Subconjunctival hemorrhage (SCH, hyposphagma) is a condition in which bleeding from conjunctival blood vessels accumulates in the subconjunctival space (between the bulbar conjunctiva and Tenon’s capsule). Causes include inflammation such as acute hemorrhagic conjunctivitis, external stressors like trauma or surgery, increased venous pressure due to coughing or vomiting, anticoagulant therapy such as warfarin, coagulation abnormalities, vascular abnormalities, and vascular fragility due to hypertension or diabetes. Because the bulbar conjunctiva is loosely attached to the subconjunctival tissue and sclera, even a small amount of bleeding is clearly visible to the naked eye.
Historically called “hyposphagma” (from Greek meaning “covered with blood”), case reports have accumulated in Western medicine since the 1800s. The standardized Japanese medical term corresponds to “subconjunctival hemorrhage,” while laypeople may refer to it as “bleeding in the white of the eye.” The condition occurs when blood vessels in the subconjunctival space — located between the superficial conjunctiva and Tenon’s capsule — rupture, often appearing as a well-demarcated, flat area of hemorrhage. In severe cases, it may elevate into a bullous hemorrhage, making eyelid closure difficult.
It accounts for approximately 3% of all ophthalmic outpatient visits and is found in 2.9% of patients whose chief complaint is hyperemia. Among individuals aged 65 years or older, the prevalence rises to 10.1%10). A large cross-sectional study by Mimura et al. involving 8,726 Japanese patients with hyperemia confirmed similar rates10), and no significant differences by age or sex have been reported. A review by Tarlan et al. estimated that 30–50% of cases are idiopathic, 10–30% are related to hypertension, 10–20% to trauma, and 5–15% to anticoagulant use12). Idiopathic cases are the most common, accounting for 30% to half of all cases, followed by hypertension, trauma, and anticoagulants as frequent causes. During epidemics of acute hemorrhagic conjunctivitis, this infection becomes a leading cause.
Most cases resolve spontaneously within 1 to 4 weeks without sequelae. During absorption, the hemorrhage gradually changes color from red to purple, then blue-green, and finally yellow. There is no effect on vision. However, recurrent or persistent cases warrant investigation for systemic disease, neoplasms, or coagulation disorders.
QIs subconjunctival hemorrhage a dangerous condition?
A
An isolated subconjunctival hemorrhage is benign and does not affect vision. It typically resolves spontaneously within 1 to 4 weeks. However, if it recurs or fails to resolve over a prolonged period, there may be an underlying serious systemic condition such as hypertension, diabetes, coagulation disorder, or tumor. There have been reports of Kaposi sarcoma discovered masquerading as subconjunctival hemorrhage1).
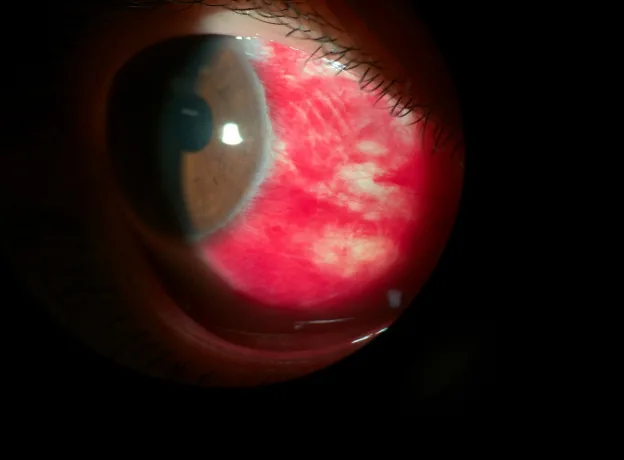
Lau AZ, Tang GY, Morgan WH, Chan GZ. Drainage of subconjunctival hemorrhage through conjunctival lymphatic pathways. American journal of ophthalmology case reports. 2025;39:102368. doi:10.1016/j.ajoc.2025.102368. PMID:40686767; PMCID:PMC12272577. Fig. 2. PMCID: PMC12272577. License: CC BY.
A set of three slit-lamp photographs showing the course of subconjunctival hemorrhage on postoperative day 1 (A), day 2 (B), and 2 weeks later (C). White arrows indicate the bleeding site, and green arrows indicate blood-filled lymphatic structures. This corresponds to the natural absorption and color changes of hemorrhage discussed in the section “2. Main Symptoms and Clinical Findings.”
