SMILE (small incision lenticule extraction) is a refractive surgery that uses a femtosecond laser to create a refractive lenticule (lens-shaped corneal piece) within the corneal stroma and removes it through a 2–3 mm small incision to correct myopia and myopic astigmatism. It fundamentally differs from conventional LASIK and PRK in that it does not use an excimer laser and is completed with a single femtosecond laser device.
Since its clinical introduction in 2008, it has become one of the most widely performed laser refractive surgeries worldwide, with over 8 million procedures performed globally as of the end of 20232). In Japan, it received regulatory approval on March 22, 20231). Initially performed as FLEx (femtosecond lenticule extraction) with a large incision, SMILE with a reduced incision size of 2–3 mm has become the standard technique. Since the first efficacy and safety study by Sekundo et al.13), numerous studies have accumulated, establishing it as a highly effective, safe, and predictable refractive surgery.
The essential feature of this surgery is that it does not create a flap. LASIK first creates a corneal flap, lifts it, and applies excimer laser, whereas SMILE excises only the intrastromal tissue without flap creation. This preserves the structural continuity of the cornea and provides protection to the anterior corneal stroma. Corneal nerve transection is also minimized, resulting in a lower risk of postoperative dry eye compared to LASIK2).
The correction range is up to spherical equivalent of 10 D (myopia ≤10 D, astigmatism ≤3 D) 1). The minimum age is 18 years, and stable refraction is a prerequisite 1). Preoperative corneal topography (including biomechanical evaluation with TBI, CBI, etc.) is mandatory in all cases, and detecting and excluding forme fruste keratoconus is the most critical factor for surgical safety 2).
QHow is SMILE different from LASIK and PRK?
A
SMILE uses only a femtosecond laser and removes a lenticule without creating a corneal flap. LASIK creates a flap and applies an excimer laser, carrying risks of flap-related complications (displacement, folds, epithelial ingrowth, etc.). PRK removes the epithelium and applies an excimer laser, causing more postoperative pain and longer recovery. SMILE has less pain (similar to LASIK), avoids LASIK flap-specific complications, and dry eye is milder than with LASIK. The incidence of postoperative ectasia is also lower than LASIK (11 vs. 90 per 100,000 eyes), offering biomechanical advantages 2). The indication range is up to spherical equivalent of 10 D (myopia ≤10 D, astigmatism ≤3 D), which is slightly narrower than LASIK (myopia, hyperopia, astigmatism) 1).
The following may occur 1–3 days after surgery. They usually resolve within a few days.
Early Postoperative Period (1–7 Days)
Vision recovery: Marked improvement from the next day. In many cases, unaided daily activities are possible from day 1.
Corneal findings: The epithelium at the incision site (2–3 mm) usually heals within 1–2 days. Corneal edema resolves within a few days.
Caution: Excessive eye rubbing can cause epithelial damage at the incision site.
1–3 months postoperatively
Stable period: Refraction and vision gradually stabilize. Refractive values stabilize by 6 months postoperatively.
Dry eye: Temporary dryness may persist. Improves as corneal nerves recover.
Follow-up: Regular check-ups at 1, 3, and 6 months postoperatively are recommended1).
Postoperative complications (caution required)
DLK (diffuse lamellar keratitis): Overall incidence 0.84%2). Often occurs within 1 week postoperatively. Managed with steroid eye drops. Severe cases require interface irrigation.
Corneal ectasia: Global incidence 0.02%2). Strict preoperative screening is essential.
Delayed visual recovery: Overall incidence 1.5%2). Caused by residual refractive error, dry eye, OBL, etc.
QWhen can I return to normal life after SMILE surgery?
A
In most cases, daily activities without glasses are possible the next day. Driving may be possible after vision is confirmed the day after surgery, but follow your doctor’s instructions. Strenuous exercise and contact sports are usually allowed after 1–2 weeks. Activities with infection risk, such as swimming and sauna, are recommended to be avoided for at least 1 month.
