Pterygium is a chronic degenerative disease in which fibrovascular proliferative tissue originating from the conjunctiva invades the cornea. It most commonly occurs on the nasal side of the cornea and forms a triangular shape extending toward the corneal center1). The name “pterygium” is derived from its wing-like triangular appearance. Histopathologically, it is characterized by subconjunctival connective tissue proliferation, elastoid degeneration of collagen fibers, and chronic inflammatory cell infiltration predominantly of lymphocytes. The condition develops and progresses on a background of age-related changes, with cumulative chronic ultraviolet exposure and dryness stimuli.
Pterygium involves not only migration and proliferation of conjunctival epithelial cells onto the cornea but also proliferation of subepithelial fibrovascular tissue. The key distinction from age-related pinguecula is that pterygium is an active proliferative lesion, not merely an extension of the conjunctiva.
Pterygium occurs overwhelmingly on the nasal side. Bilateral involvement on both the nasal and temporal sides occurs in 2–3% of cases, and temporal-only occurrence is limited to 1–2%. It is usually unilateral, but approximately 10% of cases are bilateral1). In bilateral cases, there is generally no significant difference in UV exposure between the two eyes.
Anatomically, pterygium is divided into the following four parts.
Cap: Avascular white tissue extending onto the cornea; firmly adherent to the corneal stroma
Head: The most prominent portion on the cornea
Neck: The raised proliferative tissue on the cornea
Body: The proliferative tissue on the sclera
On the corneal side of the cap, Stocker’s line (arcuate iron deposit) may be observed—an important sign of chronic progression. The cap is firmly adherent to the corneal stroma, but near the limbus the adhesion is loose enough to pass a probe beneath the lesion. This finding helps differentiate true pterygium from pseudopterygium.
Pterygium is a widely recognized ocular surface disease worldwide, with particularly high prevalence in regions near the equator where ultraviolet exposure is high1). Population-based studies around the world have reported the following prevalence rates1).
Tibet (China): approximately 14.5%
Victoria, Australia: 6.7%
Beijing Eye Study (China): 10.1% (10-year incidence)
Spanish general population: 5.9%
Andhra Pradesh Eye Disease Study (India): 9.5%
Meiktila Eye Study (central Myanmar): 19.6%
Men are affected approximately twice as often as women, and prevalence increases with age. Patients seeking treatment are most commonly in their 50s to 70s. Pterygium surgery is one of the most frequently performed ophthalmic procedures worldwide1)2). In Japan, pterygium is a representative conjunctival disease, with many consultations among middle-aged and older adults engaged in outdoor occupations such as agriculture, fishing, and forestry. Regional differences in UV exposure are reflected in the prevalence, which is considered relatively higher in areas with high ultraviolet radiation, such as Okinawa Prefecture and southern Kyushu.
Epidemiologically, age, sex, occupation, and latitude of residence are major determinants, with prevalence exceeding 10% in some regions among middle-aged and older male outdoor workers. Although rare in younger age groups, cases in individuals in their 30s are occasionally seen in areas with high UV exposure such as Okinawa and southern Kyushu. Early-onset cases are known to have a high recurrence rate, making surgical indication assessment and postoperative management particularly important.
In a large-scale study by Oke et al. using the US IRIS Registry (102,138 pterygium surgeries), tissue transplantation (conjunctival autograft, limbal conjunctival autograft, amniotic membrane graft) was performed in 83.0% and the bare sclera method in 15.3% of cases. Cornea specialists were more likely to use tissue transplantation, and it was pointed out that promoting evidence-based surgical technique selection remains a challenge2).
QWhat is the difference between pterygium and pinguecula?
A
Pterygium involves fibrovascular tissue of the conjunctiva invading the cornea, whereas pinguecula remains a yellowish-white small elevation on the conjunctiva adjacent to the limbus and does not invade the cornea. Pinguecula may progress to pterygium in some cases. See the Causes and Risk Factors section for details.
