Hyperopia is a refractive state of the eye in which parallel light rays entering the eye without accommodation focus behind the retina. In other words, it is a condition where the far point is at a finite distance behind the eye, meaning that light converging toward the back of the eye comes to a focus on the retina.
This condition is mainly caused by the combined refractive power of the cornea and lens being too weak relative to the axial length of the eye. Generally, hyperopia of +6D or more is called high hyperopia, and extreme hyperopia of +10D or more may fall into the category of microphthalmos.
Classification of Hyperopia (by Measurement Method)
Hyperopia is classified into the following three types based on the measurement method.
Total hyperopia = Manifest hyperopia + Latent hyperopia holds true.
Type
Definition
Total hyperopia
Hyperopic refractive error measured under complete cycloplegia with cycloplegic agents such as atropine.
Manifest hyperopia
Hyperopic refractive error detectable by routine refraction testing without cycloplegia.
Latent hyperopia
Hyperopic refractive error that is latent and not detected by routine testing, but becomes apparent only under cycloplegic examination. It is large in children.
QWhat is latent hyperopia?
A
Latent hyperopia is a hyperopic component that is compensated by accommodation during routine refraction testing and therefore not detectable, but becomes apparent only when examined with cycloplegic agents (such as cyclopentolate or atropine). Children have very strong accommodative ability, so the proportion of latent hyperopia is high. Missing latent hyperopia can lead to inadequate diagnosis and treatment of amblyopia or accommodative esotropia, so cycloplegic examination is always performed in pediatric hyperopia evaluation.
Classification Based on Accommodative Compensation
The part of manifest hyperopia that can be compensated by accommodation. The hyperopic degree that can be clearly seen with the naked eye through accommodation.
Absolute hyperopia
The part of manifest hyperopia that is not compensated by accommodation. Clear vision is not possible without corrective lenses.
Relative hyperopia
Related to eye position: hyperopia that can be clearly seen by accommodation, but which causes esotropia.
As the elasticity of the lens decreases with age, accommodative power declines, so the component that was hidden as facultative hyperopia in youth becomes apparent as eye strain and decreased vision in middle age and beyond.
Generally, newborns are hyperopic, with a distribution centered around +2D. By around 1 year of age, they become nearly emmetropic. Hyperopia tends to increase until around 7–8 years of age and then decreases. This is called emmetropization. In a study by Herrnheiser in 1892, the frequency of hyperopia decreased by around age 20, while the frequencies of emmetropia and myopia increased.
The prevalence of amblyopia is reported to be about 2–4% in children, with hyperopic anisometropic amblyopia and hyperopic binocular amblyopia accounting for a large proportion 1). The risk of amblyopia and accommodative esotropia particularly increases with hyperopia of +2D or more, and the risk of developing amblyopia becomes significantly higher at +6D or more (see table) 1).
The mean hyperopia in pure accommodative esotropia is +5.43D ± 2.25 D (in amblyopic eyes without esotropia, +6.11D ± 1.84 D), indicating that high hyperopia is a major risk factor for amblyopia and esotropia1). Even in special cases with high anisometropia (e.g., -17.50D) such as unilateral megalophthalmos associated with neurofibromatosis type 1 (NF1), severe amblyopia can result if early ophthalmology referral is not made 11).
High hyperopia (especially +2D or more) is prone to the following complications.
Hyperopic amblyopia: Risk of amblyopia increases with +2D or more. Particularly high risk with +4.5D or more (with strabismus) or +6D or more (without strabismus) 1)
Accommodative esotropia: Commonly occurs with hyperopia of +2 to +8D. More likely with +2D or more, and rare with +8D or more.
Angle-closure glaucoma: Due to shallow anterior chamber and narrow angle. Risk persists into adulthood.
It occurs when the axial length of the eye is shorter than normal.
Congenital: Newborns have a short axial length (about 17–18 mm, adults about 24 mm), resulting in physiological hyperopia. As they grow, the axial length elongates and emmetropization occurs.
In young children, due to lack of concentration to maintain proper focus on distant objects, instillation of cycloplegic eye drops is essential for objective refraction testing.
First choice: 1% cyclopentolate (Cyplegin®) eye drops
One to two instillations per day provide sufficient cycloplegia. Onset of effect is 30–60 minutes after instillation, lasting about half a day. Be aware of side effects (facial flushing, tachycardia, excitement).