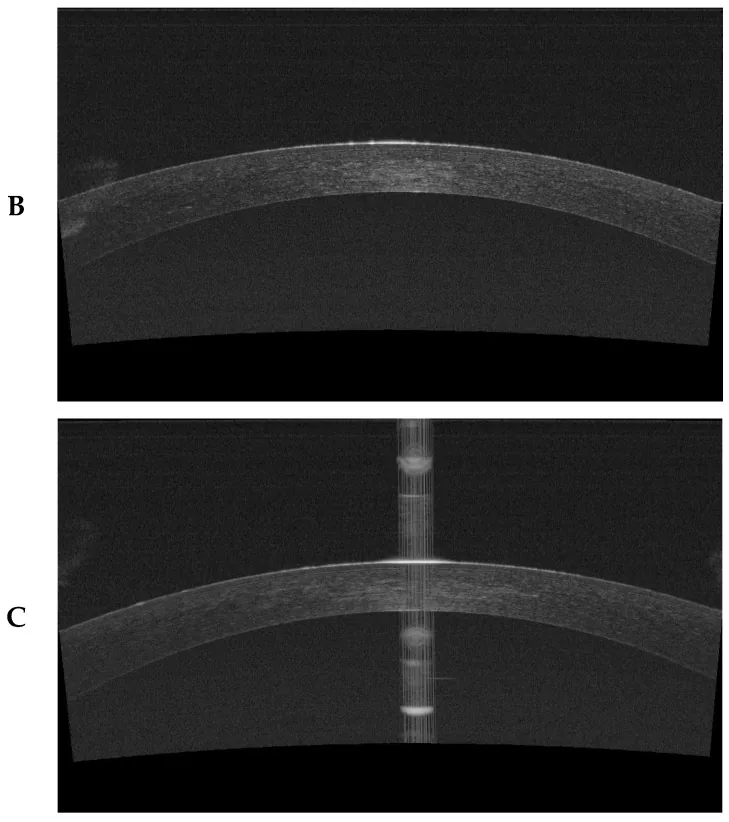
Janiszewska-Bil D, Czarnota-Nowakowska B, Kuciel-Polczak I, et al. Assessment of Changes in Cap and Residual Stromal Thickness Values during a 6-Month Observation after Refractive Lenticule Extraction Small Incision Lenticule Extraction. J Clin Med. 2024;13(7):2148. Figure 1 (panels B and C). PMCID: PMC11012741. DOI: 10.3390/jcm13072148. License: CC BY 4.0.
Two-panel composite image of corneal horizontal section captured by SS-OCT (DRI OCT Triton) after SMILE: (B) Tomographic image of the cap layer showing a uniform hyperintense band of the anterior corneal stroma (cap) and the lenticule extraction cavity beneath it; (C) Residual stromal thickness (RST) measurement image with measurement calipers placed centrally to measure the stromal thickness from the lenticule extraction cavity to the posterior corneal endothelium. Corresponds to the surgical design parameters (RST calculation, cap thickness evaluation) discussed in the section “Diagnosis and Examination Methods.”
The following examinations are performed preoperatively to carefully evaluate indications1).
Examination item
Purpose
Notes
Visual acuity (uncorrected and corrected)
Baseline assessment
Best corrected visual acuity also required
Refraction (subjective, objective, and under cycloplegia)
Keratoconus is an absolute contraindication; overlooking it risks postoperative corneal ectasia. The tomographic and biomechanical index (TBI) shows the highest diagnostic accuracy (SUCRA 96.2%), and comprehensive evaluation combined with CBI (83.8%) is recommended2). Three-dimensional evaluation of the anterior and posterior corneal surfaces and corneal thickness using Scheimpflug tomography (e.g., Pentacam) should always be performed.
