The amniotic membrane is a thin biological membrane that envelops the fetus and placenta inside the uterus of a pregnant woman. Together with the chorion and decidua, it forms the fetal membranes. The basement membrane of the amniotic membrane is the thickest in the body, has appropriate elasticity and extensibility, and exhibits excellent biocompatibility.
Amniotic membrane transplantation (AMT) is a surgical procedure in which this amniotic membrane is transplanted onto the ocular surface to reconstruct the cornea and conjunctiva. In ophthalmology, it was first reported by De Roth in 1940 for eyelid adhesions due to chemical burns. In 1995, Tseng et al. demonstrated the effectiveness of amniotic membrane transplantation for ocular surface reconstruction in rabbit eyes, leading to its widespread adoption both in Japan and abroad.
In Japan, after clinical research and advanced medical treatment systems, it was covered by insurance in 2014 (Heisei 26). Amniotic membrane transplantation is broadly classified into the following three methods.
Amniotic membrane graft method: Aims to supply the substrate.
Amniotic membrane stuff method: Aims to fill tissue defects.
QDoes the amniotic membrane not cause rejection?
A
The amniotic membrane has extremely low antigenicity and is an excellent biological support material that does not induce rejection. It can be used without HLA matching, offering advantages different from corneal transplantation.
The indications for amniotic membrane transplantation are diverse. In principle, it is indicated for ocular surface diseases for which other treatments are not sufficiently effective.
Recurrent pterygium: Particularly useful in recurrent cases with symblepharon. The extensive conjunctival defect is covered with an amniotic membrane graft. Often combined with intraoperative mitomycin C (MMC) application.
Chemical and thermal burns of the cornea and conjunctiva: Amniotic membrane covering promotes epithelialization in acute extensive corneal and conjunctival epithelial defects.
For severe dry keratoconjunctivitis, short-term placement (2–7 days) of cryopreserved amniotic membrane is emerging as a treatment option 1). Significant improvements in corneal staining scores, ocular discomfort, and severity have been reported.
3. Biological Properties and Mechanisms of Action of the Amniotic Membrane
The reason amniotic membrane is useful for ocular surface reconstruction is due to the following multifaceted biological actions.
Action as a substrate: The basement membrane promotes the extension, proliferation, and differentiation of corneal and conjunctival epithelium. Covering the exposed sclera and placing the conjunctival resection edge over the amniotic membrane periphery results in good epithelialization.
Anti-inflammatory action: Suppresses the production of inflammatory cytokines.
Anti-fibrotic action: Suppresses fibroblast proliferation and reduces postoperative scar formation.
Anti-angiogenic action: Suppresses the formation of new blood vessels.
Low antigenicity: Expression of HLA antigens is extremely low, so it does not induce rejection.
These characteristics make it highly effective in cases where recurrence of proliferative conjunctival diseases or postoperative scarring is a concern. Mitomycin C similarly suppresses fibroblasts, but amniotic membrane is superior in that it also acts as a substrate for the epithelium.
QHow are amniotic membrane and mitomycin C used differently?
A
Both have the effect of suppressing fibroblast proliferation. In pterygium surgery, for primary cases in young patients with thick, vascular tissue or for recurrent cases, intraoperative application of mitomycin C and amniotic membrane transplantation are actively combined. Amniotic membrane also has the advantage of functioning as a substrate for the epithelium, and the two act complementarily.
