Hyphema is the accumulation of red blood cells in the anterior chamber (the space between the cornea and the iris). A small amount of bleeding only visible under slit-lamp microscopy is called microhyphema.
The most common cause is blunt trauma. Blunt force causes a sudden increase in anterior chamber pressure, stretching the limbus. The aqueous humor moves posteriorly and into the angle, damaging the iris and ciliary body, leading to bleeding.
It is classified according to the amount of bleeding as follows:
Grade
Degree of Bleeding
0
Microhyphema
I
Less than 1/3 of the anterior chamber
II
1/3 to 1/2 of the anterior chamber
III
1/2 to less than total filling of the anterior chamber
IV
Total hyphema
Among grade IV, the state where the anterior chamber is completely filled with bright red blood is called total hyphema. The state filled with dark red to black blood is called 8-ball hyphema (black ball hyphema), suggesting impaired aqueous humor circulation and hypoxia.
QCan hyphema occur without trauma?
A
Besides trauma, hyphema can occur spontaneously due to intraocular surgery, iris neovascularization, ocular tumors, blood disorders (e.g., leukemia, hemophilia), use of anticoagulants, etc. For details, see the “Causes and Risk Factors” section.
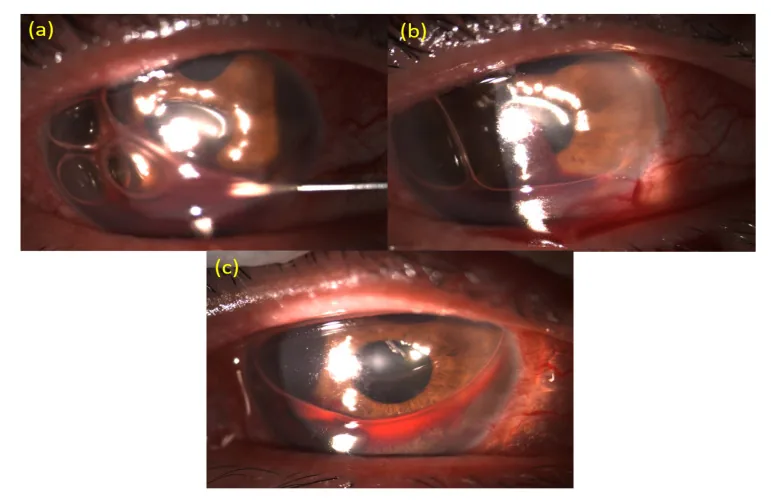
Lin IH, et al. A Novel Procedure for the Management of Severe Hyphema after Glaucoma Filtering Surgery: Air-Blood Exchange under a Slit-Lamp Biomicroscopy. Medicina (Kaunas). 2021. Figure 2. PMCID: PMC8400149. License: CC BY.
Slit-lamp photograph showing hyphema with blood pooling in the lower anterior chamber. Also shown is the procedure of inserting a needle into the anterior chamber and removing blood, illustrating the main clinical findings and treatment scene.
Hyphema forms a layer inferiorly (layering), and its color changes from red to black over time. Clotted blood appears darker. It is important to record the height from the inferior corneal limbus in millimeters.
Mild (Grade I–II)
Risk of increased intraocular pressure: Approximately 13.5%.
Visual impairment: Remains mild if the pupillary area is clear.
Fundus visibility: Often possible.
Severe (Grade III–IV)
Risk of increased intraocular pressure: Dramatically increases to 27% in Grade III and 52% in Grade IV.
Eight-ball hyphema: High risk of pupillary block and secondary angle closure.
Fundus view: Often not possible; ultrasound examination is necessary.
The main complications are as follows:
Elevated intraocular pressure: Caused by trabecular meshwork obstruction by red blood cells.
Blunt trauma is the most common cause. Compression force to the eye disrupts blood vessels in the iris, ciliary body, and trabecular meshwork, leading to accumulation of red blood cells in the anterior chamber.
After intraocular surgery: Can occur with any ophthalmic surgery, including cataract surgery. In patients taking warfarin, bleeding events during cataract surgery increase about 3-fold compared to non-users (overall incidence 9–10%), but most are self-limited hyphema or subconjunctival hemorrhage5).
After ICL (implantable collamer lens) surgery: The haptics of the ICL may form an iridociliary cyst, which can rupture and cause hyphema or posterior chamber hemorrhage6). This can occur even without a history of trauma or eye rubbing. UBM identification of the cyst is useful for diagnosis, and conservative treatment often leads to resolution; urgent ICL removal is not always necessary.