Optical zone diameter: 6.0–7.0 mm (larger is better for reducing higher-order aberrations if corneal thickness is sufficient)
Astigmatism correction range: −0.25 D to −5.00 D (accuracy tends to decrease with high astigmatism)2)
QHow long should contact lenses be discontinued before surgery?
A
Soft contact lenses are usually discontinued 1–2 weeks before surgery. Hard contact lenses (rigid gas permeable, scleral lenses) have a greater impact on corneal shape, requiring discontinuation for 3 weeks to 1 month or longer. Preoperative examinations must be performed after contact lens discontinuation. This is an essential step to accurately assess corneal shape.
SMILE surgery is performed as a day procedure under topical anesthesia. The standard steps are as follows2):
Patient setup: Topical anesthesia (e.g., oxybuprocaine), disinfection, and draping. The patient is instructed to focus on a fixation light during the procedure.
Suction ring placement: The eye is fixed and intraocular pressure is kept constant. Maintaining suction during laser delivery is critical. If suction loss occurs, laser delivery is stopped and resumed after reapplication. Suction loss occurs in approximately 0.5–1% of cases, with lower rates in experienced hands.
Femtosecond laser delivery (lenticule creation): Incisions are made in the order: posterior cap surface → anterior cap surface → incision opening. A femtosecond laser system such as VisuMax (Zeiss) is used. Delivery time is approximately 25–40 seconds per eye. If excessive bubble accumulation (OBL) occurs during delivery, the procedure is paused until the bubbles clear.
Lenticule dissection and extraction: Using a dedicated spatula, blunt dissection is performed first on the posterior cap surface (deep plane) and then on the anterior cap surface (shallow plane). The lenticule is then grasped with forceps and pulled out through the small incision. Complete dissection of the lenticule is essential; incomplete dissection can lead to difficulty in extraction and delayed visual recovery2).
Confirmation of complete extraction: The lenticule is unfolded to confirm complete removal (partial retention can cause delayed visual recovery). The shape and thickness of the extracted lenticule are checked to ensure they match the intended parameters.
Postoperative care: The cornea is gently irrigated with saline to remove residual debris from the extraction pocket. Antibiotic eye drops (e.g., fluoroquinolones) and steroid eye drops are administered to complete the procedure.
Total surgery time for both eyes is approximately 15–30 minutes. The actual laser delivery time per eye is very short, about 25–40 seconds, resulting in minimal physical, mental, and time burden for the patient.
Antibiotic eye drops: for 1–2 weeks postoperatively (e.g., levofloxacin 0.5% or moxifloxacin 0.5%). Use 4–6 times daily.
Steroid eye drops: fluorometholone 0.1% or prednisolone eye drops, tapered over 2–4 weeks postoperatively (also for prevention/treatment of Grade I DLK)
Artificial tears/mucin secretagogues: for postoperative dry eye (diquafosol 3% 6 times daily or rebamipide 2% 4 times daily)
Preservative-free formulations: preservative-free artificial tears (e.g., Hyalein Mini) are recommended for postoperative ocular surface protection
Regular check-ups: 1 day, 1 week, 1 month, 3 months, and 6 months after surgery1)
For undercorrection or refractive regression, enhancement surgery is considered after 6 months postoperatively once refraction is stable1). Options include:
Creating a flap on the original cap surface with a femtosecond laser and additional excimer laser ablation (LASIK-like enhancement): the most common method. Residual corneal thickness must be confirmed.
Surface ablation with PRK: an option when residual stromal bed is thin. Consider using mitomycin C (MMC) to prevent postoperative haze.
SMILE re-treatment: attempted at some facilities but not standardized.
It is essential to confirm that the residual corneal thickness (sum of cap, lenticule extraction cavity, and residual stromal bed) meets the safety standard (RST ≥ 280 μm) when performing enhancement2). The incidence of undercorrection is continuously improving through nomogram optimization and AI-driven predictive models, with recent enhancement rates below 5% at many facilities.
QIs reoperation (enhancement) necessary after SMILE surgery?
