Advantages of Trabeculectomy

Non-Penetrating Deep Sclerectomy (Deep Sclerectomy / NPDS)
1. What is Non-Penetrating Deep Sclerectomy (NPDS)?
Section titled “1. What is Non-Penetrating Deep Sclerectomy (NPDS)?”Non-penetrating deep sclerectomy (NPDS) is a glaucoma surgery reported by Kozlov and Fyodorov in 1989 1). After resecting the deep scleral flap and removing the outer wall (roof) of Schlemm’s canal, the juxtacanalicular trabecular meshwork is dissected to promote aqueous filtration through the trabeculo-Descemet membrane (TDM) 1)2).
The greatest feature of NPDS is that it does not penetrate the anterior chamber 1). The juxtacanalicular trabecular meshwork is the site of greatest resistance to aqueous outflow; removing it increases aqueous outflow and lowers intraocular pressure. By avoiding sudden decompression of the anterior chamber, the risk of serious complications associated with penetrating surgery, such as hypotony, choroidal detachment, and anterior chamber flattening, is reduced 1)4).
The history of non-penetrating filtration surgery dates back to sinusotomy by Kasnov and Walker in 1964. Over the following decades, refinements led to the establishment of NPDS. In Europe, it is widely used as a major option for glaucoma surgery, but due to its technical difficulty and long learning curve, it is less frequently performed in the United States 1).
Advantages of NPDS
Reduction of hypotony complications: Lower risk of hypotony and choroidal detachment1)
Suppression of cataract progression: Tendency for lower cataract formation rate than trabeculectomy1)
Reduced postoperative management: Less burden of bleb management1)
Q
What is the difference between NPDS and trabeculectomy?
A
NPDS is a procedure that filters aqueous humor through the TDM without penetrating the anterior chamber, while trabeculectomy drains aqueous humor by full-thickness penetration of the anterior chamber. NPDS has fewer serious postoperative complications such as hypotony and choroidal detachment, but its long-term intraocular pressure-lowering effect tends to be slightly inferior to trabeculectomy. Meta-analyses have reported that the intraocular pressure-lowering effects of both procedures are equivalent, but trabeculectomy tends to require fewer postoperative medications.
3. Indications and Contraindications
Section titled “3. Indications and Contraindications”NPDS is indicated for primary and secondary open-angle glaucoma1)2). The main candidates are cases where intraocular pressure cannot be controlled with maximum tolerated medical therapy or laser treatment. Its usefulness has also been reported for congenital glaucoma4).
In uveitic glaucoma, NPDS may be advantageous because postoperative inflammation is reduced compared to penetrating surgery. Eyes with long axial length are at high risk of hypotony after penetrating filtration surgery, so NPDS should be considered.
| Category | Target Disease |
|---|---|
| Indications | Primary and secondary open-angle glaucoma |
| Absolute contraindications | Angle-closure glaucoma, neovascular glaucoma |
| Relative contraindication | Narrow angle, traumatic glaucoma |
Angle-closure glaucoma and neovascular glaucoma are absolute contraindications because aqueous outflow via TDM cannot be expected. In narrow-angle glaucoma, surgery may be possible if the angle is opened by combined lens reconstruction.
4. Surgical technique
Section titled “4. Surgical technique”Conjunctival incision and antimetabolites
Section titled “Conjunctival incision and antimetabolites”Conjunctival incision is performed using a limbal-based or fornix-based approach. There is no difference in intraocular pressure reduction between the two methods. To reduce the risk of fibrosis, antimetabolites (MMC or 5-FU) are applied as widely and posteriorly as possible 2).
Creation of superficial scleral flap
Section titled “Creation of superficial scleral flap”The superficial scleral flap is created in a triangular, rectangular, or trapezoidal shape. Thickness is 1/3 to 1/2 of the sclera, and length is 3 to 5 mm. This flap serves as the roof of the decompression chamber 2).
Deep scleral flap and Schlemm’s canal opening
Section titled “Deep scleral flap and Schlemm’s canal opening”Dissection begins posteriorly at a deep layer near the suprachoroidal space, advancing anteriorly to identify the scleral spur and Schlemm’s canal 2). The roof of Schlemm’s canal is removed, and the cribriform trabeculum and inner wall of Schlemm’s canal are gently dissected with capsulorhexis forceps. In this step, it is important to avoid pressure on the globe and prevent TDM perforation.
Performing anterior chamber paracentesis before deep flap dissection reduces trabecular bulging and lowers the risk of perforation. If perforation occurs, it is managed with microiridectomy.
Implant placement
Section titled “Implant placement”To maintain the scleral space (intrascleral lake) postoperatively, a space-maintaining device may be used 2).
Non-absorbable implants
T-flux®: A highly hydrophilic acrylic implant made of poly-Megma®. The T-shaped arm is inserted into the Schlemm’s canal opening.
Esnoper®: A new implant made of non-absorbable acrylic polymer.