Sickle cell disease is a particularly important risk factor. In the hypoxic environment of the anterior chamber, red blood cells sickle and become rigid, making it difficult for them to pass through the trabecular meshwork. As a result, even a small amount of bleeding can cause a severe increase in intraocular pressure. Furthermore, sickled red blood cells within blood vessels can cause central retinal artery occlusion and ischemic optic neuropathy. Even sickle cell trait poses a risk.
QCan cataract surgery be performed while taking anticoagulants?
A
Cataract surgery while continuing warfarin increases bleeding events, but most are self-limited hyphema or subconjunctival hemorrhage, with no adverse effects on postoperative visual acuity5). However, for individual risks, collaboration between the primary care physician and ophthalmologist is important.
The diagnosis of hyphema involves the following stepwise examinations.
Slit-lamp examination: Confirms blood accumulation in the anterior chamber, recording the height, color, and grade of bleeding. Large hyphemas can also be seen with a penlight.
Visual acuity test: Assesses the degree of vision loss.
Pupillary light reflex test: If bleeding is extensive, also check the consensual reflex of the fellow eye.
Seidel test: Uses fluorescein staining to check for corneal perforation.
Gonioscopy: Essential for evaluating angle recession and peripheral anterior synechiae. However, due to high risk of rebleeding, it should be avoided for 1–2 weeks after injury 4).
Imaging (CT/MRI): Performed when severe conjunctival edema, hypotony, or subconjunctival hemorrhage suggests globe rupture. MRI is contraindicated if a metallic foreign body is suspected.
Sickle cell screening: Consider screening in all patients of African descent.
The basic treatment is to rest and wait for natural absorption.
Position: Avoid lying on your back; sit or elevate the head of the bed 30–45 degrees. This allows blood to settle in the lower anterior chamber, preventing central visual obstruction and limiting exposure to the corneal endothelium and trabecular meshwork.
Hospitalization criteria: Children, hyphema with a level exceeding 1/3 to 1/2 of the anterior chamber, patients unable to follow instructions, and those with sickle cell disease accompanied by elevated intraocular pressure should be hospitalized.
Avoid strenuous activity: Rest to prevent rebleeding.
Standard prescription examples in Japan are as follows.
Atropine ophthalmic solution (1%): Once daily (at bedtime). Dilates the pupil and relaxes the ciliary muscle to reduce inflammation and stress on the angle.
Rinderon ophthalmic solution (0.1%): Four times daily. For anti-inflammatory purposes.
Adona tablets (30 mg): 3 tablets divided into 3 doses after each meal. Hemostatic agent.
For elevated intraocular pressure, add the following:
Anterior chamber washout: Perform anterior chamber irrigation using a Simcoe needle through a corneal side port. If the blood clot is large or hardened, remove it with forceps or use a vitreous cutter for excision and aspiration.
Timing of surgery: Around day 4 after injury is suitable for anterior chamber washout. At this time, the risk of rebleeding is reduced, and the blood clot is partially separated from ocular tissues.
Indications for surgery:
Healthy individuals: IOP ≥50 mmHg persisting for 5 days, or ≥35 mmHg persisting for 7 days.
Patients with sickle cell disease: IOP ≥25 mmHg persisting for more than 24 hours.
In children, when total hyphema causes visual deprivation posing a risk of amblyopia.
Glaucoma surgery: If high intraocular pressure persists after anterior chamber washout, filtration surgery may be indicated. Lens extraction is necessary if there is lens dislocation or damage. Consider laser iridotomy for pupillary block.
QIs hospitalization necessary for hyphema?
A
In many cases, outpatient management is possible with close follow-up. However, hospitalization is recommended for children, cases with a large amount of bleeding (more than 1/3 to 1/2 of the anterior chamber), cases with elevated intraocular pressure in sickle cell disease, and cases where the patient cannot follow instructions for rest.
When blunt force is applied to the eye, intraocular pressure rises rapidly. The corneal limbus stretches, and aqueous humor moves posteriorly and into the angle. This mechanical change damages the blood vessels of the iris and ciliary body, causing bleeding into the anterior chamber. Shearing forces on the damaged tissue are the main mechanism of vascular disruption.
Rebleeding occurs 3 to 7 days after injury when the initial clot contracts and dissolves 4). The incidence is reported to be 5-10% 4). Rebleeding is often more severe and in larger amounts than the initial bleed. More than 50% of rebleeding cases show elevated intraocular pressure.
Risk factors for rebleeding are as follows:
Low intraocular pressure or elevated intraocular pressure
Bleeding occupying more than 50% of the anterior chamber
Elevated intraocular pressure associated with hyphema occurs through multiple mechanisms.
Trabecular meshwork obstruction by red blood cells: Large numbers of normal red blood cells physically obstruct the trabecular meshwork.
Hemolytic glaucoma: Macrophages containing hemoglobin obstruct the trabecular meshwork. It is characterized by a reddish-brown discoloration of the trabecular meshwork4).