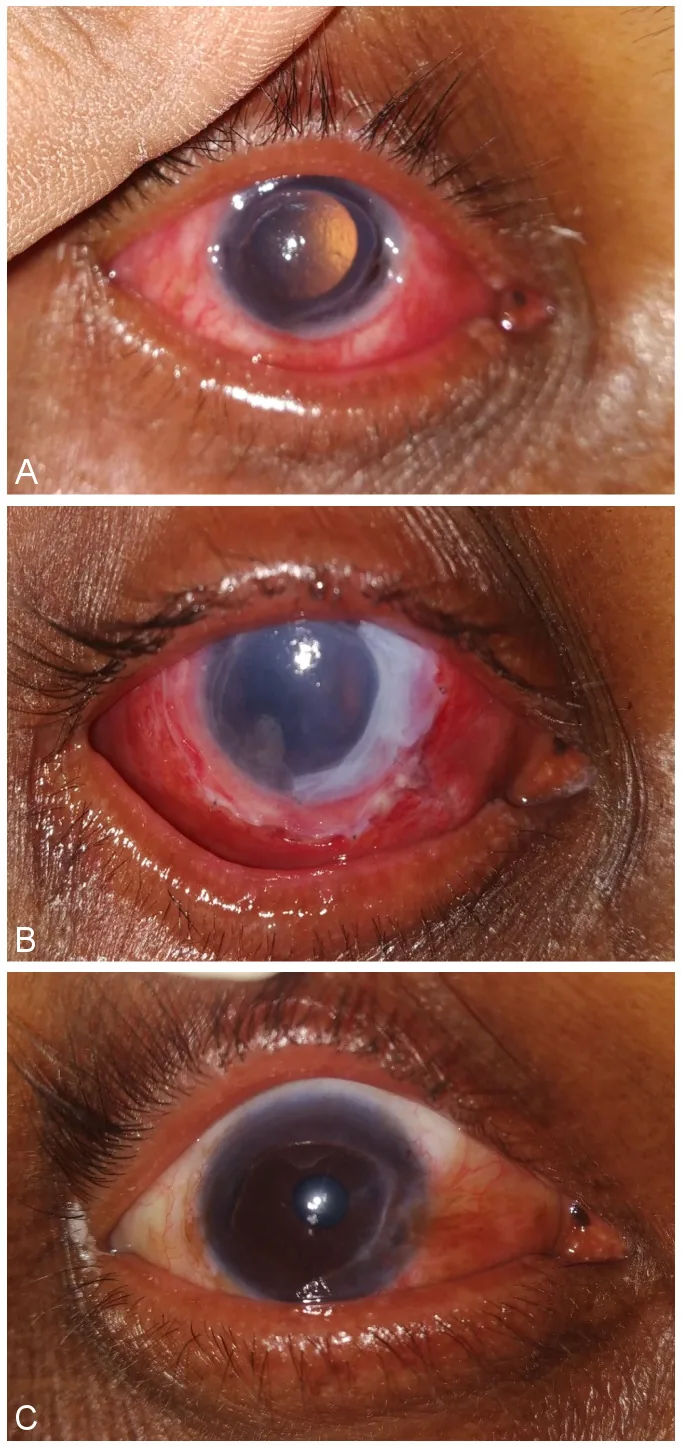
Panigrahi S, Swain P, Nanda A, et al. Tenon’s patch graft to the rescue during COVID-19 pandemic. GMS Ophthalmol Cases. 2023 Mar 1;13:Doc10. Figure 1. PMCID: PMC10073980. License: CC BY.
A: Preoperative Mooren ulcer with impending perforation; B: 1 day postoperatively; C: 1 month postoperatively. After amniotic membrane transplantation, the ocular surface re-epithelializes, and the condition progresses from a high perforation risk to stabilization.
The basic steps of the amniotic membrane graft technique combined with pterygium surgery are described below.
Preparation of amniotic membrane: Remove from storage container, wash with antibiotic (flomoxef sodium 50 mg/mL in saline), then soak in saline. Confirm orientation and remove excess chorionic membrane.
Orientation check (sponge technique): Apply a saline-moistened sponge to the amniotic membrane. On the chorionic side, the membrane adheres to the sponge and lifts; on the epithelial side, it does not lift.
Placement and suturing of amniotic membrane: Place the membrane with the epithelial side up on the sclera and suture with 10-0 nylon. Avoid perforating the sclera when passing the needle (approximately one-third depth of the sclera).
Trimming: After trimming the superior and inferior portions of the membrane, excise near the limbus. Trimming too close to the suture site may cause postoperative rolling of the membrane.
