Corneal topography is a test that quantitatively measures the curvature and shape of the anterior and posterior corneal surfaces. Its main purposes are to detect and quantify corneal irregular astigmatism, assess disease progression, and aid in refractive surgery planning.
Historically, in the early 17th century, Scheiner conducted research using corneal reflection, and in the late 19th century, the Placido disk was introduced. Modern devices use concentric rings, slit light, or interferometric light to map the entire cornea with high precision.
Corneal topography is a technique that primarily uses Placido ring reflection to measure the shape (curvature) of the anterior corneal surface. On the other hand, corneal tomography is an advanced technique that uses a Scheimpflug camera or anterior segment OCT to measure the three-dimensional structure of the cornea, including the anterior and posterior surfaces and thickness 1). In clinical practice, topography and tomography are combined for comprehensive corneal evaluation.
Corneal Topography
Measurement target: Shape of the anterior corneal surface
Principle: Primarily Placido ring reflection
Data provided: Corneal power map (curvature)
Advantages: High reproducibility and spatial resolution. Suitable for normal to moderate irregular astigmatism.
Corneal Tomography
Measurement target: Three-dimensional structure of the anterior and posterior corneal surfaces
Data provided: Anterior and posterior curvature, elevation, and corneal thickness maps
Advantages: Allows evaluation of the posterior corneal surface. May be measurable even in the presence of opacity or edema 1).
QWhat is the difference between topography and tomography?
A
Topography is a technique that primarily uses Placido ring reflection to measure the shape (curvature) of the anterior corneal surface. On the other hand, tomography uses a Scheimpflug camera or anterior segment OCT to measure the three-dimensional structure of the cornea, including the anterior and posterior surfaces and thickness. In conditions such as keratoconus, changes in the posterior surface may appear before those in the anterior surface, making tomographic evaluation more important.
Kanclerz P, Khoramnia R, Wang X. Current Developments in Corneal Topography and Tomography. Diagnostics (Basel). 2021;11(8):1466. Figure 1. PMCID: PMC8392046. License: CC BY.
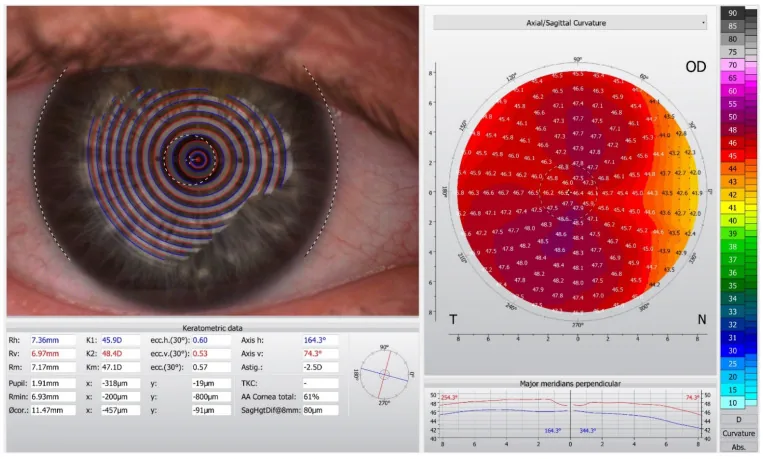
Placido ring reflection image (left) and axial curvature map calculated from concentric ring images (right) obtained with Oculus Keratograph 5M. This corresponds to the Placido ring reflection principle and axial curvature map discussed in the section “Placido-type devices.”
Mire rings (black and white concentric circles) are projected onto the anterior corneal surface (precorneal tear film), and the shape of the reflected image is used to quantitatively measure corneal curvature radius and refractive power. Representative devices: TMS (TOMEY), Atlas, Keratograph.
Advantages: High spatial resolution and reproducibility. Optimal for measuring the anterior corneal surface.
Limitations: Affected by tear film instability. The posterior corneal surface cannot be measured. Only about 60% of the corneal surface is evaluated, limiting detection of peripheral lesions6). In cases of severe corneal irregularity, mire ring visualization becomes difficult.
The mire image of Placido rings can be used to qualitatively assess corneal irregularity without a device, and is particularly useful in pediatric or uncooperative patients4).
A Scheimpflug camera captures rotating slit light to reconstruct the three-dimensional structure of the anterior and posterior corneal surfaces. It enables measurement of anterior and posterior corneal shape, corneal thickness, and total corneal refractive power and higher-order aberrations1). Representative devices: Pentacam (OCULUS), Galilei (dual Scheimpflug + Placido), Sirius (Scheimpflug + Placido).