A
Enhancement surgery is considered if undercorrection, overcorrection, or refractive regression occurs. The decision is usually made after 6 months postoperatively once refraction is stable. The common method is to create a flap on the original cap surface with a femtosecond laser and perform additional excimer laser ablation. Confirmation of residual corneal thickness is essential.
The femtosecond laser focuses within the corneal stroma, creating interfaces for the anterior and posterior surfaces of the lenticule through plasma formation and micro-photodisruption. The corneal stroma (lenticule) sandwiched between these two incision planes is removed, changing the corneal curvature and correcting myopia.
The shape of the lenticule (difference in curvature between the anterior and posterior surfaces) is designed according to the amount of refractive correction. Removing a convex lens-shaped stromal piece that is thicker in the center and thinner at the periphery reduces the refractive power of the cornea, correcting myopia.
The minimum lenticule thickness is usually set at 15–20 μm or more; if the lenticule is thinner than this, safe extraction may be difficult. For astigmatism correction, the accuracy of limbal marking and eye tracking systems is important to precisely position the asymmetric (axis-asymmetric) lenticule shape 6). The optical zone diameter in SMILE is typically set between 6.0 and 7.0 mm, but a larger optical zone (≥6.5 mm) has been reported to result in fewer postoperative higher-order aberrations (especially coma) and better night vision function 2). However, enlarging the optical zone increases the amount of tissue removed (→ decreased RST), so individual design balancing biomechanics and visual function is important 2).
SMILE preserves corneal biomechanical properties better than LASIK. Meta-analysis showed that the decrease in Corneal Resistance Factor (CRF) at 12 months postoperatively was significantly smaller than with FS-LASIK (MD, −1.13; 95% CI −1.36 to −0.90; P < 0.001) 2). The decrease in Corneal Hysteresis (CH) was also smaller than with FS-LASIK (MD, −1.17; 95% CI −1.45 to −0.89; P < 0.001) 2).
The reason for this advantage lies in the cap structure that preserves the anterior stroma (the site with the highest mechanical strength). The cap (anterior stroma) maintains the continuity of the lamellar structure and provides higher biomechanical strength than the LASIK flap 2).
The differences between the SMILE cap and the LASIK flap are: (1) no hinge, maintaining continuity with the cornea around the entire circumference; (2) a closed structure with only a small incision (2–3 mm) under the cap communicating with the outside; and (3) preservation of strong collagen fibers in the anterior stroma. This design means that postoperative trauma-related flap dislocation, as seen in LASIK, is usually not a concern 2). The LT index (maximum lenticule thickness/central corneal thickness ratio) management value of ≤28% is an important indicator for maintaining this biomechanical advantage; exceeding 28% is thought to negatively affect biomechanics beyond the reinforcing effect of the cap 2).
In SMILE, instruments are inserted only through a small incision (2–3 mm) near the limbus, minimizing damage to the sensory nerves (corneal nerve plexus) in the anterior stroma. In LASIK, nerves are severed around the entire circumference when creating a 360° corneal flap. Therefore, the incidence and severity of postoperative dry eye symptoms are lower with SMILE than with LASIK. Comparative studies of FS-LASIK and SMILE have also reported that corneal nerve density recovers faster and tear parameters are less affected with SMILE 4).
In vivo confocal microscopy (IVCM) time-course evaluation of corneal nerve density shows that after SMILE, the nerve plexus density recovers to about 70–80% of preoperative levels at 3 months postoperatively, whereas after LASIK, recovery is limited to about 40–60% during the same period in many cases 4). This difference is thought to correspond to the difference in severity of postoperative dry eye. Complete recovery of nerve density usually takes 6 to 12 months, and in some patients it may take more than 2 years. In patients with preoperative dry eye, nerve density recovery may be delayed, and proactive preoperative dry eye treatment may improve the postoperative course.
