SS-OCT
Wavelength: 1310 nm (long wavelength)
Penetration depth: High (images the entire anterior segment in one frame)
Resolution: Lower than SD-OCT but sufficient for clinical use
Representative device: CASIA (Tomey Corporation)

Anterior segment optical coherence tomography (AS-OCT) is a non-contact optical coherence tomography device specialized for the anterior segment. It acquires cross-sectional images of the tear film, cornea, iris, anterior lens surface, angle, and sclera, and is used for understanding the pathology of anterior segment diseases and various biometric measurements.
AS-OCT imaging was first reported by Izatt et al. in 1994. Initially, it used the same 830 nm wavelength as retinal OCT, but its penetration into scattering tissues such as the sclera was poor, making it unsuitable for angle imaging. Subsequently, devices using a longer wavelength of 1310 nm were developed, greatly improving scleral penetration and imaging speed.
Currently, Fourier-domain OCT (FD-OCT) is mainstream, offering superior measurement speed, resolution, and three-dimensional analysis capability compared to time-domain OCT (TD-OCT). FD-OCT includes two types: swept-source OCT (SS-OCT) and spectral-domain OCT (SD-OCT).
SS-OCT
Wavelength: 1310 nm (long wavelength)
Penetration depth: High (images the entire anterior segment in one frame)
Resolution: Lower than SD-OCT but sufficient for clinical use
Representative device: CASIA (Tomey Corporation)
SD-OCT
Wavelength: 840 nm (short wavelength)
Penetration depth: Shallow (difficult to image the entire anterior segment)
Resolution: Higher than SS-OCT
Use: Suitable for detailed observation of the cornea and conjunctiva
AS-OCT is a diagnostic device that allows non-contact observation of the angle. Its resolution is superior to ultrasound biomicroscopy, but the ciliary body cannot be observed 3). Its usefulness as an auxiliary diagnostic tool in glaucoma care is widely recognized 3).
Fundus OCT is a device that acquires cross-sectional images of the retina, using a light source with a wavelength of 840–870 nm. AS-OCT is specialized for observing the anterior segment (cornea, angle, iris, etc.), and the SS-OCT method uses a long wavelength of 1310 nm to enhance penetration into deep tissues. The observation target and wavelength used are different.
AS-OCT examination is performed in a seated position. The patient looks at a fixation point while the examiner aligns the scan position and captures the image. It is non-invasive and does not require an eyecup or water immersion method. Imaging can be performed in the dark, allowing angle assessment under physiological pupillary dilation. The main features of AS-OCT are listed below.
The most important landmark for interpreting AS-OCT images is the scleral spur. The scleral spur is the junction between the inner surface of the sclera and the curvature of the cornea, visible as an inward projection of the sclera. By evaluating the apposition between the iris and the inner wall of the corneosclera, angle closure can be detected.
However, it has been reported that the scleral spur is not visible in approximately 25% of cases when using scan protocols without image averaging.
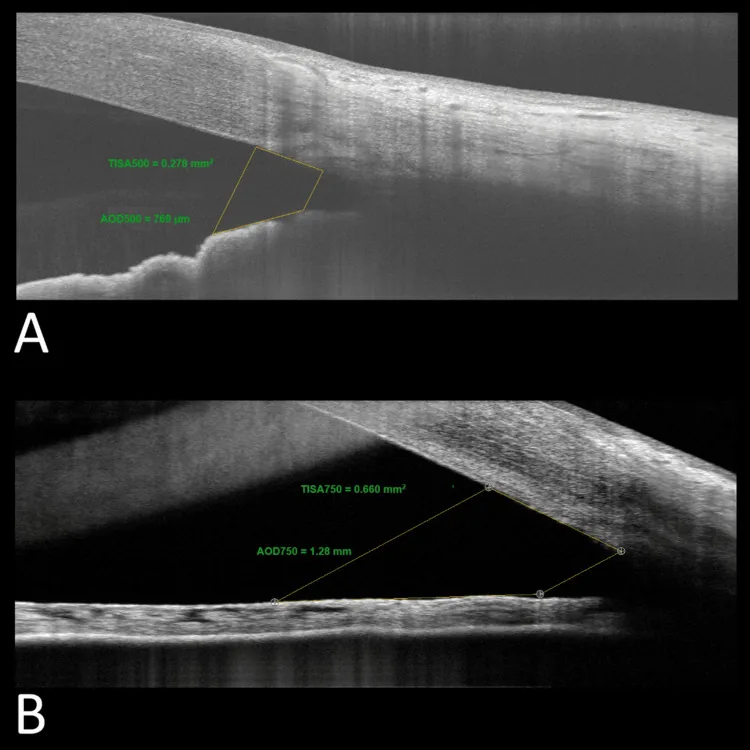
The main parameters used for quantitative measurement of the anterior chamber angle are listed below.
| Parameter | Abbreviation | Definition |
|---|---|---|
| Angle opening distance | AOD | Distance between the iris and a point 500/750 μm anterior to the scleral spur |
| Angle recess area | ARA | Area bounded by AOD, iris, and corneoscleral inner wall |
| Trabecular-iris space area | TISA | Trapezoidal area from scleral spur to AOD line |
Other parameters such as iris thickness, anterior chamber width, and lens vault have also been reported.
