Stevens-Johnson syndrome (SJS) is an acute mucocutaneous disease characterized by sudden high fever, conjunctivitis, and skin rash followed by erosions and blisters on the skin and mucous membranes throughout the body. Toxic epidermal necrolysis (TEN) is a disease type that includes the severe form of SJS. Many cases have a history of drug administration before onset, and it is also a serious adverse drug reaction. The disease was named after the American pediatricians Albert Mason Stevens and Frank Chambliss Johnson, who reported two children with fever, conjunctivitis, and erosions of the skin and oral mucosa in 1922. Subsequently, in 1956, Alan Lyell reported toxic epidermal necrolysis (TEN), and both were classified as part of the same spectrum of severe drug eruptions.
Classification
Area of skin lesions
SJS
Less than 10% of body surface area
SJS/TEN overlap
10–30% of body surface area
TEN
More than 30% of body surface area
The ocular findings of SJS and TEN are similar, making it difficult to distinguish between the two based solely on eye findings. Therefore, in ophthalmology, SJS and TEN are often collectively referred to as SJS in a broad sense. Their pathogenesis and ocular sequelae are also treated as part of a nearly common spectrum.
The incidence is extremely rare, at a few cases per million people per year, but it affects all ages including children, without gender difference. In the United States, an incidence of 12.35 cases per million per year has been reported8). Mortality rates are high: 4.8% for SJS and 14.8% for TEN3), with some reports indicating up to 30% for TEN1).
The frequency of ocular complications in SJS/TEN is approximately 70%, occurring in 53–88% of adults8). Severe ocular complications involving both pseudomembrane and keratoconjunctival epithelial defects are seen in about 40% of all SJS/TEN cases10). Due to the high mortality rate, systemic management is the main focus at onset, but the most common sequelae are ocular disorders, including visual impairment due to severe corneal opacity and dry eye that persist throughout life11). In cases that progress to corneal epithelial stem cell deficiency, the corneal epithelial cells that should be supplied centripetally from the limbus become insufficient, and conjunctiva-derived tissue with blood vessels invades the corneal surface. This irreversible change is central to visual impairment, so the quality of acute-phase treatment within days of onset greatly influences prognosis13).
SJS/TEN is often recognized in pediatrics, dermatology, and emergency medicine, but in cases where ocular symptoms precede skin lesions, patients may first visit an ophthalmologist. In presentations with systemic fever and rash, differentiation from acute bilateral conjunctivitis is always a concern. Therefore, even general ophthalmologists need to facilitate early diagnosis and multidisciplinary treatment, keeping interprofessional collaboration in mind. At the initial visit, systemic symptoms and skin/mucous membrane findings should not be overlooked; when bilateral conjunctivitis is accompanied by fever, active collaboration with dermatology and emergency medicine is necessary. In suspected cases, early hospitalization and aggressive acute-phase ophthalmic intervention are directly linked to improved visual prognosis.
QWhat is the difference between SJS and TEN?
A
SJS and TEN are diseases on the same spectrum, classified by the area of skin involvement. Less than 10% of body surface area is SJS, 10–30% is SJS/TEN overlap, and more than 30% is TEN. Ocular findings are similar and difficult to differentiate, so in ophthalmology they are collectively referred to as SJS in a broad sense. Mortality rates are 4.8% for SJS and 14.8% for TEN3). The incidence of severe ocular complications is approximately 40% overall in SJS/TEN10).
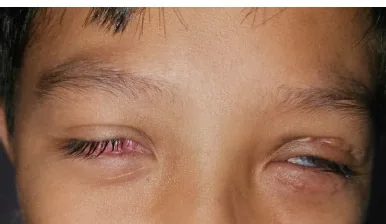
Wibowo E, Maharani RV, Sutikno NA. Symblepharon as Ocular Manifestation Post Stevens-Johnson Syndrome: A Rare Case. Romanian Journal of Ophthalmology. 2024 Oct-Dec; 68(466):$2. Figure 1. PMCID: PMC11809831. License: CC BY.
Both eyes are narrowed and cannot open fully; the right anterior segment is covered with scars and granulation tissue, and the left eye shows narrowing and scars after eyelid transplantation. This presents severe chronic ocular surface changes in the main symptoms and clinical findings.
Bilateral conjunctival hyperemia, foreign body sensation, and ocular pain: Ocular symptoms occur simultaneously or within a few days before the onset of a rash mainly on the trunk.