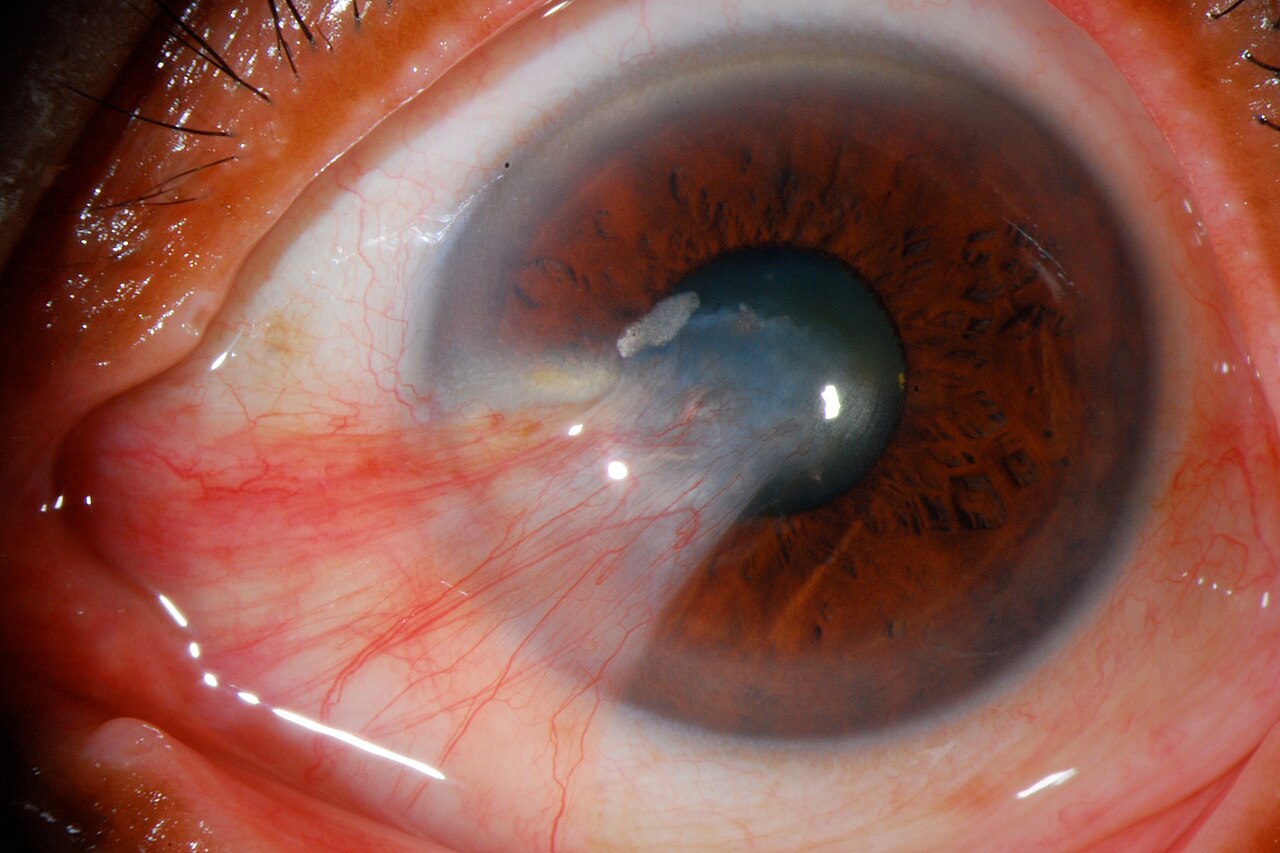
Jmvaras José Miguel Varas, MD. Pterygium Slitlamp.jpg. Wikimedia Commons. License: CC BY 3.0.
White fibrous tissue with blood vessels extends in a triangular shape from the conjunctiva of the palpebral fissure toward the central cornea. As it progresses, it approaches the pupillary area, causing irregular astigmatism and decreased visual acuity.
The chief complaints of patients with pterygium can be broadly classified into three categories.
Foreign body sensation: Tends to occur when the pterygium head is prominently elevated. May be accompanied by dry eye-like symptoms due to abnormal tear distribution.
Hyperemia: Prominent when blood vessels in the body of the pterygium are abundant. Many patients seek consultation for cosmetic reasons.
Visual disturbance: When corneal invasion exceeds approximately 2 mm, regular and irregular astigmatism develop, leading to decreased visual acuity.
When the pterygium head is prominently elevated, it can cause abnormal tear distribution, leading to epithelial damage and dellen formation in the adjacent peripheral cornea. In advanced cases, diplopia due to restricted ocular movement may also occur.
In the early stages, patients often notice it due to cosmetic concerns such as “the white part of the eye looks slightly raised” or “red blood vessels are noticeable on the nose side of the eye when looking in the mirror.” Redness worsens transiently and tends to intensify with stimuli such as strong sunlight, pollen, dryness, and cigarette smoke.
Slit-lamp microscopy reveals a triangular, white, membrane-like tissue with abundant blood vessels, extending from the inner canthus toward the center of the cornea. In typical cases, diagnosis is relatively easy and can be made after examining only a few cases. Pterygium is generally described by a series of findings: congestion of the nasal bulbar conjunctiva, elevation of the pterygium body, corneal invasion of the head, and grayish-white discoloration of the cap tip. These findings are combined to determine the stage and activity.
When the body shows severe congestion with dilated, tortuous blood vessels, the pterygium is assessed as highly active with a high risk of progression and recurrence. Conversely, an “atrophic type” pterygium with thin blood vessels, a thin and translucent body, and nearly arrested progression may reasonably be managed with observation alone without rushed surgery.
Atypical cases also exist, such as those where the tip does not form a triangle or where the tip forms two heads. Additionally, even if it appears to be a pterygium at first glance, careful observation may rarely reveal a tumor such as squamous cell carcinoma; therefore, differential diagnosis is necessary if findings are abnormal.
