0%) 10). The median time to closure was 4 years 10).
In the closure group, the frequency of hyperreflective inner border (HIB) at the cavity margin and linear hyperreflective outer plexiform layer (LHOP) was significantly higher than in the stable group 10). These findings may reflect coordinated activation of microglia and Müller cells 10).
Myopic: Outward traction due to posterior staphyloma and macular schisis are involved 1). Vitrectomy alone may be insufficient, and combined macular buckling is considered.
Traumatic: Ocular deformation and retinal stretching due to trauma, and strong vitreoretinal adhesion in young individuals are involved 14).
Drug-induced: Tamoxifen-induced macular holes are speculated to involve Müller cell neurodegeneration 4). Outer layer defects are characteristic, while the inner layer is often preserved.
Alport syndrome: Complete absence of the ILM due to type IV collagen mutation 7). The ILM is completely absent, making macular hole surgery difficult.
Pediatric non-traumatic: Traction due to epiretinal proliferation may be the cause. A 9-year-old girl achieved closure in 1 month with ILM peeling and C₃F₈ gas tamponade, with visual acuity improving to 20/40 at 1 year postoperatively 8).
7. Latest Research and Future Perspectives (Research-stage Reports)
Ocriplasmin is a 27 kDa serine protease that enzymatically cleaves the adhesion between the vitreous and retina1). The dose is a single intravitreal injection of 0.125 mcg/0.1 mL 2). Indications are limited to cases with “persistent VMT + iFTMH <400 μm + no ERM” 2).
In the MIVI-TRUST trials, vitreomacular adhesion release was achieved in 26.5% of the ocriplasmin group (vs. 10.1% placebo) at 28 days post-injection, and the hole closure rate was 40.6% in the ocriplasmin group (vs. 10.6% placebo). In the RCOphth IPD meta-analysis (1,067 cases), iFTMH closure rate was 36.8% (control 9.3%, OR 6.1), VA improvement was +5.97 letters (control +3.33 letters, difference +2.32 letters) 2).
Reported side effects include ERG changes (amplitude reduction 40%, 81.3% recovered over time), dyschromatopsia (4.5% vs. control 0.6%), and lens subluxation2). In real-world clinical practice, efficacy tends to be lower than in RCTs, and adoption rates are declining 2).
Intravitreal gas injection (pneumatic vitreolysis)
In the DRCR Retina Network Protocol AH trial, 0.3 mL of 100% C₃F₈ was injected intravitreally for small MH (median 79 μm). The closure rate was 29% (95% CI 16–45%), but retinal tears/detachment occurred in 12% (7/59 eyes, 95% CI 6–23%), leading to trial termination2). It is contraindicated in patients with peripheral retinal fragility 2).
LHEP-sparing surgery has been rapidly developing in recent years. A technique of embedding a double flap of peeled ILM and LHEP into the macular hole has also been reported 11). Future prospective randomized controlled trials are needed 11).
HIB and LHOP detected by image processing may serve as predictive markers for spontaneous closure of LMH 10). Future prospective studies are expected to validate these markers.
Retinal regeneration therapy using stem cells is at an experimental stage 1). It is expected to be applied for photoreceptor regeneration and functional recovery after macular hole closure.
Grieco G, Carla MM, Di Stefano G, Scampoli A, Governatori L, Tombolini B, et al. Updates on surgical and nonsurgical innovations for macular hole treatment. Surv Ophthalmol. 2025 Nov 12:S0039-6257(25)00215-2. doi:10.1016/j.survophthal.2025.11.008.
Kim SJ, Lim JI, Bailey ST, Kovach JL, Vemulakonda GA, Ying GS, et al; American Academy of Ophthalmology Preferred Practice Pattern Retina/Vitreous Committee. Idiopathic Macular Hole Preferred Practice Pattern. Ophthalmology. 2025 Feb 7:S0161-6420(24)00785-1. PMID:39918525. doi:10.1016/j.ophtha.2024.12.021.
Sohn A, Sanchez G, Mantopoulos D.. Partial thickness subfoveal hole in a patient treated with tamoxifen: a case report and review of the literature. J Med Case Rep. 2022;16(1):471. doi:10.1186/s13256-022-03681-4. PMID:36539911; PMCID:PMC9769049.