Advantages: Simultaneous acquisition of anterior and posterior curvature, elevation, and corneal thickness maps.
Limitations: Glare during measurement; in cases of corneal opacity, scattering makes cross-sectional imaging difficult.
Using interferometric analysis, it is less affected by tear film and opacity, and can obtain peripheral information. SS-OCT (wavelength 1,310 nm) is represented by CASIA2 (TOMEY), with a wide measurement range that can display the entire cornea in one image. SD-OCT (wavelength 840 nm) achieves high resolution.
Advantages: Non-contact, fast, and evaluable even in cases of corneal opacity. Minimal influence from the tear film.
Limitations: Not suitable for evaluating tear film breakup (dry eye).
By combining a Placido-type device (corneal topography and aberration measurement) with the Hartmann-Shack method (wavefront sensor for refractive aberration measurement), it is possible to compare corneal refractive data and ocular refractive data.
The characteristics of each device are shown below.
Fix the patient’s head with a chin rest and forehead strap, and have them look straight at the fixation light. Focus and centering adjustments directly affect measurement accuracy. Encourage the patient to open their eyes wide to minimize the effect of the eyelids. Take at least two images to confirm reproducibility.
Contact lens discontinuation period: Contact lenses temporarily alter corneal shape. For accurate data acquisition, hard (RGP) lenses should be discontinued for at least 2 weeks, and soft lenses for at least 1 week. When evaluating suitability for refractive surgery, it is recommended to perform multiple measurements after contact lens discontinuation and confirm reproducibility 6).
When reviewing examination results, first check that focus and centering are within a certain range, and verify that automatic digitization has not misidentified different rings. Then evaluate the power scale using the color-coded map.
Power Map (Axial / Tangential / Refractive): Displays corneal refractive power using color coding. Axial power is based on slope, robust to noise, and suitable for overall astigmatism assessment. Tangential (instantaneous) power reflects local curvature and is excellent for identifying the apex of keratoconus. Refractive power reflects optical properties based on Snell’s law.
Elevation Map: Displays the difference between the corneal surface and a reference sphere as height. Isolated elevations on the anterior and posterior surfaces are important indicators of corneal ectasia6). The posterior elevation map shows high sensitivity and specificity for detecting subclinical keratoconus6).
Pachymetry Map: Displays corneal thickness distribution. In a normal cornea, the center is thinnest and gradually increases toward the periphery. Eccentric thinning suggests corneal ectasia.
Correlate with slit-lamp findings. Be aware of artifacts due to corneal scars, dry eye, and neovascularization.
QHow long is the required contact lens cessation period?
A
Hard (RGP) lenses require cessation for at least 2 weeks, and soft lenses for at least 1 week. Since contact lenses temporarily alter corneal shape, especially for refractive surgery candidacy, it is recommended to perform multiple measurements after cessation to confirm reproducibility 6).
de Paiva Barreto M Jr, et al. Corneal ectasia following photorefractive keratectomy: a confocal microscopic case report and literature review. Arq Bras Oftalmol. 2024;87(6):e2021-0296. Figure 1. PMCID: PMC11629660. License: CC BY.
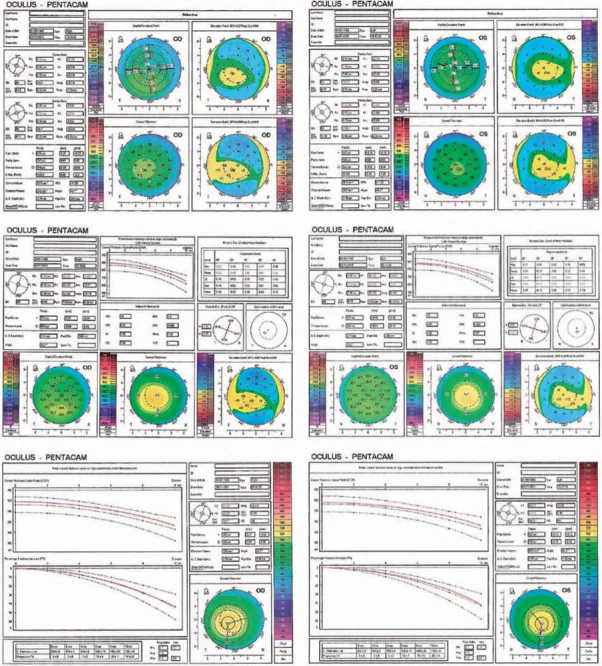
Preoperative corneal tomography of both eyes using OCULUS Pentacam. Four maps (anterior elevation, posterior elevation, axial curvature, and corneal thickness) are displayed, used for shape evaluation in borderline suspected cases. This corresponds to the three-dimensional anterior and posterior evaluation using a Scheimpflug device discussed in the section “Screening and Diagnosis of Keratoconus.”