Decreased visual acuity: Caused by corneal and conjunctival epithelial defects in the acute phase and corneal opacity in the chronic phase.
Dryness and photophobia: Persist due to dry eye in the chronic phase.
Malaise and sore throat: Many patients experience these as cold-like prodromal symptoms preceding the onset.
Clinical Findings (Findings Confirmed by Physician Examination)
Bilateral conjunctival hyperemia: Severe hyperemia occurring almost simultaneously with mucosal and skin rashes.
Pseudomembrane formation: A characteristic finding in the acute phase, adhering to the conjunctival surface in a wing-like shape.
Corneal and conjunctival epithelial defects: May be extensive. Persistent epithelial defects can lead to corneal infection, melting, or perforation.
Eyelid redness and swelling: In severe cases, the eyelids cannot be opened. Loss of eyelashes may also occur.
Corneal pseudomembrane: May appear a few days after hospitalization4).
Acute ocular findings directly linked to severity classification: The acute ocular severity classification by Sotozono et al. divides into Grades 0 to 3 based on the presence of pseudomembrane, epithelial defect, and corneal epithelial defect11).
If a patient visits an ophthalmologist before noticing the rash, it may be misdiagnosed as viral conjunctivitis. It is essential to check for fever and systemic rash.
Chronic phase (scarring phase)
Severe dry eye: Tear secretion deficiency due to obstruction of the lacrimal gland ducts occurs in almost all cases. Meibomian gland dysfunction is also frequently present.
Trichiasis: Persists for many years and worsens the ocular surface condition. Often requires removal 3–4 times per month according to the hair cycle.
Symblepharon: The fornix disappears, and the palpebral conjunctiva adheres to the bulbar conjunctiva.
Conjunctival invasion of the cornea: When corneal epithelial stem cells are lost, conjunctival tissue covers the corneal surface, causing visual impairment.
Epithelial keratinization: In severe cases, the keratoconjunctival surface becomes keratinized like skin.
Loss of palisades of Vogt: This is a clinical sign indicating the loss of corneal epithelial stem cells at the limbus.
The severity of ocular complications does not necessarily correlate with the extent of skin lesions. Cases have been reported where more severe damage occurred in the eye not receiving eye drops compared to the contralateral eye, indicating that SJS/TEN is fundamentally a systemic immune disease1).
The presence of pseudomembrane formation, corneal epithelial defects, and conjunctival hyperemia in the acute phase are important factors for predicting the development of ocular complications. A Japanese multicenter study reported that cases with pseudomembrane formation or corneal epithelial defects in the acute phase had a high rate of severe chronic ocular sequelae11). Therefore, detailed ocular findings should be recorded daily or every few days during the acute phase, and grading should be followed over time.
SJS/TEN is often triggered by drug administration. In children, it is frequently preceded by Mycoplasma infection. Many patients experience cold-like symptoms such as malaise and sore throat before onset, and some viral infection is thought to be a trigger, but the detailed mechanism of onset remains unknown. The latency period from the start of drug administration to onset is relatively short, typically 4 days to 1 month, with the most frequent onset within 2–3 weeks after starting the suspected drug. However, cases of onset after long-term administration also occur, so the duration of administration alone cannot rule out a causal relationship.
Cause Category
Representative Drugs/Factors
Antibiotics
Sulfa drugs (e.g., ST combination) are the most common
Antiepileptic drugs
Carbamazepine, phenytoin, lamotrigine
Analgesic and antipyretic drugs
Nonsteroidal anti-inflammatory drugs (NSAIDs)
Uric acid-lowering drugs
Allopurinol
Antineoplastic drugs
Immune checkpoint inhibitors (ICIs)
Infections
Mycoplasma infection (especially in children), herpes simplex virus
Many cases have been reported, particularly with antiepileptic drugs. Cases have been reported where symptoms developed 35 days after combined use of carbamazepine and phenytoin 3), and where TEN developed after switching to lamotrigine 7). The contribution of NSAIDs to onset is presumed to involve prostaglandin production inhibition as a mechanism.
In recent years, SJS/TEN caused by immune checkpoint inhibitors (ICIs) has also been reported. In a post-marketing survey of tislelizumab, 3 cases of TEN were identified among 3,795 adverse events 5). The median time to onset of ICI-induced SJS/TEN is 32 days, and a report of 305 cases followed up found 69 deaths 4).
