Nd:YAG laser goniopuncture is an essential component of non-penetrating glaucoma surgery (NPGS). NPGS includes deep sclerectomy, canaloplasty, and viscocanalostomy 1)2).
Intraocular pressure control after NPGS depends on aqueous filtration through the trabeculo-Descemet’s membrane (TDM). When this TDM thickens due to incomplete intraoperative dissection or postoperative fibrosis, aqueous outflow resistance increases and intraocular pressure rises.
Goniopuncture creates microperforations in the TDM, restoring direct aqueous outflow from the anterior chamber to the intrascleral space. This converts a failed non-penetrating filtration into a penetrating type, but because it is performed at a safe time after bleb formation, the risk of hypotony-related complications is significantly reduced.
Compared to trabeculectomy, NPGS has fewer hypotony-related complications but inferior long-term intraocular pressure reduction 1)2). Goniopuncture is an important adjunctive procedure that improves the success rate of NPGS.
QCan goniopuncture be performed after trabeculectomy?
A
Goniopuncture is a procedure specific to non-penetrating glaucoma surgery (NPGS) and is not indicated after trabeculectomy. In NPGS, the trabeculo-Descemet’s membrane remains intact, and laser perforation restores aqueous outflow. In trabeculectomy, a full-thickness perforation has already been created, so goniopuncture is not applicable.
In addition to topical anesthesia, instill 1% apraclonidine and pilocarpine. Miosis induced by pilocarpine reduces the risk of iris incarceration. If intraocular pressure is high, combine with a systemic carbonic anhydrase inhibitor.
Apply a gonioscopy contact lens and align the aiming beam of the Nd:YAG laser with the translucent TDM. Use the following parameters in free-running Q-switched mode.
Spot size: 3–10 μm
Power: 5–15 mJ
Number of shots: 4–15
The irradiation site should be anterior (toward the cornea) to minimize the risk of iris prolapse or peripheral anterior synechiae formation. To reduce the risk of iris incarceration after laser, argon laser iridoplasty may be performed near the TDM window.
Administer steroid eye drops (1% prednisolone acetate) three times daily for 3 days. Continue glaucoma medications until the follow-up visit. Re-examine after 1–3 weeks to check intraocular pressure and complications.
If intraocular pressure is high, pretreat with apraclonidine or systemic CAI
Create the perforation site on the corneal side
Never perform ocular massage
If iris incarceration occurs, attempt conservative management with miotics; if ineffective, consider laser or surgical synechialysis.
QWhat is the success rate of goniopuncture?
A
It has been reported that a single goniopuncture achieves at least a 20% reduction in intraocular pressure compared to before treatment for at least 2 years in about 50% of cases. It is positioned as an essential procedure for improving the success rate of NPGS and is the first-line laser treatment for intraocular pressure elevation after NPGS.
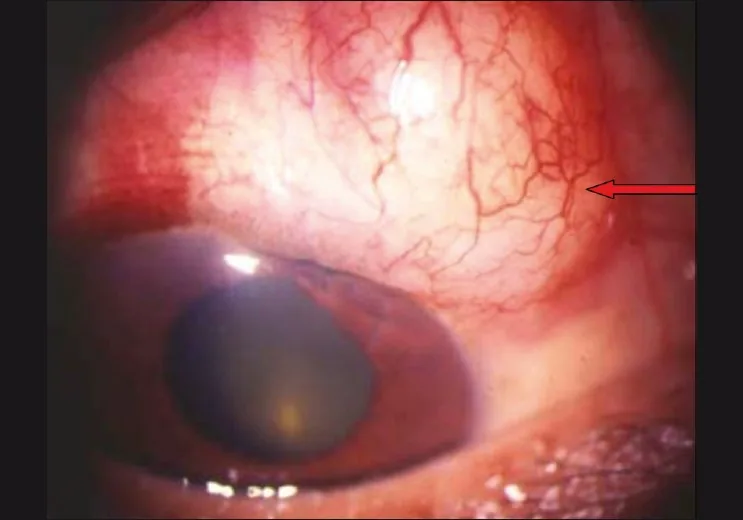
Lingam Vijaya; Panday Manish; George Ronnie; et al. Management of complications in glaucoma surgery. Indian J Ophthalmol. 2011 Jan;59(Suppl 1):S131-S140. Figure 2. PMCID: PMC3038515. License: CC BY.
Postoperative photograph showing an encapsulated filtering bleb with a thick, vascularized wall. A localized elevated subconjunctival bleb and surrounding vascular proliferation indicate insufficient outflow due to encapsulation.
Pazos M, Traverso CE, Viswanathan A; European Glaucoma Society. European Glaucoma Society - Terminology and guidelines for glaucoma, 6th Edition. Br J Ophthalmol. 2025;109(Suppl 1):1-212. doi:10.1136/bjophthalmol-2025-egsguidelines. PMID:41026937.
European Glaucoma Society. European Glaucoma Society Terminology and Guidelines for Glaucoma, 5th Edition. Br J Ophthalmol. 2021 Jun;105(Suppl 1):1-169. doi:10.1136/bjophthalmol-2021-egsguidelines. PMID:34675001.
Krasnov MM. Q-switched laser goniopuncture. Arch Ophthalmol. 1974;92(1):37-41. PMID: 4857748.
Copy the article text and paste it into your preferred AI assistant.
Article copied to clipboard
Open an AI assistant below and paste the copied text into the chat box.