Atropine eye drops (when stronger cycloplegia is needed)
Regardless of age, 1% atropine eye drops are used, instilled twice daily for 7 days. This provides the most complete cycloplegia and can detect the full amount of latent hyperopia. Since the effect lasts 1–2 weeks and mydriasis and photophobia persist, it is important to explain this to the patient.
Objective refraction under cycloplegia is essential for detecting latent hyperopia; without cycloplegia, there is a risk of significantly underestimating the degree of hyperopia.
Normal refractive values in infants and young children (under 1% cyclopentolate cycloplegia)
If the refractive error is 2D or more stronger than the normal value, consider prescribing glasses.
Also, as diagnostic criteria for amblyopia, use interocular difference ≥2 lines or binocular ≤20/50 for ages 3-4, and interocular difference ≥2 lines or binocular ≤20/40 for ages 5 and older1).
It is important to differentiate pseudoneuritis from papilledema. In high hyperopia, the optic disc margins may appear blurred, but there is no leakage on fluorescein angiography, and visual fields and acuity are usually within normal limits.
QWhy is cycloplegic medication necessary for hyperopia testing in children?
A
Children have much greater accommodative power than adults, and even with hyperopia, they unconsciously accommodate to see clearly. Therefore, a standard refraction test without cycloplegic drugs significantly underestimates the degree of hyperopia. In particular, latent hyperopia is not detected without cycloplegia. By measuring with complete cycloplegia using cyclopentolate or atropine eye drops, the true hyperopic refractive error becomes apparent. Prescribing appropriate corrective glasses based on this value leads to prevention and treatment of amblyopia and accommodative esotropia.
Asthenopia only: A +0.25D convex lens may be effective.
In a prospective study by the Pediatric Eye Disease Investigator Group (PEDI), 27% of children aged 3–6 years with anisometropic amblyopia achieved resolution of amblyopia with spectacle correction alone, with an average improvement of 0.29 logMAR 2). The current standard approach is to observe with refractive correction alone until visual acuity stabilizes after prescribing glasses 2).
First step: Full-time wear of full correction glasses
Prescribe full correction glasses based on cycloplegic refraction and have the child wear them full-time. Often, visual acuity improves to some extent with glasses alone. The current standard approach is to observe with refractive correction alone until visual acuity stabilizes after prescribing glasses 2).
If visual acuity does not improve sufficiently with glasses alone, apply an adhesive patch to the sound eye.
Moderate amblyopia (20/40 to 20/80): 2 hours of patching per day is as effective as 6 hours 5).
Severe amblyopia: 6 hours of patching per day is nearly as effective as full-time patching 6).
Third step: Atropine eye drops (penalization)
Instill 1% atropine in the sound eye to blur near vision via cycloplegia, encouraging use of the amblyopic eye. It is nearly as effective as patching for moderate amblyopia7). Useful as an alternative when patching compliance is poor.
Bangerter filters
A method of attaching a translucent filter to the spectacle lens of the sound eye. In a PEDI study, the difference in visual acuity improvement compared to patching was within 0.5 lines after 24 weeks 1).
For pure accommodative esotropia, instill 0.5% atropine three times daily for 3–5 days, and have the patient wear fully corrective glasses or glasses with a power reduced by 0.5 D. It is important to ensure that the glasses are worn continuously and that the frame does not slip down.
For partially accommodative esotropia, hyperopic glasses are similarly prescribed, but residual esotropia is treated with surgery or prism therapy.
In accommodative esotropia complicated by hyperopic amblyopia, it is necessary to concurrently perform spectacle prescription, amblyopia treatment, and strabismus correction. If strabismus surgery is performed while amblyopia remains untreated, there is a risk of binocular suppression being released postoperatively, leading to diplopia. Therefore, the principle is to prioritize or concurrently conduct amblyopia treatment 1).
In adults with accommodative esotropia (esotropia without glasses), removing glasses may cause social and occupational limitations. In such cases, refractive surgery (e.g., LASIK) may be performed to improve strabismus. However, the primary purpose of refractive surgery is refractive correction, and the surgical effect on strabismus is secondary. This must be fully explained preoperatively 15).
High hyperopia (+6D or more) in children can cause amblyopia and accommodative esotropia. It is necessary to detect the full hyperopic power early and correct it with glasses or other means. After childhood, contact lenses are also an option. Since findings such as short axial length and shallow anterior chamber persist, continuous attention to the risk of complications in adulthood (e.g., angle-closure glaucoma) is required. In cases of nanophthalmos complicated by uveal effusion syndrome, scleral window surgery is effective 3). Regular follow-up is recommended for nanophthalmos cases 3).