In clinical practice, classification based on the extent of the lesion is used to determine surgical indications.
Grade
Extent of Progression
Grade 1
Remains near the corneal limbus
Grade 2
Proliferation beyond the limbus
Grade 3
Extends to the pupil
Grade 4
Extends beyond the pupil
The Eguchi classification is used as an indicator of the extent and activity of the lesion. Internationally, the Tan classification is widely used, which evaluates the thickness of the pterygium based on the visibility of the episcleral vessels through the lesion11).
T1 (atrophic): A thin pterygium through which episcleral vessels are clearly visible
T2 (intermediate): Intermediate type
T3 (fleshy): A fleshy pterygium through which episcleral vessels cannot be seen. High recurrence rate
Whether the pterygium is fleshy or not, as well as the patient’s age, are important factors in assessing surgical indications and recurrence risk. Recurrence rates are higher in young patients, cases with fleshy pterygia, and cases with nevi or pigmentation1). In addition to the Tan classification, attempts are being made to stratify recurrence risk preoperatively by also evaluating vascular density and the degree of fibrosis11).
Clinically, the distance from the corneal center to the pterygium is recorded in millimeters as the corneal invasion length (distance from the head apex to the limbus). It is thought that irregular astigmatism begins to occur when the invasion length exceeds 2 mm, and the visual axis begins to be affected when it exceeds 3 mm. Corneal topography reveals flat meridians extending radially from the pterygium head, serving as an indicator of postoperative corneal shape normalization.
The most established cause of pterygium development is ultraviolet (UV-B) exposure1). Chronic UV stimulation damages corneal limbal stem cells, accelerates the proliferation of subconjunctival tissue, and breaches the Bowman’s membrane barrier, invading between the corneal epithelial basal cell layer and Bowman’s membrane. Near the leading edge, it disrupts Bowman’s membrane and forms adhesions with the superficial stromal tissue.
The “albedo hypothesis” explains the nasal predilection. Ultraviolet light entering from the nasal side of the face passes through the cornea and is focused on the nasal limbus due to the lens effect of the cornea, causing greater damage to nasal limbal stem cells. Computer simulations have also shown that laterally incident UV light converges on the limbus of the opposite (medial canthal) side. Additionally, the caruncle, plica semilunaris, and nasal conjunctiva are anatomically less protected by the eyelids and are more directly exposed to UV radiation.
Other aggravating factors besides UV include aging, male sex, outdoor occupations, and exposure to tobacco smoke. The high prevalence in Arctic and equatorial regions further supports a strong association with UV exposure. Involvement of human papillomavirus and herpes virus has also been suggested.
UV exposure: The greatest risk factor. More common in outdoor workers and residents near the equator1)
Age and sex: Prevalence increases with age, and males are affected approximately twice as often as females
Climate and environment: Exposure to dryness, wind, and dust
Genetic predisposition: Family history has been reported
Smoking/tobacco smoke exposure: Nicotine and cotinine exposure has been reported to alter pterygium cell proliferation and migration1)
Viral infection: Involvement of HPV and HSV has been suggested
Risk factors for recurrence include young age, fleshy and non-transparent pterygium (Tan T3), and severe inflammation1)11). In particular, young patients under 40 years of age have been reported to have higher tissue proliferative capacity compared with older patients, with postoperative recurrence rates increasing several-fold. When considering surgical indications, it is important not to “rush into surgery because the patient is young,” but rather to “explain the risk of recurrence precisely because the patient is young and make a careful decision.”
Outdoor workers: Occupations such as farming, fishing, construction, and forestry that involve long hours outdoors tend to have high levels of UV exposure and faster progression. Even when sunglasses cannot be used regularly due to occupational requirements, we recommend countermeasures such as brimmed hats or windproof goggle-type protective eyewear.
Elderly patients: Often have concurrent age-related tear deficiency and dry eye, which can exacerbate the irritative symptoms of pterygium
History of refractive surgery: When a pterygium develops on the cornea after LASIK or PRK, the surgical plan becomes more complex. Preoperative corneal topographic evaluation is especially important.
Possibility of future glaucoma surgery: Surgery that extensively uses the conjunctiva may reduce the success rate of future trabeculectomy. Choosing a surgical technique that preserves the superior conjunctiva is preferable.
QCan pterygium occur in both eyes?
A
Pterygium is often unilateral, but approximately 10% of cases are bilateral. Cases occurring on both the nasal and temporal sides are seen in 2–3% of cases. Since ultraviolet exposure affects both eyes equally, if pterygium develops in one eye, follow-up observation of the other eye is also important.
The diagnosis of pterygium can be easily made using slit-lamp microscopy. The diagnosis is relatively straightforward based on the characteristic triangular-shaped fibrovascular proliferative tissue on the nasal side. However, when surgery is being considered, it is necessary to examine in detail the extent of the lesion and disruption of limbal function. Slit-lamp findings to record include the degree of vascular dilation and congestion in the body of the pterygium, the thickness of the head, the position of the cap apex (distance from the corneal center), the presence or absence of Stocker’s line, and the presence or absence of dellen formation.