Eye drops can also induce SJS/TEN. A case has been reported where brinzolamide eye drops, a sulfonamide carbonic anhydrase inhibitor, caused systemic SJS/TEN overlap (99% body surface area) 1). Systemic absorption through the conjunctiva and nasal mucosa is thought to trigger a systemic immune response in genetically susceptible individuals.
SJS/TEN after COVID-19 vaccination has also been reported 2). Vaccine-induced SJS/TEN tends to develop within 1–8 days, which is shorter than drug-induced SJS/TEN (2–3 weeks) 2).
HLA genotypes are strongly associated with SJS/TEN susceptibility. Testing for HLA-B58:01 before allopurinol administration and HLA-B15:02 before carbamazepine administration is recommended 8). Furthermore, in Japanese SJS/TEN patients with severe ocular complications, HLA-A*02:06 has been reported to show a strong association 12). Analysis of these HLA polymorphisms plays an important role in identifying causative drugs and pre-medication screening.
QWhich drugs cause SJS/TEN?
A
The most common causative drugs are sulfonamides (antibiotics) and antiepileptic drugs (carbamazepine, phenytoin, lamotrigine), followed by NSAIDs and allopurinol. In recent years, reports due to immune checkpoint inhibitors (ICIs) have also increased 5)6). Eye drops (brinzolamide) can also trigger systemic SJS/TEN 1). Onset after COVID-19 vaccination has also been reported 2). Specific HLA polymorphisms such as HLA-B58:01, HLA-B15:02, and HLA-A*02:06 determine susceptibility 8)12).
SJS diagnostic criteria (3 required items)10): (1) Severe mucosal lesions at the mucocutaneous junction (hemorrhagic or congestive), (2) Erosions or blisters covering less than 10% of the body surface area, (3) Fever of 38°C or higher. SJS is diagnosed when all three major items are met. Accessory findings include atypical target-like erythema multiforme, bilateral nonspecific conjunctivitis (with or without corneal epithelial damage and pseudomembrane formation), and epidermal necrotic changes on histopathology.
TEN diagnostic criteria (3 required items)10): Blisters, epidermal detachment, and erosions covering more than 10% of the body surface area, exclusion of staphylococcal scalded skin syndrome (SSSS), and fever of 38°C or higher.
Even cases diagnosed as SJS may progress to TEN during the peak phase, so reassessment is necessary after initial evaluation 10).
Grading of Ocular Complications
Grade 0: No ocular lesions. Use prophylactic artificial tears 11).
Grade 1: Conjunctival injection only, no corneal lesions. Use antibiotic eye drops 3 times daily and steroid eye drops 6 times daily 8).
Grade 2: Corneal involvement present, no pseudomembrane. In addition to the above, consider amniotic membrane transplantation (Prokera or amniotic membrane transplant; AMT) 8).
Grade 3: Corneal involvement with pseudomembrane. Consider aggressive treatment including AMT 8).
Systemic severity assessment using SCORTEN: SCORTEN (SCORe of Toxic Epidermal Necrosis) is a widely used scoring system for predicting prognosis in SJS/TEN. It evaluates seven items: age ≥40 years, presence of malignancy, heart rate ≥120/min, epidermal detachment area ≥10%, elevated serum urea nitrogen, elevated blood glucose, and low serum bicarbonate. Higher scores indicate increased mortality and provide an objective measure for the need for intensive care and systemic management. Ophthalmologists contribute to treatment decisions by collaborating with dermatologists and emergency physicians and sharing SCORTEN.
Viral conjunctivitis: May be misdiagnosed when patients present with only ocular symptoms in the acute phase. Pay attention to the presence of systemic fever and rash.
Ocular cicatricial pemphigoid: Similar as a chronic cicatrizing keratoconjunctivitis. It is an autoimmune disease with a gradual course; impression cytology and immunohistochemistry are useful for differentiating between the two conditions.
Staphylococcal scalded skin syndrome (SSSS): Must be excluded according to TEN diagnostic criteria. SSSS mainly occurs in children, and epidermal detachment occurs at the granular layer level, a superficial condition that is histopathologically distinct from TEN, which causes necrosis down to the dermis.
Blepharitis/Meibomian gland inflammation: Considered in the differential diagnosis for chronic eyelid margin changes, but distinguished by the presence or absence of scarring.