In adults (aged 20 or older, with stable refractive error), hyperopia can be corrected by excimer laser procedures such as LASIK (laser in situ keratomileusis) or PRK (photorefractive keratectomy). The guidelines for refractive surgery (8th edition) recommend an upper limit of approximately +6D (spherical equivalent) for hyperopic correction; for higher degrees of hyperopia, the indication should be carefully considered 4).
Hyperopic LASIK is more prone to regression compared to myopic correction, especially for high hyperopia of +4D or more, where long-term refractive stability tends to decrease 4). This is related to the specific corneal ablation pattern (peripheral ablation, central sparing), and the interaction with age-related corneal shape changes accelerates regression.
PRK does not create a corneal flap, so it may be chosen for patients with thin corneas or those with high activity levels (sports, occupation). However, postoperative subepithelial haze is more common in hyperopic correction than in myopic correction, which may affect long-term correction accuracy 4).
Hyperopia correction with phakic intraocular lenses (ICL, IPCL, etc.) is positioned as an option for cases with high hyperopia (over +6 D) that are not candidates for LASIK. Since no corneal ablation is performed, the risk of regression is low, but there are separate risks of complications such as cataract, increased intraocular pressure, and corneal endothelial cell loss 4).
QDoes children's hyperopia improve with growth?
A
Many children have physiological hyperopia (around +2 D) in infancy, and as they grow, the axial length elongates and emmetropization occurs. However, the process of emmetropization follows a course where hyperopia temporarily increases until around 7–8 years of age and then decreases. Mild hyperopia often improves naturally with growth, but in cases of high hyperopia (over +6 D) or when complicated by amblyopia or accommodative esotropia, correction may still be needed after growth. Additionally, in high hyperopia, a shallow anterior chamber persists even in adulthood, so ongoing risk management for angle-closure glaucoma is necessary.
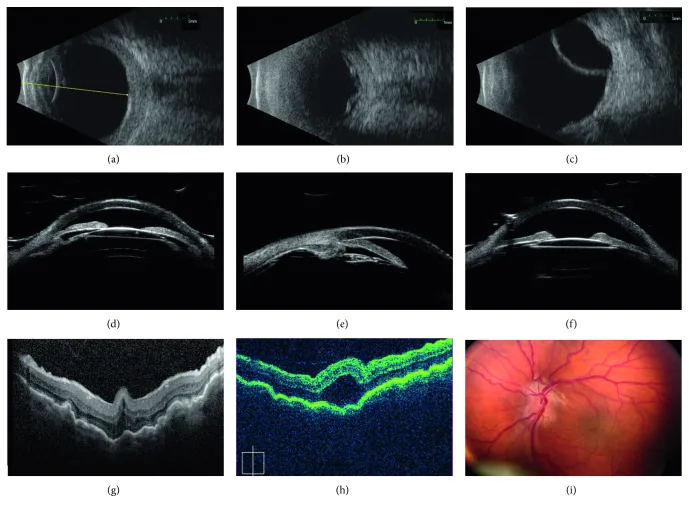
Carricondo PC, Andrade T, Prasov L, Ayres BM, Moroi SE. Nanophthalmos: A Review of the Clinical Spectrum and Genetics. J Ophthalmol. 2018;2018:2735465. Figure 1. PMCID: PMC5971257. License: CC BY.
Nine-panel composite image in nanophthalmos: (a–c) B-mode ultrasound shows short axial length, thickened sclera/choroid, serous retinal detachment and choroidal effusion; (d–f) ultrasound biomicroscopy (UBM) shows shallow anterior chamber, angle closure, and anterior rotation of the lens-iris diaphragm; (g–h) OCT shows prominent chorioretinal folds; (i) fundus photograph shows a crowded disc with blurred disc margins and vascular tortuosity. Corresponds to the anatomical features of high hyperopia (short axial length, shallow anterior chamber, pseudoneuritis) discussed in the section “Pathophysiology and Detailed Mechanisms.”
Hyperopia occurs when the combined refractive power of the cornea and lens is relatively weak relative to the axial length. In a normal eye, the combined refractive power of about 58–60 D and an axial length of about 24 mm are balanced, so that parallel light rays focus precisely on the retina. In a hyperopic eye, this balance is disrupted, and the focal point is formed behind the retina.