Ultrasound biomicroscopy (UBM) is also used for anterior segment tomographic imaging. The characteristics of both are compared.
| Item | AS-OCT | Ultrasound Biomicroscopy |
|---|---|---|
| Principle | Optical | Ultrasound |
| Resolution | 15 μm | 50 μm |
| Maximum scan range | 16 × 6 mm | 5 × 5 mm |
Gonioscopy is indispensable in glaucoma practice 3), and in Japan, the Shaffer classification and Scheie classification are commonly used to describe angle findings 3).
AS-OCT is a non-contact examination; the instrument does not touch the eye. There is no pain or discomfort. Anesthetic eye drops are not required, and the examination takes only a few minutes.
In glaucoma clinical practice, AS-OCT is useful as an adjunct to gonioscopy, or as an alternative when gonioscopy is difficult due to corneal disease or lack of patient cooperation. Because it is non-contact and can be performed in the dark, angle assessment under physiological mydriasis is possible.
Based on iris morphology and the position of the lens relative to anterior segment structures, mechanisms of angle closure such as pupillary block and anterior lens displacement can be identified 4). It has become indispensable for observing morphological changes of the iris such as shallow anterior chamber, narrow angle, and plateau iris.
It is also useful as a patient education tool when recommending laser iridotomy.
Angle imaging devices cannot replace gonioscopy 6). Gonioscopy should be performed in all patients with suspected glaucoma 6).
AS-OCT is useful for identifying iris morphology in narrow angles, assessing lens effects, and triaging eyes where gonioscopy is difficult 6). However, peripheral anterior synechiae (PAS), pigment deposition, and other secondary causes of trabecular dysfunction may be missed, so evaluation solely by angle imaging should be avoided 6).
AS-OCT is also applied in preoperative and postoperative evaluation of glaucoma surgery. It is used to assess the morphology of filtering blebs after trabeculectomy and to confirm the position of intraocular drainage devices.
Tanito et al. (2024) clearly visualized the stent condition, which was difficult to evaluate with conventional 2D cross-sectional images, using raster scanning and 3D AS-OCT imaging in cases 2 years after PreserFlo MicroShunt (PFM) implantation. In the right eye, a C-shaped deformation was confirmed, suggesting that the fin may have prolapsed from the scleral pocket 1).
This C-shaped deformation has rarely been reported in the literature and is thought to be caused by compression from surrounding scar tissue 1). Adding 3D images to 2D images significantly improved the accuracy of stent evaluation 1).
Measurement of peripapillary retinal nerve fiber layer thickness (RNFL) and macular inner retinal layer thickness using OCT can be used to assess structural progression in glaucoma 3). Each OCT device is equipped with a program to detect changes over time.
However, imaging conditions (e.g., measurement position shift, image quality) affect the measured values, so caution is needed not to take the values at face value 3). In advanced glaucoma eyes, a floor effect occurs where further thinning becomes difficult to detect, making OCT progression assessment more suitable for relatively early cases 3).
Glaucoma diagnosis should not be based solely on OCT, as results indicating “outside normal limits” may be false positives 6). Comprehensive judgment integrating clinical findings and visual field testing is essential 6).
Computer-aided diagnostic devices, including OCT, are used for detecting glaucoma and identifying progressive optic neuropathy 5). With advances in device technology (e.g., high-resolution SD-OCT), improvements in diagnostic performance are expected 5).
No, it cannot. AS-OCT has the advantage of non-contact imaging in dark conditions, but findings such as peripheral anterior synechiae, pigmentation, and neovascularization in the angle may be difficult to detect with AS-OCT 6). Gonioscopy should be performed in all patients suspected of having glaucoma 6).
Huang et al. (2024) conducted a bibliometric analysis of 20 years (2004–2023) of literature on AS-OCT applications in glaucoma, analyzing 931 reports. The United States had the most publications with 288, followed by China with 231, and Singapore with 124. By author, Aung Tin had the most publications (80) and citations (3595) 2).
The number of papers has increased rapidly since 2012, and since 2015, more than 60 papers have been published stably each year2). Since 2018, advances in artificial intelligence (AI) have led to a notable shift from manual measurement to automated detection and recognition in research2).
A recent research frontier is the automated detection of angle closure using deep learning2). Conventional AS-OCT image evaluation relies on manual measurement of various parameters, which is time-consuming, subjective, and has low reproducibility.
Deep learning algorithms learn directly from image data and demonstrate the ability to classify open, narrow, and closed angles with high accuracy. A 3D deep learning-based digital gonioscopy system (DGS) has shown diagnostic accuracy comparable to ophthalmologists in detecting narrow iridocorneal angles and peripheral anterior synechiae2).
FD-mode AS-OCT operating at a wavelength of 1310 nm is enabling rapid three-dimensional cube scanning of the anterior segment. This is expected to allow the following evaluations:
3D AS-OCT has also demonstrated utility in postoperative evaluation of glaucoma surgical devices, clearly visualizing the overall shape of stent deformation or displacement, which is difficult with 2D images1).
Optical coherence tomography angiography (OCTA) is a rapidly developing technology. It is considered less susceptible to floor effects than retinal nerve fiber layer measurements and may be advantageous over OCT for progression assessment in advanced glaucoma eyes, but standardized clinical application methods have not been established3).
It is still at the research stage. Although automated detection of angle closure using deep learning algorithms has shown high accuracy2), it has not yet been widely implemented in clinical practice. Challenges such as insufficient data and lack of unified diagnostic criteria remain.