Postoperative corneal ectasia is primarily attributed to reduced corneal biomechanical strength due to insufficient residual stromal thickness (RST) or excessive lenticule thickness, as well as preexisting subclinical keratoconus. Analysis shows that 65.5% of ectasia cases had abnormal or suspicious corneal topography preoperatively, and 52.3% had RST < 280 μm 2).
The incidence of ectasia after SMILE is rarer than after LASIK (11 vs. 90 per 100,000 eyes) 5), but management of ectasia once it occurs is similar to that for post-LASIK ectasia. If progression is confirmed, corneal cross-linking (CXL) is the first-line treatment, and it has been covered by insurance in Japan since 2022.
Opaque bubble layer (OBL) is caused by accumulation of water vapor and carbon dioxide between layers. Maintaining room temperature at 18–25°C and humidity at 30–70%, along with appropriate laser energy settings, are preventive measures 2). If OBL is extensive and covers the pupillary area, it is recommended to wait for complete resolution before proceeding with lenticule extraction. Forcing the procedure increases the risk of wrong plane dissection.
In a 5-year comparative study by Li et al. (2019), both the SMILE and FS-LASIK groups maintained safety and efficacy, with no significant difference in long-term corneal biomechanical effects 3). The SMILE group maintained good refractive stability even after 5 years. Both procedures showed excellent uncorrected distance visual acuity (UDVA) at 5 years, and best-corrected visual acuity (BCVA) was well maintained 3).
In a systematic review by Moshirfar et al.5), the ectasia rates for PRK, LASIK, and SMILE were calculated as 20, 90, and 11 per 100,000 eyes, respectively. SMILE’s ectasia rate was shown to be approximately 1/8 that of LASIK, but it has been pointed out that the follow-up period for SMILE is still short, potentially leading to underestimation5). The same review confirmed that ectasia can also occur in eyes without any known risk factors, highlighting the need for further refinement of preoperative screening.
In a prospective multicenter SMILE study for US FDA approval (myopia with astigmatism) reported by Dishler et al.6), the mean residual spherical equivalent was −0.07D (±0.38D SD) at 12 months postoperatively, and 95.4% of eyes achieved UCVA of 20/20 or better, meeting safety and efficacy criteria. For astigmatism correction, it was also shown that cyclotorsion error correction using limbal marking is effective in improving accuracy6).
In a systematic review and meta-analysis by Song et al.7), the astigmatism correction outcomes of SMILE and LASIK were compared, showing no significant differences in correction accuracy, residual astigmatism, or visual acuity. However, in cases of high astigmatism (>2.0D), SMILE’s cyclotorsion error control was shown to affect outcomes. The use of limbal marking and eye tracking systems is recommended7).
Reinstein et al.8) compared the relative corneal tensile strength of PRK, LASIK, and SMILE using a mathematical model. SMILE was shown to preserve more corneal strength for equivalent correction amounts due to its cap structure that spares the anterior stroma compared to LASIK. This theoretical basis is argued to be consistent with SMILE’s lower ectasia rate8).
Corneal Biomechanics After SMILE: Long-Term Changes
In a 1-year follow-up study by Shetty et al.9), SMILE showed significantly smaller decreases in postoperative corneal biomechanics (CRF, CH) compared to LASIK. This difference became evident after 3 months postoperatively and was maintained at 12 months. It is suggested that the protection of the anterior stroma may be due to the biomechanical contribution of the cap9).
SMILE is considered to have a lower ectasia risk than LASIK and a risk profile similar to PRK 10). However, preoperative screening for subclinical keratoconus is also important in SMILE, and comprehensive biomechanical evaluation including CBI and TBI should be performed 10).
Definition of Progression and International Consensus
The international consensus by Gomes et al. 11) proposed a definition of ectasia progression (at least two consistent changes among anterior corneal steepening, posterior corneal steepening, and corneal thinning), and this criterion is applied to the management of ectasia after refractive surgery including SMILE.