Systemic treatment: Steroid pulse therapy (methylprednisolone 500–1,000 mg/day for 3 days, 1–2 courses) is initiated early after onset10). In severe cases, IVIG therapy (0.4–1.0 g/kg/day for 3–5 days) or plasma exchange is added. Early high-dose administration, as permitted by the patient’s general condition, is important to suppress the progression of ocular surface inflammation. Options include adding cyclosporine (3–5 mg/kg/day) or TNF-α inhibitors such as etanercept and infliximab, which have been reported effective particularly in steroid-resistant or persistent cases. Systemic management in a burn unit or intensive care unit—including temperature control, fluid management, nutritional support, and infection prevention—is essential, and multidisciplinary team-based comprehensive treatment is provided.
Ocular topical treatment: Betamethasone eye drops or ointment is applied frequently, 6–10 times daily, to prevent symblepharon formation. Antibiotic eye drops are used concomitantly for infection prevention. Whether corneal epithelial stem cells can be preserved is the most critical factor determining visual prognosis in the chronic phase11)13).
Early amniotic membrane transplantation (AMT): Considered for Grade 2 or higher8). A report indicates that BCVA 20/20 was achieved in 9 out of 10 extremely severe cases8). Since infectious keratitis occurs in 35% of cases, additional antibiotic prophylaxis is needed8). Ophthalmic evaluation within 24–48 hours of onset and early AMT intervention improve visual prognosis13). Amniotic membrane transplantation can be performed by suturing to cover the bulbar conjunctiva, fornix, and palpebral conjunctiva entirely, or by using a sutureless ring device such as Prokera. Prokera can be placed in a treatment room, avoiding invasive surgery in the acute phase, and its use in clinical settings is expanding. The amniotic membrane has anti-inflammatory, anti-angiogenic, and anti-scarring properties, and promotes ocular surface wound healing by releasing growth factors and anti-inflammatory cytokines.
Chronic Phase Treatment
Dry eye management: Frequent instillation of preservative-free artificial tears, hyaluronic acid eye drops, rebamipide eye drops (enhancing mucin production and anti-inflammatory effects), diquafosol eye drops (promoting water and mucin secretion), and punctal plugs are used. Dry eye in the chronic phase of SJS is not simply a decrease in tear volume but a complex severe dry eye involving lipid layer abnormalities due to meibomian gland dysfunction, mucin deficiency due to goblet cell loss, and conjunctival epithelial keratinization. Therefore, management with a single agent is difficult, and a multi-drug strategy to supplement each component of the tear film is necessary. Since preservatives worsen keratoconjunctival epithelial damage, all eye drops should be preservative-free whenever possible.
Trichiasis management: Regular epilation every 3–4 times per month according to the hair cycle. For fine, depigmented lashes, titanium forceps or suture forceps are effective. In recurrent cases, eyelid surgery for lash root excision or electrolysis (hair root destruction) is added. Trichiasis after SJS differs from typical age-related entropion; it is caused by mild marginal entropion at the posterior lid margin extending to scar tissue at the hair root, altering the direction of lash growth. Therefore, not only simple epilation but also active treatment of the underlying lid margin scarring is necessary. If long-standing trichiasis is left untreated, it can lead to pseudopterygium, corneal astigmatism, and corneal opacity, so early intervention is desirable.
Inflammation management: Low-dose steroid eye drops suppress chronic inflammation and slow the progression of cicatricial changes. Monitor for MRSA/MRSE carriage and select appropriate antibiotics based on culture. In SJS/TEN patients with severe ocular sequelae, the conjunctival sac has a high carriage rate of MRSA/MRSE, which can trigger ocular surface inflammation recurrence or infectious keratitis. Therefore, regular conjunctival sac cultures and consideration of MRSA-effective antibiotics such as vancomycin or linezolid when needed are considered. With chronic steroid eye drops, monitor for elevated intraocular pressure and secondary glaucoma, and perform regular intraocular pressure measurements.
Scleral lenses and visual rehabilitation: Limbus-supported hard contact lenses and scleral lenses are effective for improving visual function in severe dry eye and irregular ocular surface.