Visual acuity and refraction test: Confirmation of spherical equivalent. This is essential because pterygium is an ocular surface disease that causes visual impairment.
Corneal topography: Quantitatively evaluates the degree of irregular astigmatism. Useful for determining surgical indication.
Keratometry: Assesses changes in corneal curvature.
Probe passage test: Determines whether a probe can be passed under the lesion near the limbus (passable in pterygium, not passable in pseudopterygium).
Pseudopterygium: Develops secondary to chemical injuries of the cornea and conjunctiva, ophthalmic surgery, trauma, corneal ulcers, persistent corneal epithelial defects, corneal infections, and cicatricial conjunctival diseases. While pterygium occurs on the nasal side, pseudopterygium can occur not only on the nasal side but in any direction. Additionally, the proliferative tissue is adherent across the entire corneal surface, and a probe cannot be passed under the lesion- Pinguecula: A yellowish-white small elevation adjacent to the limbus. It does not invade the cornea.
Terrien marginal degeneration: A chronic degeneration accompanied by peripheral corneal thinning; in advanced cases, fibrovascular proliferation on the cornea may resemble pterygium.
Limbal keratoconjunctivitis: Presents with inflammatory nodules and injection at the limbus, similar to the injection of the pterygium body. Differentiate by history and presence of atopic predisposition.
Conjunctivochalasis: A condition in which redundant inferior bulbar conjunctiva causes injection and foreign body sensation, which can exist independently of pterygium. When both are present, evaluate them separately.
Understanding the concomitant and differential diagnoses of pterygium is important in surgical planning. In pseudopterygium, the cornea may be severely thinned, potentially leading to corneal perforation during or after surgery. If anterior segment OCT confirms corneal thinning, consider concurrent superficial keratoplasty using preserved cornea.
If slit-lamp examination reveals atypical pterygium morphology (bifid head, irregular tip, nodular surface, associated hemorrhage or necrosis, etc.), consider the possibility of conjunctival intraepithelial neoplasia or squamous cell carcinoma and always perform histopathological examination of the resected specimen. Although rare, cases have been reported in which patients presenting with a pterygium-like appearance were actually found to have ocular surface squamous neoplasia (OSSN).
Asymptomatic pterygium can be managed with observation alone. For injection and foreign body sensation, provide the following symptomatic treatments.
Low-concentration steroid eye drops: Reduce injection and inflammation
NSAID eye drops: Reduce foreign body sensation and injection
Artificial tears / hyaluronic acid eye drops: Address dry eye symptoms caused by tear film distribution abnormalities
However, pharmacotherapy cannot stop the progression of the lesion, and surgery is necessary for advanced cases. Sun protection with sunglasses and brimmed hats, tear film stabilization with artificial tears, and hyaluronic acid eye drops or 3% diquafosol sodium eye drops for cases with dry eye are also used concurrently. Long-term steroid eye drops carry risks of increased intraocular pressure, posterior subcapsular cataract, and infection; therefore, they should not be used indiscriminately, and intraocular pressure and the lens should be evaluated regularly.
When corneal invasion progresses, causing irregular astigmatism or decreased visual acuity
When restriction of eye movement occurs
Cosmetic concerns
The benefits of surgery and the risk of postoperative recurrence should be fully explained, and the decision should be made in consultation with the patient. It is necessary to explain to the patient that younger patients are more prone to recurrence.
Pterygium surgery consists of excision of the proliferative tissue and reconstruction of the ocular surface. The current standard technique is conjunctival autograft (CAG) or limbal-conjunctival autograft (LCAG)1)11). The combination of conjunctival reconstruction and suppression of proliferative tissue is considered the principle of recurrence prevention, and either a pedicle conjunctival flap, free conjunctival flap, or amniotic membrane covering is selected.
The general surgical procedure is as follows.
Administer topical anesthesia and subconjunctival infiltration anesthesia.
Dissect the pterygium head along with the conjunctiva and Tenon’s capsule from the cornea.
Remove residual tissue on the corneal surface as thoroughly as possible and smooth it with a diamond burr or toothed forceps.
Extensively remove Tenon’s capsule from the body (“wata-nuki”).
If necessary, apply mitomycin C (0.02–0.04%) for 1–3 minutes and rinse thoroughly with saline.
Harvest a conjunctival flap or LCAG flap from the superior bulbar conjunctiva.
Suture or fix the graft flap to the resection site with fibrin glue.
Allow the donor site conjunctival defect to epithelialize naturally, or suture it if small.
Conjunctival Autograft (CAG/LCAG)
Pedicle conjunctival flap transplantation: The conjunctiva adjacent to the resection site is moved to cover the defect. Reconstruction is possible while maintaining blood flow, offering high safety.