Corneal topography is the gold standard for early screening of suspected keratoconus6). Early keratoconus often appears normal on slit-lamp examination, and topography may be the only clue.
Placido-based findings: Irregular rings in the central area, inability to project rings in the periphery, and large asymmetric components. Inferior steepening (I-S ratio ≥ 1.2) and skewing of the radial axis >21° are typical patterns 6). The Klyce/Maeda method and Smolek/Klyce method are used as screening indices.
Scheimpflug-based findings: Inferior decentration of the posterior corneal protrusion and corneal thinning can be detected early. The posterior elevation map may appear before anterior changes.
Anterior segment OCT: Thinning of the corneal stroma and central to inferior conical protrusion can be evaluated with a resolution of approximately 10 μm.
The Belin-Ambrosio enhanced ectasia display integrates the corneal thickness spatial profile (CTSP), percentage thickness increase (PTI), and deviations of anterior and posterior elevation on the Pentacam, improving screening accuracy for corneal ectasia5). The tomographic and biomechanical index (TBI) combined with Corvis ST enables comprehensive screening considering corneal biomechanics5).
In temporal keratoconus, the standard I-S ratio may fall within the normal range. In a 14-year-old case, Pentacam detected temporal steepening and thinning, and the T-N (temporal-nasal) ratio was useful for diagnosis 3). This suggests the importance of multifaceted evaluation beyond the I-S ratio.
In pellucid marginal degeneration (PMD), a characteristic inferior steepening called the lobster claw pattern is detected. In a teenage case, the Belin-Ambrosio enhanced ectasia display and corneal biomechanical assessment with Corvis ST were useful for diagnosis 5).
The ABCD classification system is used to assess progression of corneal ectasia. It consists of the following four components 6):
A (Anterior curvature): Anterior curvature in the 3 mm zone of maximum curvature radius
B (Posterior curvature): Posterior curvature in the 3 mm zone of maximum curvature radius
C (Thinnest corneal thickness): Thinnest corneal thickness (μm)
D (Best Corrected Visual Acuity): Snellen visual acuity
Progression is defined as the confirmation of two or more of the following: anterior steepening, posterior steepening, and thinning 6). In children and young adults, progression on tomography has been confirmed in 77% of eyes 7), making regular follow-up important.
QIs corneal topography useful for early detection of keratoconus?
A
Corneal topography is the gold standard for early screening of keratoconus6). Even in early keratoconus where slit-lamp examination appears normal, topography can detect characteristic patterns such as inferior steepening. Combining tomography (e.g., Pentacam) allows evaluation of posterior corneal changes and comprehensive assessment using the Belin-Ambrosio display, enabling earlier detection.
When progression is confirmed by the ABCD classification, corneal cross-linking (CXL) is indicated. After CXL, follow-up every 6 months to 1 year is performed to confirm cessation of progression. Topography and tomography are also used to evaluate corneal shape after CXL.
Exclusion of potential corneal ectasia is essential for determining the indication for refractive surgery 6). If topographic screening reveals abnormalities, surgery should be canceled, and hard contact lenses or corneal transplantation should be considered.
PRK and SMILE are reported to have a lower risk of postoperative corneal ectasia compared to LASIK 6). Postoperatively, topography is used to evaluate dioptric changes in the cornea and detect decentered ablation.
In topography-guided LASIK (e.g., CONTOURA), anterior corneal data acquired with the Topolyzer Vario directly determine the laser ablation pattern 2). The 3Z nomogram has been proposed to address discrepancies between manifest refractionastigmatism and topographic astigmatism2).
Topography is used to evaluate irregular corneal astigmatism before cataract surgery. It contributes to improving the accuracy of toric IOL axis alignment. It is also used for astigmatism evaluation after corneal transplantation, contact lens fitting, and assessment of corneal shape changes due to pterygium.
Additionally, in evaluating irregular astigmatism due to subepithelial infiltrates (SEI) after adenoviral conjunctivitis, Placido ring mires have been reported to detect surface irregularities more sensitively than SS-OCT color maps 4). Serial Placido ring imaging was also useful for monitoring treatment with tacrolimus eye drops 4).
There are three definitions of corneal power used in corneal topography.