Scleral lenses for visual improvement: For severe dry eye with irregular corneal surface, scleral lenses or limbus-supported large-diameter contact lenses such as BostonSight PROSE (Prosthetic Replacement of the Ocular Surface Ecosystem) are useful. By retaining a buffer fluid between the lens and the cornea, they optically correct fine corneal irregularities and maintain a continuous moist environment, thereby suppressing the progression of epithelial damage. In many bilateral SJS patients, not only refractive correction but also reduction of pain, photophobia, and foreign body sensation is achieved.
For severe visual impairment due to conjunctival tissue invasion into the cornea, limbal stem cell transplantation (LSCT) or cultured mucosal epithelial transplantation is performed. There are three types of limbal stem cell transplantation depending on the surgical technique. A systematic review of autologous limbal stem cell transplantation reported that the anatomical/functional success rates for conjunctival-limbal autograft (CLAu) were 81%/74.4%, for simple limbal epithelial transplantation (SLET) 78%/68.6%, and for cultivated limbal epithelial transplantation (CLET) 61.4%/53% 9). CLAu and SLET showed significantly better outcomes than CLET (p=0.0048) 9).
For cultured mucosal epithelial transplantation, a method using autologous oral mucosal epithelial sheets is available, and autologous oral mucosal epithelial transplantation is approved as advanced medical care in Japan 13). In cases such as bilateral SJS where autologous limbal tissue is not available, a small amount of the patient’s own oral mucosa is harvested, expanded into an epithelial sheet in culture medium, and then transplanted onto the corneal surface using amniotic membrane or fibrin glue as a carrier. During the preparation of cultured epithelial sheets, a medium supplemented with retinol and EGF is used to eliminate xenogeneic substances. Combination with mitomycin C to suppress fibroblast activity may also be employed. After transplantation, combined use of steroid eye drops and immunosuppressive agents is continued to prevent recurrence of ocular surface inflammation.
Penetrating keratoplasty (PKP) is considered for cases with corneal scarring, but in the absence of limbal stem cells, epithelialization failure is likely, and the prognosis of PKP alone is limited 8). Therefore, in severe LSCD, a two-stage surgery is often chosen: first, limbal stem cell transplantation or cultured mucosal epithelial transplantation is performed to stabilize the ocular surface, followed by lamellar keratoplasty or penetrating keratoplasty for corneal opacity 13).
The Boston keratoprosthesis (KPro) is used as an option for severe cases where visual recovery is difficult with other treatments 8). In particular, for bilateral SJS cases without autograft sources, type II (mucous membrane-covered) using a titanium optical part and tissue part has been reported as a means to overcome chronic conjunctivalization and symblepharon. However, long-term complications such as glaucoma, retinal detachment, infection, and device exposure are not uncommon, requiring lifelong strict management. In a case of brinzolamide-induced SJS/TEN, PKP was performed for symblepharon and corneal scarring, improving visual acuity to 0.05 1).
Since ocular surface inflammation can recur after ophthalmic surgeries such as cataract surgery, even in mild cases, sufficient anti-inflammatory treatment with oral steroids is necessary postoperatively. Preoperatively, conjunctival sac culture should confirm the presence of MRSA or MRSE, and prophylactic antibiotic eye drops should be administered as needed. For cataract surgery, it is recommended to minimize the wound size, protect the ocular surface with viscoelastic material, and complete the surgery in as short a time as possible.
QWhat is the most important aspect of treatment in the acute phase?
A
Sufficient anti-inflammatory treatment of the ocular surface in the acute phase is most important. Systemic steroid pulse therapy (methylprednisolone 500–1,000 mg/day for 3 days) 10) combined with frequent administration of topical betamethasone eye drops is necessary. If corneal epithelial stem cells can be preserved in the acute phase, corneal transparency is likely to be maintained. For Grade 2 or higher, early amniotic membrane transplantation can be added to expect a good visual prognosis even in severe cases 8).
The pathophysiology of SJS/TEN is explained by an excessive cellular immune response to drug metabolites against a background of genetic predisposition, followed by widespread epithelial cell apoptosis and secondary inflammation and tissue damage. Although the targeting of epidermal and mucosal epithelial cells is common throughout the body, on the ocular surface, the combination of limbal stem cell location, blood flow, and tear film components makes inflammation more likely to persist and directly leads to loss of tissue regenerative capacity.