Absorbable implants and others
Aquaflow®: A cylindrical collagen implant. After placement, it absorbs water and triples in volume, then degrades over 6–9 months.
SK-gel®: Made of cross-linked hyaluronic acid. Healon GV (viscoelastic substance) is also used for space maintenance.
CO2 laser-assisted sclerectomy (CLASS)
Section titled “CO2 laser-assisted sclerectomy (CLASS)”The CO2 laser scanning system (IOPtiMate) is effective for vaporizing dry tissue, allowing precise treatment of Schlemm’s canal and the TDM window while controlling thinning of the scleral tissue. Infrared CO2 laser is absorbed and blocked by aqueous humor, providing a self-regulating mechanism to prevent intraocular perforation. Compared to conventional NPDS, the learning curve is shorter and the surgical time is shorter.
Goniopuncture
Section titled “Goniopuncture”After NPDS, aqueous outflow resistance through the TDM may increase over time, leading to elevated intraocular pressure 5). In such cases, goniopuncture with Nd:YAG laser (LGP) creates a full-thickness hole in the TDM to reduce outflow resistance.
| Parameter | Setting |
|---|---|
| Laser | Nd:YAG (Q-switched) |
| Initial energy | 2 mJ |
| Endpoint | Appearance of microfiltering bleb |
Preoperatively, 2% pilocarpine and local anesthesia are administered, and the anterior edge of the TDM is irradiated while observing the angle with a contact lens. LGP within 3 months postoperatively is not recommended due to the risk of hypotony or iris incarceration. The most frequent complication after LGP is iris prolapse/incarceration (up to 17.6%).
The morphology of the filtering bleb after goniopuncture may be affected by conjunctivochalasis 5). In eyes with conjunctivochalasis, the sudden increase in aqueous outflow due to LGP may utilize the lax conjunctiva as a low-resistance pathway, leading to abnormal inferior bleb extension. This phenomenon often resolves spontaneously, but it is important to check for conjunctivochalasis preoperatively and reflect it in postoperative management 5).
Q
What is goniopuncture?
A
Goniopuncture is an Nd:YAG laser procedure performed when intraocular pressure rises due to thickening of the TDM after NPDS. Under gonioscopy, a full-thickness hole is made in the TDM to reduce outflow resistance of aqueous humor into the subconjunctival space. Irradiation is performed with an initial energy of about 2 mJ, and the appearance of a microfiltering bleb is the endpoint. Performing it within 3 months postoperatively is not recommended due to the risk of hypotony. The most common complication is iris incarceration (up to 17.6%).
5. Treatment Outcomes and Complications
Section titled “5. Treatment Outcomes and Complications”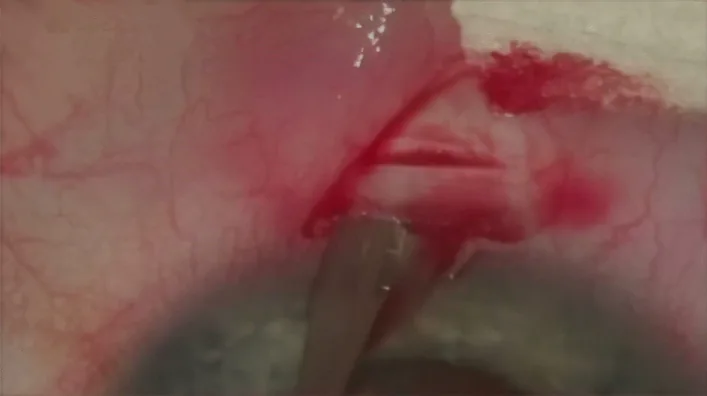
Rękas M, Konopińska J, Byszewska A, et al. Mini-canaloplasty as a modified technique for the surgical treatment of open-angle glaucoma. Sci Rep. 2020;10(1):12801. Figure 1. PMID: 32733032; PMCID: PMC7393495; DOI: 10.1038/s41598-020-69261-y. License: CC BY.
Intraoperative image showing the conjunctiva opened and a superficial scleral flap being created. This is a representative photograph illustrating the basic steps of deep sclerectomy.
Treatment Outcomes
Section titled “Treatment Outcomes”Several meta-analyses comparing NPDS and trabeculectomy have been reported 1)3). Long-term intraocular pressure reduction tends to be superior with trabeculectomy, but some RCTs have reported equivalent efficacy between the two procedures 2). The number of postoperative intraocular pressure-lowering medications tends to be higher with NPDS 1).
On the other hand, NPDS has significantly fewer hypotony-related complications and a lower rate of cataract progression 1). Reduced burden of postoperative management is also a clinical advantage.
Complications
Section titled “Complications”NPDS generally has a good safety profile, but there are specific complications 1)4).
The most common intraoperative complications are inability to identify Schlemm’s canal and TDM perforation. TDM perforation has been reported in up to 30% of cases, and large perforations can lead to iris incarceration, requiring conversion to trabeculectomy 7).