Free conjunctival graft (CAG): A conjunctival flap is harvested from another site (usually the superotemporal bulbar conjunctiva) and transplanted. It offers the advantage of being suturable to any desired location.
Limbal conjunctival autograft (LCAG): A conjunctival autograft that includes limbal tissue. Recovery of limbal function leads to an even lower recurrence rate1)9).
Other Reconstruction Methods
Amniotic membrane transplantation: Can cover extensive conjunctival defects. Has anti-inflammatory, anti-angiogenic, and anti-fibroblast proliferation effects. Useful for recurrent pterygium and extensive resection cases10).
Conjunctival rotation flap: The conjunctiva adjacent to the resection site is rotated and used for coverage11).
Fibrin glue: Used as a graft fixation method alternative to suturing. Reduced surgical time and postoperative inflammation have been reported.
The recurrence rates for each pterygium surgical technique are shown below1)9)10).
The bare sclera technique has an extremely high recurrence rate and is no longer recommended1). Conjunctival autograft is the current gold standard, with limbal conjunctival autograft (LCAG) showing the lowest recurrence rate1)9). In a meta-analysis by Zheng et al., LCAG was reported to have a significantly lower recurrence rate compared with bare sclera, conjunctival autograft, and intraoperative MMC therapy (the difference from amniotic membrane transplantation was not significant)9).
The recurrence rate of amniotic membrane transplantation is 3.7–40.9% in the meta-analysis by Li et al., which is higher than that of conjunctival autograft (2.6–17.7%). However, it remains a useful option in patients with extensive conjunctival scarring or those who may require glaucoma surgery in the future10).
In a report by Oke et al. analyzing 102,138 cases from the US IRIS Registry, the 5-year reoperation rate was 7.7% in the tissue graft group and 11.0% in the bare sclera group. The bare sclera technique still accounted for approximately 15% of pterygium surgeries in the United States2).
Differentiating the orientation (inner vs. outer side) of the graft can be a problem when transplanting a free conjunctival flap. A double-flip method for maintaining the correct orientation of the graft has also been reported3).
Öztürk et al. reported a double-flip technique for conjunctival autografting in which three sides of the graft are incised, the graft is flipped over the uncut side and fixed with two sutures, and then the fourth side is cut and re-flipped. This technique reliably maintains the epithelial side and the limbus-fornix orientation of the graft3).
The following adjuvant therapies are used in combination to further reduce the recurrence rate1)11).
Mitomycin C (MMC): A 0.02–0.04% solution is applied to the sclera using a sponge for 1–5 minutes, then thoroughly irrigated. It suppresses subconjunctival fibroblast proliferation. In Japan, this is not covered by insurance, and adequate explanation and consent are required before use. In the RCT by Lam et al., the recurrence rate was 8.3–8.6% in the group receiving 0.02–0.04% MMC applied for 5 minutes, and 22.9–42.9% with 3-minute application, demonstrating the impact of application time8). In a 10-year long-term RCT by Young et al., the recurrence rate was 25.5% in the MMC group versus 6.9% in the LCAG group, showing that LCAG was superior even in the long term7).
5-Fluorouracil (5-FU): Reported to have fewer complications than MMC or beta irradiation. In a comparative study by Silva et al., the recurrence rate was 5.83% in the 5-FU group and 25.5% in the non-use group15).
β-irradiation: Although effective with recurrence rates of 0–11.8%, serious complications such as scleral thinning, scleral melting, perforation, infectious endophthalmitis, and cataract progression have been reported, and it is currently not recommended13)
Anti-VEGF therapy (bevacizumab): Subconjunctival injection and postoperative eye drops have been attempted. A 2018 meta-analysis by Sun et al. reported a reduced recurrence rate at 12 months of follow-up, but the optimal administration method has not been established14)
Cyclosporine eye drops: In a 2017 network meta-analysis by Fonseca et al. (14 interventions, 24 RCTs), conjunctival autograft plus cyclosporine 0.05% eye drops was most effective for preventing recurrence6)
The following eye drop prescriptions are used for postoperative anti-inflammatory control and suppression of subconjunctival proliferative tissue.
Levofloxacin ophthalmic solution (Cravit®) 1.5%: 4 times daily, for 1 week to 1 month postoperatively
Betamethasone sodium phosphate ophthalmic solution (Rinderon®) 0.1%: 4 times daily, continued for approximately 6 months postoperatively
Tranilast ophthalmic solution (Rizaben®) 0.5%: 4 times daily, continued for 6 months postoperatively to suppress subconjunctival proliferative tissue
Some institutions use fluorometholone 0.1% eye drops instead of betamethasone to reduce the risk of intraocular pressure elevation. Hyaluronic acid eye drops are also used concomitantly for epithelial protection. Suture removal is performed at approximately 2 weeks. If left untreated, inflammation persists and may induce recurrence.