SJS/TEN is classified as a type IV (delayed-type) hypersensitivity reaction. Drug metabolites presented on MHC class I molecules play a central role, with CD8+ cytotoxic T lymphocytes (CTLs) being key effectors 5). Activated CD8+ T cells secrete TNF-α and IFN-γ, inducing keratinocytes to produce nitric oxide (NO). This NO promotes keratinocyte death via the Fas/Fas ligand pathway 5). Widespread keratinocyte apoptosis leads to full-thickness epidermal necrosis and detachment, observed histopathologically as complete necrosis of the epidermal basal layer. Confirming a positive Nikolsky sign and epidermal basal layer necrosis on skin biopsy is useful for differentiating from conditions such as SSSS.
Granulysin has been identified as a major mediator of keratinocyte death in SJS/TEN 5). NK cells also mediate keratinocyte death through binding of the CD94/NKG2C receptor to HLA-E molecules on keratinocytes 5). TNF-α upregulates cell death-associated molecule expression in the epidermis, ultimately leading to widespread epidermal detachment 5).
Furthermore, vasculitis due to immune complex deposition in the subepithelial vessel walls of the skin and mucous membranes is thought to be involved, with microcirculatory disturbances contributing to erosion formation and delayed wound healing. Inhibition of prostaglandin production, a common mechanism of NSAIDs, is also presumed to be involved in the development of SJS/TEN 13).
In the eye, epithelial detachment and loss of hemidesmosomes can occur before immune cell infiltration 8). Basal vacuolization is observed in early keratinocytes despite the absence of immune cells, suggesting cytokine dysregulation prior to immune infiltration 8). This indicates that ocular surface inflammation may precede or occur concurrently with the systemic drug reaction, providing a rationale for frequent topical steroid administration in the acute phase as a disease-modifying intervention rather than mere symptomatic treatment.
In the later phase, CD8+ cytotoxic T lymphocytes infiltrate and target keratinocytes 8). In the chronic phase, neutrophils persist in conjunctival tissue, potentially driving immune dysregulation and leading to limbal stem cell damage 8). Persistent chronic inflammation progresses conjunctival fibrosis and scarring, which may lead to goblet cell loss, obstruction of accessory lacrimal glands, and meibomian gland dysfunction, ultimately fixing tear film disruption. To break this chronic cycle, long-term suppression with low-concentration steroid eye drops may be used even for mild inflammation.
Anatomy and Mechanism of Corneal Epithelial Stem Cell Loss
Corneal epithelial stem cells reside in the basal layer of the limbal epithelium, accounting for less than 1% of all basal cells. These stem cells proliferate and differentiate while migrating centripetally toward the central cornea, maintaining the turnover of the entire corneal epithelium. An anatomical feature of the limbal epithelium is the presence of radial folds called the palisades of Vogt (POV), which contain abundant blood vessels, nerves, and a specialized microenvironment that constitutes the stem cell niche. POV are normally easier to observe in the superior and inferior quadrants, but may not be clearly visible in healthy eyes of individuals aged 10 years or younger or 70 years and older. Therefore, diagnosis is made not solely by the absence of POV but in combination with findings such as conjunctival epithelial invasion and differences in epithelial staining.
When extensive keratoconjunctival epithelial defects occur in the acute phase and limbal stem cells are lost, conjunctival-derived epithelium covers the corneal surface, leading to opacification and neovascularization. This process is called limbal stem cell deficiency (LSCD)8). SJS is one of the major causes of chronic LSCD, and in a single-center study of 738 eyes, 10.4% were attributed to SJS8). In recent years, attempts have been made to objectively diagnose the severity and distribution of LSCD by combining identification of goblet cells via impression cytology, direct observation of POV basal cells using in vivo confocal microscopy, and layer-specific evaluation of epithelial thickness with anterior segment OCT8).
HLA-A02:06 is strongly associated with SJS/TEN with severe ocular complications in the Japanese population12). Susceptible HLA types have been identified for specific drugs, such as HLA-B58:01 (allopurinol), HLA-B15:02 (carbamazepine), and HLA-B57:01 (abacavir), and premedication screening is increasingly enabling prevention of onset in these areas8). These HLA polymorphisms function as key molecules that determine the interaction between T-cell receptors (TCRs) and drugs/drug metabolites. The hapten hypothesis and the p-i (pharmacologic interaction) hypothesis have been proposed, suggesting that the drug molecule itself or its reactive metabolite directly binds to the peptide-binding groove of the HLA molecule, altering the presentation of self-peptides and inducing an abnormal autoreactive T-cell response. Elucidation of these molecular mechanisms provides a foundation for future prevention strategies and safe drug selection.