Conjunctival suturing: Suture the conjunctiva to the amniotic membrane and sclera with 7-0 absorbable suture.
Placement of protective soft contact lens: Used to relieve postoperative pain and promote epithelial regeneration.
Mitomycin C (0.04%, applied for 3 minutes) is placed on the sclera and under the conjunctiva after excision of proliferative tissue, prior to amniotic membrane transplantation. After removal, irrigate thoroughly with 200 mL of saline.
Administer antibiotic and steroid eye drops. Continue steroids for at least one month, and switch to a lower potency formulation depending on the condition.
Assess epithelial progression with fluorescein staining.
In Japan, amniotic membrane transplantation was covered by insurance in 2014. While corneal transplantation is performed under the Organ Transplant Law, the handling of amniotic membrane is not directly regulated by law and is managed according to the guidelines of the Japan Society for Tissue Transplantation.
The following requirements must be met for implementation:
Surgeon criteria: Must be certified as a surgeon based on the amniotic membrane transplantation guidelines established by the Japan Cornea Society and the Japan Cornea Transplant Society.
Facility criteria: Must be registered as a facility performing amniotic membrane transplantation with the relevant regional Bureau of Health and Welfare.
Amniotic membrane supply: Must use amniotic membrane provided by a bank accredited by the Japan Society for Tissue Transplantation.
It is operated by a facility accredited by the Japan Society for Transplantation. Category I accredited banks can supply to other facilities, while Category II banks supply only to their own facility. Certified coordinators are responsible for donor explanation, consent acquisition, amniotic membrane processing and testing, storage, and other tasks.
The main requirements that donor amniotic membrane must meet are as follows.
Donors are pregnant women undergoing elective cesarean section
Negative results on infectious disease screening (HBV, HCV, HIV, HTLV-1, syphilis) within 3 months before the expected delivery date
Negative results on retesting considering a window period of 60 to 90 days after delivery
Negative results on microbiological testing at the time of collection and 1 month after cryopreservation
Cryopreserved at -80°C or lower. Storage period is within 2 years from collection.
QCan amniotic membrane transplantation be performed at any facility?
A
Amniotic membrane transplantation is performed only at certified facilities with certified surgeons. Surgeons must meet the criteria established by the Japan Cornea Society and receive certification, and the facility must also be registered with the regional Bureau of Health and Welfare.
6. Latest Research and Future Prospects (Research-stage Reports)
A device (PROKERA®) in which cryopreserved amniotic membrane is mounted on a plastic ring has been developed1). It can be placed on the ocular surface like a scleral contact lens and does not require sutures, so it can be performed in an outpatient setting. The amniotic membrane usually dissolves within 3 to 5 days. Two multicenter retrospective studies on severe dry eye reported significant improvements in corneal staining scores and ocular discomfort 2 to 7 days after placement1).
A method using dried, gamma-sterilized amniotic membrane together with a bandage contact lens has also been reported1). A retrospective study of 56 eyes showed improvement in corneal epithelial erosion within 1 to 2 weeks. A large-diameter (17 mm) dried amniotic membrane with a central opening has also been developed, which helps reduce visual impairment during wear.
Lyophilized amniotic membrane: Clinical application of lyophilized amniotic membrane, which can be stored at room temperature instead of conventional −80°C freezing, is progressing. This greatly improves convenience in storage and transportation.
Drug-impregnated amniotic membrane: Techniques for impregnating amniotic membrane with antifungal drugs and transplanting it have been reported at the case report level.
Application of 3D printing technology: A rapid amniotic membrane fixation method using a 3D-printed ring has been developed for acute Stevens-Johnson syndrome, and a reduction in surgical time has been reported.
Amniotic membrane extract eye drops: Research on eye drops containing growth factors extracted from amniotic membrane is ongoing.
Jones L, Craig JP, Markoulli M, et al. TFOS DEWS III: Management and Therapy. Am J Ophthalmol. 2025;279:289-386. doi:10.1016/j.ajo.2025.05.039. PMID:40467022.