Santhiago et al. 12) showed that percent tissue altered (PTA) ≥40% is an independent risk factor for post-LASIK ectasia. In SMILE (KLEx), since the cap contributes to corneal strength differently from the flap, there is debate about directly applying the LASIK-based PTA threshold, but management values of LT index ≤28% and RST ≥280 μm are commonly important 12).
Meta-analyses have confirmed that postoperative residual astigmatism is significantly higher and correction accuracy is lower in the high astigmatism group (>2.0D) compared to the low astigmatism group (<2.0D). Cyclotorsion error correction using limbal marking or triple centration improves accuracy 2).
Sekundo et al. 13) reported the first efficacy and safety trial (6-month outcomes) of femtosecond laser lenticule extraction (FLEx). FLEx is the precursor technology to SMILE, and this trial laid the foundation for the subsequent development of SMILE. Reducing the incision size from 7 mm in FLEx to 2–3 mm in SMILE achieved better corneal nerve protection and safety.
The TFOS DEWS III report by Jones et al. 14) states that multiple studies support that SMILE has a significantly smaller impact on postoperative dry eye symptoms and corneal nerve density compared to LASIK. For ocular surface optimization after refractive surgery, preoperative MGD treatment, diquafosol, and perioperative use of IPL are considered 14).
Reports indicate that AI-driven nomogram adjustments combining preoperative corneal biomechanical parameters improve refractive prediction accuracy by more than 25% 2). Future development of personalized nomograms using multimodal data is expected.
The ectasia risk scoring system by Randleman et al.15) is useful for preoperative prediction of post-LASIK ectasia and consists of five factors: abnormal corneal topography, low residual stromal thickness, young age, thin cornea, and high myopia. Since similar factors increase the risk of postoperative ectasia in SMILE, the concept of this scoring can be applied to preoperative screening15).
New-generation technologies such as CLEAR and SILK
In addition to SMILE, several femtosecond laser lenticule extraction technologies such as CLEAR (cornea lenticule extraction for advanced refractive correction) and SILK (smooth incision lenticule keratomileusis) have been developed, and further technical standardization is progressing2). CLEAR is a variant of SMILE that aims to improve incision design and expand application to hyperopia and presbyopia correction. SILK is developed to smooth the cut surface and suppress bubble formation, improving ease of lenticule dissection and speed of visual recovery. These new technologies inherit the flap-free and biomechanics-preserving principles established in SMILE while aiming to expand indications, improve accuracy, and reduce complications.
Research on corneal lenticule reimplantation after SMILE
Attempts are being made to reimplant lenticules extracted during SMILE as allogeneic corneal inlays in patients with hyperopia, presbyopia, or keratoconus. Although immune reactions may be minimal, this is currently at an experimental stage and has not reached general clinical application. In cases where lenticules are reused for hyperopia correction, the principle involves cryopreserving the extracted lenticule and transplanting it into an appropriate patient to alter corneal thickness and refractive power, and its potential as an alternative to banked corneas is being discussed. However, further evidence accumulation is needed regarding long-term safety and efficacy.
Wang Y, Xie L, Yao K, Sekundo W, Alió JL, Mehta JS, Goel S, Elmassry A, Schallhorn J, Shilova T, Cao H, Xu L, Chen X, Zhang F, Bai J, Zhang W, Liu Q, Zhou X, Chen Y, Wang Z, Jhanji V, Yang K, Writing Committee for the Guideline Working Group. Evidence-Based Guidelines for Keratorefractive Lenticule Extraction Surgery. Ophthalmology. 2025;132(4):397-419. doi:10.1016/j.ophtha.2024.11.016. PMID:39577672.
Li M, Li M, Chen Y, Miao H, Yang D, Ni K, et al. Five-year results of small incision lenticule extraction (SMILE) and femtosecond laser LASIK (FS-LASIK) for myopia. Acta ophthalmologica. 2019;97(3):e373-e380. doi:10.1111/aos.14017. PMID:30632671.