In PD-1 inhibitor-induced SJS/TEN, PD-L1 expression, which is not normally detected in healthy skin, is significantly upregulated in lymphocytes and keratinocytes5). This results in keratinocyte death mediated by activated CD8+ T cells5).
QWhy does permanent damage remain in the cornea?
A
In the acute phase, when corneal epithelial stem cells (located in the basal cells of the limbal epithelium) are lost, regeneration of the corneal epithelium becomes impossible. The corneal surface is covered by conjunctival tissue with blood vessels and connective tissue, becoming opaque and irregular. In the chronic phase, the persistent presence of neutrophils drives immune dysregulation and maintains stem cell damage 8). Lacrimal duct obstruction also contributes to tear secretion deficiency, and dry eye and corneal opacity persist throughout life.
With the expanded use of ICIs, reports of SJS/TEN are increasing. In a study of 13 cases (China) of tislelizumab-induced SJS/TEN, 9 were male, with a mean age of 73.15±7.13 years 5). Treatment regimens varied, including steroids alone, steroids+IVIG, and steroids+IVIG+cyclosporine, and 12 patients improved 5).
For a case of tislelizumab-induced SJS/TEN that did not improve with initial steroid and IVIG treatment, improvement was achieved by combining a TNF-α inhibitor (recombinant human TNF receptor II-antibody fusion protein) with blood purification 5). The application of TNF-α inhibitors in the treatment of SJS/TEN is attracting attention as a new therapeutic strategy.
Cultured Corneal Epithelial Sheets and Regenerative Medicine
Regenerative medicine for limbal stem cell deficiency has advanced significantly in recent years. By adding retinol and EGF to the culture medium, it has become possible to produce corneal epithelial sheets without feeder cells or serum, and transplant materials free of xenogeneic substances are being clinically applied 13). Autologous oral mucosal epithelial transplantation can be used as an autologous cell source even for bilateral LSCD and is indicated for severe ocular surface diseases such as SJS 13). SLET is becoming widespread as a simpler and lower-cost surgical technique compared to LSCT, and a review of existing studies has shown superior outcomes over CLET 9). Furthermore, a product in which oral mucosal epithelial cell sheets are adhered to an amniotic membrane substrate has been launched as a regenerative medical product, and clinical application for bilateral LSCD is progressing. Clinical research on iPS cell-derived corneal epithelial cell sheets is also being conducted in Japan, and they are expected as a next-generation treatment for patients with bilateral diseases who cannot obtain autologous cell sources.
It has been reported that sulfonamide eye drops can also cause systemic SJS/TEN. A systemic reaction covering 99% of the body surface area occurred 6 days after starting brinzolamide eye drops 1). It has been shown that the absorption route via the conjunctiva and nasal mucosa can trigger a systemic immune response in genetically susceptible individuals 1). This finding indicates that even eye drops used in ophthalmology can trigger severe systemic drug eruptions, and careful judgment is required when prescribing to patients with a history of drug allergy.
Cases of SJS/TEN complicated by fulminant type 1 diabetes mellitus have been reported 3). It is presumed that a systemic immune response destroys pancreatic β-cells, highlighting the importance of blood glucose monitoring during SJS/TEN management 3). Other systemic complications of SJS/TEN include acute interstitial pneumonia, acute kidney injury, liver dysfunction, and coagulation abnormalities, making continuous multi-organ monitoring essential in systemic management.
Patients with SJS/TEN who have severe ocular sequelae require a combination of multiple treatments throughout their lives, including corneal transplantation, limbal stem cell transplantation, artificial cornea, and scleral lenses. In addition, continuous treatment for dry eye, trichiasis, and chronic conjunctivitis, as well as regular visual field and intraocular pressure assessments, and management of secondary glaucoma and cataracts are necessary. Therefore, it is difficult for a single institution or department to manage these patients, and a long-term follow-up system centered on corneal specialists, along with multidisciplinary collaboration with dermatology, rheumatology, dentistry and oral surgery, and rehabilitation medicine, is essential. Low vision care and vocational support are also important for maintaining patients’ quality of life, and early introduction of visual rehabilitation is recommended. Regarding medical expense subsidy systems, severe ocular sequelae associated with SJS/TEN may be partially covered under the designated intractable disease “Severe erythema multiforme (acute phase)” and the framework of corneal diseases as sequelae, so it is desirable to provide information in collaboration with medical social workers.