Hemorrhagic patch: A bright red or dark red hemorrhagic patch is seen under the bulbar conjunctiva. It ranges from localized punctate or blotchy spots to diffuse spread across the entire bulbar conjunctiva. It changes color to pink, orange, and yellow during the absorption process.
Location of bleeding: More common in the inferior conjunctiva than the superior conjunctiva. In trauma and diabetes, it is more common on the temporal side than the nasal side.
Bullous elevation: In severe cases, the conjunctiva swells in a bullous manner, making eyelid closure difficult. There are reports of 360-degree bullous subconjunctival hemorrhage occurring after intravitreal injection in a patient with severe hemophilia A, leading to inability to close the eyelid2).
Danger signs: When accompanied by hyperemia, discharge, conjunctival laceration, hyphema, or iritis, further investigation of the underlying condition such as trauma, contusion, or infectious conjunctivitis is necessary. Conjunctival lacerations hidden by bleeding are easy to miss, so careful slit-lamp examination is required.
Differential diagnosis from acute hemorrhagic conjunctivitis: In acute hemorrhagic conjunctivitis (AHC) caused by enterovirus 70 (EV70) and coxsackievirus A24 variant (CA24v), subconjunctival hemorrhage appears in 70–90% of all AHC cases, presenting abruptly with bilateral involvement, follicular conjunctivitis, and preauricular lymphadenopathy9). The incubation period is extremely short at approximately one day, and even unilateral cases often become bilateral the following day. Hemorrhages range from patchy or petechial to extensive, taking on a spread-out appearance 3–5 days after onset. Repeated outbreaks have been reported in Japan, including the EV70 epidemic in Okinawa in 1994 and the CA24v epidemic in Okinawa in 20119). Epidemic history, contact history, and the presence or absence of bilateral involvement are important for diagnosis.
Bleeding occurs between Tenon’s capsule and the conjunctiva due to damage to conjunctival blood vessels. In older adults, the elastic and connective tissues between Tenon’s capsule and the conjunctiva are fragile, making bleeding more likely to spread.
Risk Factor
Mechanism
Idiopathic (approximately 40%)
Unknown cause
Trauma
Direct damage to conjunctival blood vessels
Systemic hypertension
Main cause in people aged 50 and over
Diabetes mellitus
Fragility due to microvascular damage8)
Warfarin
SCH incidence 3.7% in users, 1.7% in non-users7)
DOAC (Direct Oral Anticoagulant)
Apixaban, rivaroxaban, edoxaban, dabigatran, etc. Self-discontinuation is common because INR monitoring is not required.
Antiplatelet drugs
Delayed hemostasis due to aspirin, clopidogrel, etc.
Valsalva maneuver
Vascular rupture due to increased venous pressure from coughing, vomiting, constipation, weightlifting, etc.
Idiopathic subconjunctival hemorrhage accounts for 30–50% of all cases and occurs without a clear trigger. Age-related fragility of conjunctival vessels is thought to be involved12). In young patients, mild Valsalva maneuvers (lifting heavy objects, sneezing, straining during constipation, unconscious coughing during sleep) may be hidden triggers.
Traumatic subconjunctival hemorrhage results from direct ocular contusion, foreign bodies, contact lens manipulation, or eye rubbing. In children, accidental contact during tag or ball games is a common cause. In traumatic cases, always check for hyphema, iris dialysis, lens subluxation, commotio retinae, and globe rupture. Particularly, 360-degree subconjunctival hemorrhage, marked hypotony, or vision loss strongly suggests occult globe rupture, warranting orbital CT and exploratory surgery.
Hypertension-related subconjunctival hemorrhage is the most common known cause in patients aged 50 and older. Mimura et al. reported a significantly higher prevalence of hypertension in recurrent cases10). With the widespread use of home blood pressure monitoring, untreated hypertension is increasingly discovered following subconjunctival hemorrhage.
Anticoagulant and antiplatelet-related subconjunctival hemorrhage has an incidence of 3.7% with warfarin (vs. 1.7% in non-users)7), and a similar risk is estimated with the recent widespread use of DOACs. As treatment for atrial fibrillation and venous thrombosis increases in elderly patients, this remains an important cause.