The lens can increase its refractive power by thickening through contraction of the ciliary muscle (accommodation), compensating for hyperopia. As long as the hyperopia is within the range of accommodation, no visual impairment occurs (facultative hyperopia). However, because accommodation must be maintained constantly, fatigue of the accommodative muscles (asthenopia) is likely to occur.
With aging, the elasticity of the lens decreases and accommodative power declines, so hyperopia that was asymptomatic in youth may manifest as asthenopia and decreased vision in middle age and beyond. The proportion of absolute hyperopia increases, and corrective glasses become necessary.
The axial length of a newborn is short (about 17–18 mm), and there is physiological hyperopia (around +2 D). With growth, the axial length elongates (to about 24 mm in adults), and the balance between refractive power and axial length is achieved, leading to emmetropization. This emmetropization process is regulated by a feedback mechanism that depends on visual input.
Around the age of 7 to 8 years, there is a temporary slight increase in hyperopic power. If refractive error evaluation is neglected during this period, amblyopia and esotropia may be missed.
Children have stronger ciliary muscle tension and greater accommodative power compared to adults. Therefore, much of hyperopia is hidden as latent hyperopia, and accurate hyperopic power cannot be measured without cycloplegia. Glasses prescribed without detecting latent hyperopia result in inadequate correction, reducing the effectiveness of amblyopia and strabismus treatment.
In high hyperopia due to axial hyperopia, the axial length is short, leading to a shallow anterior chamber. Eyes with a shallow anterior chamber tend to have narrow angles, increasing the risk of acute angle-closure glaucoma attacks. Additionally, relative crowding of the posterior pole due to short axial length can cause blurred optic disc margins (pseudoneuritis) and posterior pole retinal folds.
In nanophthalmos with high hyperopia, pathological abnormalities of the sclera may constrict the vortex veins (draining vessels of the choroidal system) at the scleral penetration site, potentially causing uveal effusion syndrome. In type I (true nanophthalmos with scleral thickening), which presents with short axial length and high hyperopia, scleral window surgery is effective when exudative retinal detachment occurs 3). Regular follow-up is recommended in nanophthalmos cases.
Eyes with high hyperopia (especially +6D or more, axial hyperopia) tend to have shallow anterior chambers and narrow angles. With aging, the lens thickens, further narrowing the angle and increasing the risk of acute angle-closure glaucoma (AACG).
The following are recommended for AACG risk management 1):
Regular assessment of anterior chamber depth and angle width (UBM, AS-OCT, etc.)
Preoperative confirmation of anterior chamber depth and preparation for emergency management when mydriasis is required
Consideration of prophylactic laser peripheral iridotomy (LPI) in adults with high hyperopia and shallow anterior chambers
Cataract surgery replaces the lens with a thinner intraocular lens, thus eliminating the angle-closure risk in high hyperopia. In very short axial length high hyperopia (+8D or more, axial length <21 mm), prophylactic lens extraction (clear lens extraction) before cataract development may be considered for angle-closure glaucoma prevention.
Excimer laser correction for hyperopia (LASIK/PRK) has been considered less stable than for myopia, with a tendency for regression (myopic shift). In recent years, improvements in corneal ablation patterns have enhanced accuracy, and good outcomes have been reported for moderate hyperopia (around +3 D).
Expansion of SMILE (small incision lenticule extraction) for hyperopia is also under research. For high hyperopia exceeding +6 D, there are still limitations, and surgical options including phakic intraocular lenses (ICL) for hyperopia may be considered 13). The KLEx (SMILE) guidelines have clarified the indications for myopia and myopic astigmatism, with LASIK remaining the mainstream for hyperopia correction 13). Attention to hyperopic eyes in IOL power calculation during cataract surgery (effects of anterior chamber depth and lens thickness) is also important, and newer formulas (e.g., Barrett Universal II) have improved accuracy for hyperopic eyes 14).
Photo screening devices have been shown to be effective for early detection of pediatric hyperopia and amblyopia, which are difficult to detect with traditional visual acuity tests 8). The introduction of photo screeners in 3-year-old health checkups is becoming more widespread, and improvements in early detection rates of amblyopia are expected. The Spot Vision Screener can measure refractive error, strabismus angle, pupil size difference, and interpupillary distance, and displays an abnormality when amblyopia risk factor thresholds are exceeded 8).