Lu H, Xu W, Wu Y, Zhang M, Ma S. Ocular administration of brinzolamide leading to Stevens-Johnson syndrome/toxic epidermal necrolysis overlap: A case report and review. Medicine. 2025;104(49):e46362. doi:10.1097/MD.0000000000046362. PMID:41366987; PMCID:PMC12689009.
Jessica J. Padniewski, Erick Jacobson‐Dunlop, Sam Albadri, Sara Hylwa. Stevens–Johnson syndrome precipitated by Moderna Inc. COVID‐19 vaccine: a case‐based review of literature comparing vaccine and drug‐induced Stevens–Johnson syndrome/toxic epidermal necrolysis. Int J Dermatology. 2022;61(8):923-929. doi:10.1111/ijd.16222.
Zhang X, Huang D, Lou D, Si X, Mao J. Stevens-Johnson Syndrome/Toxic epidermal necrolysis complicated with fulminant type 1 diabetes mellitus: a case report and literature review. BMC endocrine disorders. 2024;24(1):172. doi:10.1186/s12902-024-01683-5. PMID:39218880; PMCID:PMC11367887.
Zhou Y, Xue H, Lu C, Zhang Y, Wu Q, Zhang J, et al. Treatment of Tislelizumab-Induced Toxic Epidermal Necrolysis and Agranulocytosis: A Case Report and Literature Review. Current drug safety. 2025;20(3):361-365. doi:10.2174/0115748863297885240604111018. PMID:38910480; PMCID:PMC12307955.
Yu H, Li Y, Qu X, Zhu J, Liu Z, Mu Z. Stevens-Johnson syndrome/toxic epidermal necrolysis induced by tislelizumab: a case report and literature review. Frontiers in immunology. 2025;16:1689877. doi:10.3389/fimmu.2025.1689877. PMID:41346629; PMCID:PMC12672898.
Zhang M, Wu R, Jia M, Sun S, Zhang L, Tang T. Sintilimab-induced erythema multiforme drug eruption in the treatment of sigmoid colon cancer: A case report and literature review. Medicine. 2023;102(41):e35659. doi:10.1097/MD.0000000000035659. PMID:37832081; PMCID:PMC10578730.
Zhang L, Yang P, Zhu Y, Liu K, Sun Z. Toxic epidermal necrolysis following lamotrigine replacement therapy in a woman planning pregnancy: a case report and literature review. BMC Womens Health. 2025;25:371. doi:10.1186/s12905-025-03796-y.
Jennifer C. W. Hu, Danielle Trief. A narrative review of limbal stem cell deficiency & severe ocular surface disease. Ann Eye Sci. 2023;8:13-13. doi:10.21037/aes-22-35.
Shanbhag SS, Nikpoor N, Rao Donthineni P, Singh V, Chodosh J, Basu S. Autologous limbal stem cell transplantation: a systematic review of clinical outcomes with different surgical techniques. The British journal of ophthalmology. 2020;104(2):247-253. doi:10.1136/bjophthalmol-2019-314081. PMID:31118185.
Sotozono C, Ueta M, Nakatani E, Kitami A, Watanabe H, Sueki H, et al. Predictive Factors Associated With Acute Ocular Involvement in Stevens-Johnson Syndrome and Toxic Epidermal Necrolysis. American journal of ophthalmology. 2015;160(2):228-237.e2. doi:10.1016/j.ajo.2015.05.002. PMID:25979679.
Ueta M, Tokunaga K, Sotozono C, Inatomi T, Yabe T, Matsushita M, Mitsuishi Y, Kinoshita S.. HLA class I and II gene polymorphisms in Stevens-Johnson syndrome with ocular complications in Japanese. Mol Vis. 2008;14:550-555. PMID:18385790; PMCID:PMC2274925.
Kinoshita S, Koizumi N, Ueta M, Sotozono C. New surgical approaches to the management of Stevens-Johnson syndrome and toxic epidermal necrolysis. Cornea. 2015;34 Suppl 11:S97-S103.
Copy the article text and paste it into your preferred AI assistant.
Article copied to clipboard
Open an AI assistant below and paste the copied text into the chat box.