With appropriate primary surgery, the recurrence rate can be kept at 1.5–5%. If recurrence occurs, do not immediately perform reoperation; instead, continue steroid eye drops and tranilast eye drops for about six months, monitor the progression of regrowth, and then determine whether reoperation is necessary. This is because the activity of the recurrent proliferative tissue may naturally decrease during six months to one year of observation, at which point reoperation becomes less difficult.
For postoperative persistent epithelial defects, a therapeutic soft contact lens (the product approved in Japan is Alcon Air Optix®) may be used. Made of silicone hydrogel material that can be worn continuously for 30 days, it is expected to promote epithelial adhesion and relieve ocular pain. During wear, if the lens becomes heavily soiled or dry, clean it with saline solution or replace it with a new lens. As a rule, do not use it in the presence of active infection.
Standard postoperative follow-up is scheduled for the next day, 1 week, 2 weeks (suture removal), 1 month, 3 months, and 6 months. Since the majority of recurrences within 6 months occur during this period, adherence to follow-up visits during this time is extremely important. Early signs of recurrence include the observation of fine blood vessels entering the cornea from the edge of the graft flap or the resected area. If detected early, progression may be controlled by intensifying steroid eye drops.
When pterygium recurs, highly active proliferative tissue adheres firmly from the cornea to the medial rectus muscle, making surgery more difficult than the initial procedure. Extensive excision of the lesion, including the area around the medial rectus, is often required, and a combination of amniotic membrane transplantation, mitomycin C application, and autologous limbal transplantation is frequently necessary. Recurrent pterygium surgery often becomes a combined procedure involving multiple techniques such as dissection and re-fixation of the medial rectus muscle, amniotic membrane grafting based on the size of the conjunctival defect, and, when needed, superficial keratectomy.
Regarding the timing of reoperation for recurrent pterygium, performing surgery prematurely while inflammation and proliferation are still highly active risks provoking further recurrence. It is therefore reasonable to first control inflammation with steroid eye drops and proceed with reoperation only after disease activity has subsided. It is important to share with patients a strategy of “not rushing to surgery immediately upon recurrence, but considering reoperation after observing for about six months.”
QHow can recurrence be prevented after pterygium surgery?
A
Performing conjunctival autograft (CAG or LCAG) is the most important measure. Network meta-analysis has shown that combining CAG with cyclosporine 0.05% eye drops is the most effective for preventing recurrence. Continuing postoperative steroid and tranilast eye drops for six months can also reduce the recurrence rate. With appropriate primary surgery, the recurrence rate can be kept to approximately 1.5–5%. Ultraviolet protection is also effective for long-term recurrence prevention.
Damage to corneal limbal stem cells caused by ultraviolet radiation plays a central role in the development of pterygium1). Normal limbal tissue functions as a barrier preventing conjunctival tissue from invading the cornea, but chronic UV-B exposure disrupts this function, leading to pterygium formation. Pterygium is now understood not as a mere age-related conjunctival degeneration, but as a complex pathology combining localized epithelial stem cell damage, fibrovascular proliferation, and chronic inflammation.
p53 mutation and MDM2: Ultraviolet-induced DNA damage causes mutations in the p53 gene. In pterygium tissue, both p53 and MDM2 (mouse double minute 2) expression are elevated, but p53 is predominantly localized in the cytoplasm and barely detected in the nucleus12). As a result, apoptosis is not induced, and p21, a transcriptional target of p53, is also undetected. Dysfunction of the p53-MDM2 pathway is thought to support the survival and proliferation of pterygium cells1)12)
Matrix metalloproteinase (MMP) activation: MMP-1, MMP-2, MMP-9, and others are activated, degrading Bowman’s membrane and the extracellular matrix, thereby promoting tissue invasion
Angiogenic factors: VEGF, bFGF, and others are overexpressed, promoting the abundant formation of new blood vessels in pterygium1)
HIF-1α: Hypoxia-inducible factor expression is upregulated, promoting angiogenesis through the hypoxic response
Oxidative stress: Accumulation of 8-OHdG (an oxidative DNA damage marker) has been reported, suggesting the involvement of oxidative stress1)
Abnormal subepithelial protein deposition: Denatured abnormal aggregated proteins caused by glycation and racemization accumulate beneath the epithelium. Some theories propose that abnormalities in the subepithelial connective tissue constitute the core pathology- Epithelial-mesenchymal transition (EMT): In pterygium epithelial cells, a decrease in native conjunctival epithelial markers and an increase in mesenchymal markers have been reported. Cells that acquire migratory and proliferative capacity through EMT are thought to crawl across the cornea
Telomerase activity and apoptosis suppression: Changes in telomerase activity have been reported in pterygium epithelial cells, enabling sustained cellular proliferation- Viral involvement: Viruses such as HPV and HSV have been detected in pterygium tissue, and it has been suggested that viral infection may contribute to pathogenesis by inducing epithelial degeneration and immune responses
Proliferation of subconjunctival connective tissue and elastoid degeneration of collagen fibers are characteristic findings. Chronic inflammatory cell infiltration predominantly composed of lymphocytes is observed. Pterygium tissue crosses the Bowman’s membrane barrier at the corneal limbus, invades between the corneal epithelial basal cell layer and Bowman’s membrane, destroys Bowman’s membrane near the leading edge, and forms adhesions with the superficial stromal tissue. As the condition progresses, abnormally aggregated proteins that have undergone glycation and racemization deposit beneath the epithelium, and collagen fiber degeneration along with angiogenesis promote remodeling of the subepithelial connective tissue. Such complex tissue remodeling is thought to explain why residual active cells proliferate again with simple excision alone.