Axial power (sagittal power): Pa = (n-1)/d. Calculated from the distance d from the normal line at the measurement point to the reference axis. It is robust to noise based on slope and extends the measurement equivalent to a keratometer to a wide area.
Instantaneous power (tangential power): Pi = (n-1)/r. Calculated from the local radius of curvature r at the measurement point. It reflects local shape changes more accurately but is sensitive to noise.
Refractive power (focal power): Pr = n/f. Based on the focal length f. It most accurately reflects optical properties based on Snell’s law.
Autokeratometers and Placido-based devices measure only the anterior corneal surface and do not consider the posterior surface. Assuming that the shapes of the anterior and posterior surfaces are proportional, the keratometric index (usually 1.3375) is used to calculate total corneal refractive power. This assumption generally holds for normal corneas, but after refractive surgery or in corneal ectasia, the proportional relationship between the anterior and posterior surfaces breaks down, leading to errors 1).
In the Scheimpflug principle, by manipulating the lens plane and image plane so that the tangents drawn from the object plane, lens plane, and image plane intersect at a single point (Scheimpflug intersection), a focused image can be obtained even for non-planar objects 1). This principle enables distortion-free imaging of slit-light corneal cross-sections.
Combining corneal shape analysis with wavefront aberrometry allows quantitative evaluation of higher-order aberrations (coma, spherical aberration, etc.) in addition to spherical and cylindrical errors (second-order aberrations). Aberrations are expanded using Zernike polynomials and quantified as RMS (root mean square) values. In keratoconus, a marked increase in vertical coma aberration is characteristic 6). Some devices can perform topography and aberrometry simultaneously 1).
In recent years, combined devices integrating topography/tomography and biometric measurements (axial length, anterior chamber depth, etc.) have emerged 1). The concept of Total Corneal Refractive Power for intraocular lens power calculation has been proposed, and it is expected to improve the accuracy of power calculation in cataract surgery, especially after refractive surgery 1).
Research on corneal shape analysis using AI (machine learning/deep learning) is progressing. Its application to automatic detection and progression prediction of keratoconus from topography data is being considered, but it is still at the research stage.
Reports of atypical cases such as temporal keratoconus3) indicate the importance of multi-parameter evaluation including not only the standard I-S ratio but also the T-N ratio. As a reassessment of the Placido ring, it has been reported that qualitative evaluation can serve as a simple screening tool for corneal surface abnormalities even in environments where advanced devices are not available 4).
Kanclerz P, Khoramnia R, Wang X. Current Developments in Corneal Topography and Tomography. Diagnostics (Basel, Switzerland). 2021;11(8). doi:10.3390/diagnostics11081466. PMID:34441401; PMCID:PMC8392046.
Khamar P, Shetty R, Annavajjhala S, Narasimhan R, Kumari S, Sathe P, et al. Impact of crossplay between ocular aberrations and depth of focus in topo-guided laser-assisted in situ keratomileusis outcomes. Indian journal of ophthalmology. 2023;71(2):467-475. doi:10.4103/ijo.IJO_191_22. PMID:36727342; PMCID:PMC10228944.
Zhang LJ, Traish AS, Dohlman TH. Temporal keratoconus in a pediatric patient. American journal of ophthalmology case reports. 2023;32:101900. doi:10.1016/j.ajoc.2023.101900. PMID:37546376; PMCID:PMC10400863.
Toyokawa N, Araki-Sasaki K, Kimura H, Kuroda S. Evaluating anterior corneal surface using Placido ring mires for irregular astigmatism in refractory corneal subepithelial infiltrates after adenoviral conjunctivitis. BMC ophthalmology. 2024;24(1):515. doi:10.1186/s12886-024-03774-2. PMID:39609742; PMCID:PMC11603996.
Nelapatla GI, Chaurasia S. Pellucid marginal corneal degeneration in a teenager. BMJ Case Rep. 2022;15:e248599.
Jhanji V, Ahmad S, Amescua G, et al. Corneal Ectasia Preferred Practice Pattern. Ophthalmology. 2024 Apr;131(4):P205-P246. doi:10.1016/j.ophtha.2023.12.038. PMID:38349299.
Meyer JJ, Gokul A, Vellara HR, McGhee CNJ. Progression of keratoconus in children and adolescents. The British journal of ophthalmology. 2023;107(2):176-180. doi:10.1136/bjophthalmol-2020-316481. PMID:34479856.
Copy the article text and paste it into your preferred AI assistant.
Article copied to clipboard
Open an AI assistant below and paste the copied text into the chat box.