Recchioni A, Sisó-Fuertes I, Hartwig A, Hamid A, Shortt AJ, Morris R, et al. Short-Term Impact of FS-LASIK and SMILE on Dry Eye Metrics and Corneal Nerve Morphology. Cornea. 2020;39(7):851-857. doi:10.1097/ICO.0000000000002312. PMID:32243424.
Moshirfar M, Tukan AN, Bundogji N, Liu HY, McCabe SE, Ronquillo YC, et al. Ectasia After Corneal Refractive Surgery: A Systematic Review. Ophthalmology and therapy. 2021;10(4):753-776. doi:10.1007/s40123-021-00383-w. PMID:34417707; PMCID:PMC8589911.
Dishler JG, Slade S, Seifert S, Schallhorn SC. Small-incision lenticule extraction (SMILE) for the correction of myopia with astigmatism: outcomes of the United States Food and Drug Administration premarket approval clinical trial. Ophthalmology. 2020;127:1020-1030.
Song J, Cao H, Chen X, Zhao X, Zhang J, Wu G, et al. Small Incision Lenticule Extraction (SMILE) Versus Laser Assisted Stromal In Situ Keratomileusis (LASIK) for Astigmatism Corrections: A Systematic Review and Meta-analysis. American journal of ophthalmology. 2023;247:181-199. doi:10.1016/j.ajo.2022.11.013. PMID:36410469.
Reinstein DZ, Archer TJ, Randleman JB. Mathematical model to compare the relative tensile strength of the cornea after PRK, LASIK, and small incision lenticule extraction. J Refract Surg. 2013;29:454-460. doi:10.3928/1081597X-20130617-03. PMID:23820227.
Shetty R, Francis M, Shroff R, Pahuja N, Khamar P, Girrish M, et al. Corneal Biomechanical Changes and Tissue Remodeling After SMILE and LASIK. Investigative ophthalmology & visual science. 2017;58(13):5703-5712. doi:10.1167/iovs.17-22864. PMID:29101408.
Jhanji V, Ahmad S, Amescua G, et al. Corneal Ectasia Preferred Practice Pattern. Ophthalmology. 2024 Apr;131(4):P205-P246. doi:10.1016/j.ophtha.2023.12.038. PMID:38349299.
Gomes JA, Tan D, Rapuano CJ, Belin MW, Ambrósio R, Guell JL, Malecaze F, Nishida K, Sangwan VS, Group of Panelists for the Global Delphi Panel of Keratoconus and Ectatic Diseases. Global consensus on keratoconus and ectatic diseases. Cornea. 2015;34(4):359-369. doi:10.1097/ico.0000000000000408. PMID:25738235.
Santhiago MR, Smadja D, Gomes BF, et al. Association between the percent tissue altered and post-LASIK ectasia in eyes with normal preoperative topography. Am J Ophthalmol. 2014;158:87-95.e1. doi:10.1016/j.ajo.2014.04.002. PMID:24727263.
Sekundo W, Kunert K, Russmann C, Gille A, Bissmann W, Stobrawa G, et al. First efficacy and safety study of femtosecond lenticule extraction for the correction of myopia: six-month results. Journal of cataract and refractive surgery. 2008;34(9):1513-20. doi:10.1016/j.jcrs.2008.05.033. PMID:18721712.
Jones L, Craig JP, Markoulli M, Karpecki P, Akpek EK, Basu S, et al. TFOS DEWS III: Management and Therapy. American journal of ophthalmology. 2025;279:289-386. doi:10.1016/j.ajo.2025.05.039. PMID:40467022.
Randleman JB, Woodward M, Lynn MJ, Stulting RD. Risk assessment for ectasia after corneal refractive surgery. Ophthalmology. 2008 Jan;115(1):37-50.e4. doi:10.1016/j.ophtha.2007.03.073. PMID:17624434.
Copy the article text and paste it into your preferred AI assistant.
Article copied to clipboard
Open an AI assistant below and paste the copied text into the chat box.