7. Latest Research and Future Perspectives (Investigational Reports)
Oke et al. analyzed 102,138 pterygium surgeries from the US IRIS Registry and reported that the bare sclera method was still performed in 15.3% of cases. Compared with the tissue graft group, the bare sclera group had a significantly higher 5-year reoperation rate (11.0% vs 7.7%), and they pointed out that the widespread adoption of evidence-based surgical technique selection remains a challenge2).
Comparison of Surgical Techniques via Network Meta-Analysis
Fonseca et al. conducted a network meta-analysis of 24 RCTs involving 14 interventions and reported that conjunctival autograft combined with cyclosporine 0.05% eye drops was the most effective for preventing recurrence, while bare sclera excision had the highest recurrence rate. However, only studies with follow-up periods of 3 months or longer were included, and the lack of long-term follow-up was noted as a limitation6).
Basic research has reported that Nutlin, which inhibits the MDM2-p53 interaction, exhibits selective toxicity against pterygium cells.
In an in vitro study by Cao et al., Nutlin treatment promoted nuclear translocation of p53, leading to increased p21 expression and induction of apoptosis. At the concentration of Nutlin that killed 50% of pterygium cells, the survival rate of conjunctival cells was 95%. In contrast, at the MMC concentration that showed equivalent cytotoxic effects, the survival rate of conjunctival cells was only 63%12).
These results suggest that Nutlin may have higher selectivity for pterygium cells compared to MMC, and its development as a novel adjuvant therapy is expected.
Collagen matrix implants (which biodegrade in 90–180 days) have been reported to cause less conjunctival inflammation and pain compared to MMC and LCAG1). Combined use with conjunctival autograft has also been reported in cases of scleral thinning caused by MMC.
Cui et al. reported 5 cases of HSK that developed approximately 30 days after pterygium surgery. All cases were male, and 4 of the 5 cases were stromal HSK. HSV-sIgA in tear fluid, PCR, and metagenomic next-generation sequencing (mNGS) were useful for diagnosis4).
Scleritis after pterygium excision is a rare but serious complication, and it can be difficult to distinguish between infectious and autoimmune causes.
Mabrouki et al. reported a case of a 70-year-old man who developed severe scleritis 7 days after pterygium excision. Cultures were negative, but response to antibacterial agents was poor, and the condition dramatically improved with administration of an antifungal agent (voriconazole). It was suggested that the infection may have triggered an autoimmune reaction5).
Exploration of new surgical techniques and materials
For ocular surface reconstruction after excision, research is advancing on the application of cultured conjunctival epithelial sheets, cultured limbal epithelial sheets, and decellularized tissue as alternatives to autologous conjunctiva. In Japan, clinical experience with cultured epidermis and cultured corneal epithelium has been accumulating, and these may be applied in the future to complex pterygium reconstruction after extensive excision. From the perspective of regenerative medicine, functional reconstruction of limbal stem cells has also been suggested as a potential curative treatment for pterygium.
Optimization of anti-VEGF therapy: Establishment of optimal administration methods and timing for bevacizumab is awaited14)
Molecular targeted therapy: Elucidation of the MDM2-p53 pathway is progressing, and the development of selective drugs such as Nutlin is expected12)
Combination with cyclosporine eye drops: Combination with conjunctival autograft has been reported to potentially reduce recurrence rates, and wider clinical adoption is anticipated6)
Advances in surgical instruments and fixation methods: Fibrin glue fixation and the double-flip method are being developed to shorten surgical time and improve reproducibility3)
Preoperative risk stratification: Quantification of recurrence risk using the Tan classification and vascular density is enabling personalized treatment that actively combines adjuvant therapy for thick pterygia, and this approach is becoming more widespread11)
Gene expression analysis: Transcriptome analysis of pterygium tissue has suggested the involvement of the VEGF pathway, inflammatory pathways, and epithelial-mesenchymal transition (EMT) pathway, and the identification of molecular diagnostic and therapeutic targets is progressing1)12)
QWhat happens if pterygium is left untreated?
A
Pterygium gradually progresses toward the center of the cornea. When the corneal invasion exceeds 2 mm, irregular astigmatism begins to develop, and if it reaches the visual axis, it causes significant vision loss. In advanced cases, it may also cause restricted eye movement and diplopia. However, the rate of progression varies greatly among individuals, and in some cases it may remain unchanged for long periods. Even when symptoms are mild, preventive measures such as UV protection are important.