Bailey ST, Vemulakonda GA, Kim SJ, Kovach JL, Lim JI, Ying GS, et al. Idiopathic Epiretinal Membrane and Vitreomacular Traction Preferred Practice Pattern®. Ophthalmology. 2025;132(4):P197-P233. doi:10.1016/j.ophtha.2024.12.019. PMID:39918520.
Song Y, Zhang Y, Si Y, Wu S, Xiu M, Zhu J, Cui Y.. Pre- and postoperative OCT features and surgical outcomes of advanced retinitis pigmentosa with macular hole: case series and literature review. BMC Ophthalmol. 2024;24(1):370. doi:10.1186/s12886-024-03643-y. PMID:39187836; PMCID:PMC11346043.
Chaudhry SG, Liew G, Fung AT. Missing Internal Limiting Membrane during Macular Hole Repair in Alport Syndrome. Case reports in ophthalmology. 2021;12(2):320-323. doi:10.1159/000513420. PMID:34054478; PMCID:PMC8136316.
Said RB, Kraker JA, Trejo-Lopez J, Salomao DR, Scruggs BA. PEDIATRIC MACULAR HOLE ASSOCIATED WITH VITREORETINAL TRACTION ON EPIRETINAL LESIONS: A CASE REPORT AND LITERATURE REVIEW. Retinal cases & brief reports. 2025;19(6):730-735. doi:10.1097/ICB.0000000000001663. PMID:39733272; PMCID:PMC12570607.
Hsia Y, Lee CY, Ho TC, Yang CH, Yang CM. The development and evolution of lamellar macular hole in highly myopic eyes. Eye (London, England). 2023;37(6):1170-1177. doi:10.1038/s41433-022-02086-3. PMID:35562550; PMCID:PMC10102228.
Catania F, Romano MR, Crincoli E, et al. Phenomenology of spontaneous closure in degenerative and mixed type lamellar macular hole. Eye (Lond). 2024;38:315-320. doi:10.1038/s41433-023-02681-y. PMID:37524832; PMCID:PMC10810871.
Yu Y, Wang YY, Tian M, Yu XH.. SURGICAL OUTCOMES OF LAMELLAR MACULAR HOLE EYES WITH OR WITHOUT PRESERVATION OF LAMELLAR HOLE-ASSOCIATED EPIRETINAL PROLIFERATION TECHNIQUE: A Meta-analysis. Retina. 2025;45(11):1996-2002. doi:10.1097/iae.0000000000004607. PMID:40668983; PMCID:PMC12548810.
Andrea Govetto, Yann Dacquay, Matthew Farajzadeh, Eva Platner, Kyle Hirabayashi, Hamid Hosseini, Steven D. Schwartz, Jean-Pierre Hubschman. Lamellar Macular Hole: Two Distinct Clinical Entities?. American Journal of Ophthalmology. 2016;164:99-109. doi:10.1016/j.ajo.2016.02.008.
Liu W, Grzybowski A. Current management of traumatic macular holes. J Ophthalmol. 2017;2017:1748135. doi:10.1155/2017/1748135. PMID: 28239490. PMCID: PMC5292388.
Qi Zhou, Haoyue Feng, Hongbin Lv, Zhongmei Fu, Yuyu Xue, Hejiang Ye. Vitrectomy vs. Spontaneous Closure for Traumatic Macular Hole: A Systematic Review and Meta-Analysis. Front. Med. 2021;8. doi:10.3389/fmed.2021.735968.
Szeto SKH, Lam JTW, Yu AHY, Pang CMK, Lin TPH, Hui VWK, et al. Macular Hole Closure by Internal Limiting Membrane Flap without Gas Tamponade versus Conventional Surgery: A Comparative Study. Ophthalmol Retina. 2025;9(11):1034-1043. doi:10.1016/j.oret.2025.06.005. PMID:40518116.
Copy the article text and paste it into your preferred AI assistant.
Article copied to clipboard
Open an AI assistant below and paste the copied text into the chat box.