Treatment protocol for hyperopic amblyopia (stepwise management)
Treatment of hyperopic amblyopia (isoametropic/anisometropic) follows these steps 1).
Step 1 (0–18 weeks): Full correction glasses only
Prescribe full correction glasses based on cycloplegic refraction and observe with glasses alone until vision stabilizes. In PEDIG studies, spectacle correction alone improved amblyopic eye visual acuity by an average of 0.29 logMAR, and 27% no longer met amblyopia criteria 7). Skipping this step and proceeding directly to occlusion may lead to overtreatment in cases that would improve with glasses alone.
Step 2 (after 18 weeks): Add occlusion or atropine
If visual acuity plateaus at 18 weeks after glasses prescription, add occlusion or atropine. In bilateral amblyopia (isoametropic), occlusion is not possible because the amblyopic eye cannot be identified, so continuous wear of full correction glasses is the mainstay.
Stage 3 (After visual improvement): Tapering, discontinuation, and monitoring for recurrence
When visual acuity has normalized (or after confirming a plateau for 4 months), occlusion is gradually tapered. The recurrence rate of amblyopia is reported to be about 24% within one year after treatment discontinuation, making regular follow-up essential 2). In cases of recurrence, a good response to retreatment is often observed.
A study using Luminopia’s headset (72 hours of use in children) reported a visual acuity improvement of 0.15 logMAR 2). In adults with anisometropic amblyopia, an improvement of 0.15 logMAR (one line improvement per 27 hours) has been reported 2), and comparative studies with traditional occlusion therapy are ongoing. In dichoptic training under VR, 44 hours of training resulted in visual acuity improvement from 0.05 to 0.5 and acquisition of stereopsis10). The adult strabismus PPP (2023) also emphasizes the importance of refractive correction for esotropia with hyperopia, and presents a systematic management flow for surgical indications when residual strabismus persists after correction 15). Research on the appropriate timing for discontinuing occlusion therapy in preschool vision screening shows high predictability of visual acuity at age 4 (r=0.83, p<0.01), indicating that continued occlusion after age 4 may not always be effective 9). Furthermore, in untreated amblyopic children aged 7–17, spectacle correction alone improved visual acuity in 25% after 24 weeks, and additional occlusion improved it in 53% (ages 7–12), demonstrating that treatment is possible even after the sensitive period 12).
Pediatric Eye Disease Investigator Group. A randomized trial of prescribed patching regimens for treatment of severe amblyopia in children. Ophthalmology. 2003;110:2075-2087.
Pediatric Eye Disease Investigator Group. A randomized trial of atropine vs. patching for treatment of moderate amblyopia in children. Arch Ophthalmol. 2002;120:268-278.
Pediatric Eye Disease Investigator Group. Treatment of anisometropic amblyopia in children with refractive correction. Ophthalmology. 2006;113:895-903.
Kanclerz P, Przewłócka K, Arnold RW. Agreement in non-cycloplegic and cycloplegic refraction between a photoscreener and a calibrated autorefractor. BMC Ophthalmol. 2024;24(1):130. doi:10.1186/s12886-024-03375-z. PMID:38528448; PMCID:PMC10962162.
Drews-Botsch CD, Cotsonis G, Celano M, Zaidi J, Hartmann EE, Lambert SR. Is Patching after Age 4 Beneficial for Children Born with a Unilateral Congenital Cataract?. Ophthalmology. 2025;132(4):389-396. doi:10.1016/j.ophtha.2024.11.005. PMID:39522734. PMCID:PMC11930621.
Halicka J, Bittsansky M, Sivak S, et al. Virtual reality visual training in an adult patient with anisometropic amblyopia: visual and functional magnetic resonance outcomes. Vision. 2021;5(2):22.
Mukit FA, Cape HT, Huq SS, Bohn S. An Isolated Case of Unilateral Macro-Ophthalmia With Resultant Anisometropic Amblyopia in Neurofibromatosis 1. Cureus. 2023;15(9):e44679. doi:10.7759/cureus.44679. PMID:37809258; PMCID:PMC10550781.
Pediatric Eye Disease Investigator Group. Randomized trial of treatment of amblyopia in children aged 7 to 17 years. Arch Ophthalmol. 2005;123:437-447.
Wang Y, Xie L, Yao K, et al. Evidence-based guidelines for keratorefractive lenticule extraction surgery. Ophthalmology. 2025;132(4):397-419. doi:10.1016/j.ophtha.2024.11.016. PMID:39577672.