As postoperative complications, hypotony is common early on, but often does not require treatment if not accompanied by shallow anterior chamber or maculopathy. Descemet’s membrane detachment can occur weeks to months after surgery.
A rare complication has been reported in a 16-year-old male who developed a 160-degree giant retinal tear two weeks after NPDS for congenital glaucoma 4). This patient had buphthalmos and myopia, and early vitreous liquefaction due to myopia was considered a risk factor for retinal tear 4). It was managed with vitrectomy and silicone oil tamponade.
In a case where NPDS was performed on an eye after DSAEK, perforation during TDM manipulation led to complete dislocation of the endothelial graft, but spontaneous reattachment was observed after four weeks 6). Large-diameter grafts may obstruct the angle structures and hinder the success of NPDS 6).
Q
What are the complications of NPDS?
A
Intraoperative complications include TDM perforation (up to 30%) and inability to identify Schlemm’s canal most commonly; large perforations require conversion to trabeculectomy. Early postoperative hypotony is frequent but usually resolves spontaneously. Rare complications such as giant retinal tear and Descemet’s membrane detachment have been reported. Iris incarceration after goniopuncture (up to 17.6%) also requires attention. Compared to trabeculectomy, serious complications such as hypotony maculopathy, choroidal detachment, and bleb infection are significantly less common.
7. Latest Research and Future Perspectives
Section titled “7. Latest Research and Future Perspectives”XEN-DS (XEN-Augmented Deep Sclerectomy)
Section titled “XEN-DS (XEN-Augmented Deep Sclerectomy)”XEN-DS (XEN-augmented deep sclerectomy), which combines a XEN gel stent with NPDS, has been reported as a new surgical technique 7). A superficial scleral flap is created 2 mm posterior to conventional NPDS, and the XEN gel stent is inserted into the anterior chamber from the anterior wall of the deep sclerectomy 7).
In a 96-year-old patient with pseudoexfoliation glaucoma who underwent XEN-DS, postoperative intraocular pressure was stable at 5–8 mmHg for six months, and the visual field MD improved from -9.6 dB to -1.5 dB 7). There were no perioperative or postoperative complications, and no additional interventions such as needling were required 7).
XEN-DS is a surgical technique that combines the advantages of NPDS (intrascleral outflow via the scleral lake) and the standardized aqueous humor control and favorable bleb morphology of the XEN stent 7). It may eliminate the need for goniopuncture, making it suitable for patients with difficulty in follow-up visits. Clinical studies are currently underway to evaluate its long-term efficacy and safety 7).
Conjunctivochalasis and Its Impact on Bleb Morphology
Section titled “Conjunctivochalasis and Its Impact on Bleb Morphology”Cases have been reported where inferior bleb extension occurred after goniopuncture in eyes with conjunctivochalasis 5). Conjunctivochalasis is increasingly recognized as an anatomical factor affecting postoperative aqueous humor dynamics, suggesting the importance of evaluating conjunctival status in preoperative planning for bleb-forming surgeries 5).
8. References
Section titled “8. References”European Glaucoma Society. European Glaucoma Society Terminology and Guidelines for Glaucoma, 6th Edition. Br J Ophthalmol. 2025;109(Suppl 1):1-212. PMID:41026937. doi:10.1136/bjophthalmol-2025-egsguidelines.
2. Gedde SJ, Vinod K, Wright MM, et al. Primary Open-Angle Glaucoma Preferred Practice Pattern. Ophthalmology. 2021 Jan;128(1):P71-P150. doi:10.1016/j.ophtha.2020.10.022. PMID:34933745. 3. 日本緑内障学会緑内障診療ガイドライン改訂委員会. 緑内障診療ガイドライン(第5版). 日眼会誌. 2022;126(2):85-177. 4. Felemban MN, Alshehri M, Aljahdali FF, Rubio M, Schargel K. Uncommon Complication Post-deep Sclerectomy: Giant Retinal Tear. Cureus. 2024;16(2):e53854. doi:10.7759/cureus.53854. PMID:38465193; PMCID:PMC10924656. 5. Abdulrahman Alhazmi, Fahad Alharthi, Jumanah Qedair. Inferior extension of a filtering bleb following laser goniopuncture in a patient with conjunctivochalasis. American Journal of Ophthalmology Case Reports. 2026;41:102526. doi:10.1016/j.ajoc.2026.102526. 6. Salam A. Deep sclerectomy after DSAEK: A cautionary tale. BMJ case reports. 2021;14(6). doi:10.1136/bcr-2020-237541. PMID:34130970; PMCID:PMC8208012. 7. Niegowski LJ, Gillmann K, Baumgartner JM. XEN-Augmented Deep Sclerectomy: Step-by-step Description of a Novel Surgical Technique for the Management of Open-angle Glaucoma. Journal of current glaucoma practice. 2021;15(3):144-148. doi:10.5005/jp-journals-10078-1311. PMID:35173397; PMCID:PMC8807939.