Chu WK, Choi HL, Bhat AK, Jhanji V. Pterygium: new insights. Eye (London, England). 2020;34(6):1047-1050. doi:10.1038/s41433-020-0786-3. PMID:32029918; PMCID:PMC7413326.
Oke I, Elze T, Miller JW, Lorch AC, Hunter DG, Traish AS, et al. The prevalence and recurrence risk of bare sclera pterygium surgery in the United States. The ocular surface. 2023;29:547-549. doi:10.1016/j.jtos.2023.05.006. PMID:37257693; PMCID:PMC11872286.
Öztürk E, Gündüz A. Double Flip Technique for Graft Transfer in Autograft Pterygium Surgery. Turkish journal of ophthalmology. 2023;53(1):67-69. doi:10.4274/tjo.galenos.2022.41387. PMID:36847636; PMCID:PMC9973206.
Cui X, Qiu J, Huang F, Zhang C, Shao T, Wang Y. Herpes Simplex Keratitis as a Complication of Pterygium Surgery. The American journal of case reports. 2024;25:e942401. doi:10.12659/AJCR.942401. PMID:38400535; PMCID:PMC10903527.
Mabrouki FZ, Sekhsoukh R. Scleritis Following Pterygium Excision: Infection, Autoimmunity, or Both?. Cureus. 2021;13(9):e17736. doi:10.7759/cureus.17736. PMID:34659950; PMCID:PMC8491957.
Fonseca EC, Rocha EM, Arruda GV. Comparison among adjuvant treatments for primary pterygium: a network meta-analysis. The British journal of ophthalmology. 2018;102(6):748-756. doi:10.1136/bjophthalmol-2017-310288. PMID:29146761.
Young AL, Ho M, Jhanji V, Cheng LL. Ten-year results of a randomized controlled trial comparing 0.02% mitomycin C and limbal conjunctival autograft in pterygium surgery. Ophthalmology. 2013;120:2390-2395.
Lam DS, Wong AK, Fan DS, Chew S, Kwok PS, Tso MO. Intraoperative mitomycin C to prevent recurrence of pterygium after excision: a 30-month follow-up study. Ophthalmology. 1998;105(5):901-4; discussion 904-5. doi:10.1016/S0161-6420(98)95034-5. PMID:9593395.
Zheng K, Cai J, Jhanji V, Chen H. Comparison of pterygium recurrence rates after limbal conjunctival autograft transplantation and other techniques: meta-analysis. Cornea. 2012;31(12):1422-7. doi:10.1097/ICO.0b013e31823cbecb. PMID:22643650.
Li M, Zhu M, Yu Y, Gong L, Zhao N, Robitaille MJ. Comparison of conjunctival autograft transplantation and amniotic membrane transplantation for pterygium: a meta-analysis. Graefe’s archive for clinical and experimental ophthalmology = Albrecht von Graefes Archiv fur klinische und experimentelle Ophthalmologie. 2012;250(3):375-81. doi:10.1007/s00417-011-1820-8. PMID:21935607.
Kaufman SC, Jacobs DS, Lee WB, Deng SX, Rosenblatt MI, Shtein RM. Options and adjuvants in surgery for pterygium: a report by the American Academy of Ophthalmology. Ophthalmology. 2013;120(1):201-208. PMID: 23062647. doi:10.1016/j.ophtha.2012.06.066.
Cao D, Ng TK, Yip YWY, Young AL, Pang CP, Chu WK, et al. p53 inhibition by MDM2 in human pterygium. Experimental eye research. 2018;175:142-147. doi:10.1016/j.exer.2018.06.021. PMID:29932882.
Ali AM, Thariat J, Bensadoun RJ, Thyss A, Rostom Y, El-Haddad S, et al. The role of radiotherapy in the treatment of pterygium: a review of the literature including more than 6000 treated lesions. Cancer radiotherapie : journal de la Societe francaise de radiotherapie oncologique. 2011;15(2):140-7. doi:10.1016/j.canrad.2010.03.020. PMID:20674450.
Sun Y, Zhang B, Jia X, Ling S, Deng J. Efficacy and Safety of Bevacizumab in the Treatment of Pterygium: An Updated Meta-Analysis of Randomized Controlled Trials. Journal of ophthalmology. 2018;2018:4598173. doi:10.1155/2018/4598173. PMID:30254755; PMCID:PMC6145151.
Silva RSC, Avila MP, Rassi AR, Ximenes L, Silva DS Jr, Paula AC. Intra-operative use of 5-Fluorouracil in pterygium surgery: a comparative study. Semin Ophthalmol. 2013;28:34-36. PMID: 23305439. doi:10.3109/08820538.2012.730101.
Copy the article text and paste it into your preferred AI assistant.
Article copied to clipboard
Open an AI assistant below and paste the copied text into the chat box.