Ghost cell glaucoma: Degenerated red blood cells (ghost cells) appear 1–4 weeks after vitreous hemorrhage4). Red blood cells with Heinz bodies and loss of deformability obstruct the trabecular meshwork. Khaki-colored vesicles are seen in the anterior chamber. Ghost cell glaucoma rarely occurs from hyphema alone.
When severe hyphema is accompanied by sustained high intraocular pressure, the posterior cornea becomes stained with blood. This may leave visual impairment even after the hyphema resolves, requiring early anterior chamber washout.
This is an important chronic complication after blunt trauma. A tear occurs between the circular and longitudinal ciliary muscles, causing recession of the angle. In cases with angle recession of 180 degrees or more, glaucoma develops at a high rate of 6–20% over 10 years. Since onset often occurs several years or more after injury, long-term follow-up of intraocular pressure is essential.
QHow often does rebleeding occur?
A
The overall incidence of rebleeding is 5–10%, and it often occurs 3–7 days after injury 4). Rebleeding tends to be more severe than the initial bleeding, so it is important to maintain rest and undergo close observation during this period.
7. Latest research and future perspectives (reports under investigation)
With the widespread use of molecular targeted drugs, drug-related spontaneous hyphema has been reported.
Aldecoa et al. (2023) reported spontaneous hyphema in a 60-year-old woman taking ibrutinib (BTK inhibitor) 420 mg/day for 4 months for chronic lymphocytic leukemia 1). The hyphema completely resolved within 2 weeks after discontinuation of ibrutinib and topical steroid eye drops. Ibrutinib is suggested to reduce platelet adhesion to von Willebrand factor and inhibit collagen-induced platelet aggregation.
Chiang et al. (2022) reported spontaneous hyphema in a 37-year-old man with acute myeloid leukemia and severe COVID-19 pneumonia 2). It was presumed that severe thrombocytopenia (6×10⁹/L) and increased episcleral venous pressure due to prolonged prone positioning contributed.
Ison et al. (2022) reported spontaneous hyphema from iris microhemangiomas (Cobb’s tufts) in a 56-year-old woman with Eisenmenger syndrome 3). Chronic hypoxemia (resting SpO₂ 78%) and secondary polycythemia (Hb 22.5 g/dL) were thought to induce dilation of iris stromal vessels and contribute to microhemangioma formation. The hemorrhage resolved with topical atropine and dexamethasone.
Zhang et al. (Pictures & Perspectives) reported spontaneous hyphema and posterior chamber hemorrhage after ICL (implantable collamer lens) surgery 6). A 23-year-old woman presented with sudden vision loss without trauma, eye rubbing, or anticoagulant use. UBM examination revealed rupture of an iris-ciliary body cyst associated with the ICL haptics and surrounding hemorrhage. The hemorrhage resolved with conservative treatment using tobramycin-dexamethasone eye drops (4 times daily) and 1% atropine sulfate gel (twice daily) for 17 days. It was shown that emergency ICL removal is not always necessary.
Aldecoa KAT, Macaraeg CSL, Dadlani A, Yadlapalli S. Spontaneous hyphema during ibrutinib treatment in a CLL patient. Case Rep Hematol. 2023;2023:1691996.
Chiang J, Chan L, Stallworth JY, Chan MF. Spontaneous hyphema in the setting of COVID-19 pneumonia. American journal of ophthalmology case reports. 2022;26:101447. doi:10.1016/j.ajoc.2022.101447. PMID:35224286; PMCID:PMC8855609.
Ison M, Dorman A, Imrie F. Spontaneous hyphema from iris microhemangioma in Eisenmenger syndrome. American journal of ophthalmology case reports. 2022;26:101536. doi:10.1016/j.ajoc.2022.101536. PMID:35496761; PMCID:PMC9046946.
European Glaucoma Society. European Glaucoma Society Terminology and Guidelines for Glaucoma, 5th Edition. Br J Ophthalmol. 2021 Jun;105(Suppl 1):1-169. doi:10.1136/bjophthalmol-2021-egsguidelines. PMID:34675001.
American Academy of Ophthalmology Preferred Practice Pattern Cataract and Anterior Segment Committee. Cataract in the Adult Eye Preferred Practice Pattern. Ophthalmology. 2022;129(1):P52-P110.
Zhang W, Li F, Zhou J. Anterior Segment Hemorrhage after Implantable Collamer Lens Surgery. Ophthalmology. 2025;132(4):e72. doi:10.1016/j.ophtha.2024.06.015. PMID:39046379.
Copy the article text and paste it into your preferred AI assistant.
Article copied to clipboard
Open an AI assistant below and paste the copied text into the chat box.