Traumatic asphyxia: Sudden compression of the chest and abdomen causes blood to flow backward from the right atrium through the valveless innominate vein and jugular vein, producing petechiae and subconjunctival hemorrhage in the head and neck. This is known as “masque ecchymotique.” It is very rare in children, but a case has been reported of bilateral subconjunctival hemorrhage and facial edema after a tractor rollover accident6).
Tumors: Kaposi sarcoma masquerading as subconjunctival hemorrhage has been reported. A 34-year-old man with undiagnosed HIV presented with 3 months of spontaneous left eye redness, and Kaposi sarcoma was found in the inferior temporal fornix1). Recurrent subconjunctival hemorrhage can be the initial symptom of tumors such as cavernous hemangioma and lymphoma.
Systemic lupus erythematosus (SLE): Cases have been reported in which SLE and antiphospholipid antibody syndrome were diagnosed following subconjunctival hemorrhage. The patient presented with hypertension (140/110 mmHg), abdominal vein distention, and malar rash, and was diagnosed with inferior vena cava thrombosis and Budd-Chiari syndrome3).
Ocular vicarious menstruation: A very rare cause of subconjunctival hemorrhage that recurs monthly with menstruation. The mechanism is thought to be congestion and secondary bleeding of blood vessels with extrauterine estrogen and progesterone receptors. Oral contraceptives (levonorgestrel/ethinyl estradiol) markedly improve recurrence5).
Hemophilia: Severe subconjunctival hemorrhage has been reported after intravitreal anti-VEGF injection in patients with severe hemophilia A (factor VIII < 1%). Hemostasis was achieved with intravenous factor VIII administration, and subsequent preventive factor VIII administration before injections resulted in no recurrence2).
QWhat should I do if subconjunctival hemorrhage occurs while taking anticoagulants?
A
If subconjunctival hemorrhage occurs while taking warfarin, a blood test should be performed to check whether the INR (international normalized ratio) exceeds the therapeutic range. A meta-analysis of cataract surgery found that the warfarin continuation group had approximately three times more bleeding events than the non-use group, but most were self-limiting subconjunctival hemorrhages that did not affect postoperative vision7). Do not stop anticoagulant medication on your own; consult your primary care physician.
History taking: Assess for trauma, anticoagulant use, Valsalva maneuvers (coughing, vomiting, constipation, weightlifting), and association with menstruation.
Slit-lamp examination: Evaluate the extent, depth, and color of the subconjunctival hemorrhage. Carefully observe for the presence of conjunctival lacerations. Conjunctival lacerations hidden beneath the hemorrhage can easily be missed.
360-degree subconjunctival hemorrhage: May be a sign of occult globe rupture. Consider orbital CT and ocular exploration because zone II and III injuries cannot be ruled out.
Systemic Examination
Blood pressure measurement: Essential for screening of hypertension.
Blood tests: Check INR, PT, APTT, and platelet count in recurrent cases and patients on anticoagulants.
Systemic evaluation: In frequently recurring cases, add screening for coagulation abnormalities, autoimmune diseases, and malignancies3).
Liver and kidney function: Assess coagulation factor production and drug metabolism
Autoimmune screening: Antinuclear antibody, antiphospholipid antibody (to rule out SLE and antiphospholipid syndrome)3)
HIV antibody: To rule out conjunctival Kaposi sarcoma1)
Imaging: Orbital CT and MRI (when trauma or tumor is suspected)
Internal medicine consultation: Screening for hypertension, diabetes, and liver cirrhosis
In frequently recurring cases or cases that do not resolve for a prolonged period, poor control of systemic disease or blood/vascular abnormalities should be considered, and further internal medicine evaluation should be added.
Subconjunctival hemorrhage is a self-limiting condition that resolves spontaneously within 1 to 4 weeks. If an underlying cause is identified, treatment should be directed at the primary condition. The subconjunctival hemorrhage itself is left to follow its natural course.
No eye drops with insurance coverage exist for subconjunctival hemorrhage itself. For discomfort caused by tear film disruption, supportive therapy with frequent instillation of artificial tears is performed. When ocular surface diseases such as dry eye, punctate keratopathy, or conjunctivochalasis are present, dry eye medications (diquafosol sodium 3% ophthalmic solution, rebamipide 2% suspension ophthalmic solution, sodium hyaluronate ophthalmic solution, etc.) are prescribed based on each specific diagnosis.
For recurrent subconjunctival hemorrhage, capillary strengthening agents such as carbazochrome sodium sulfonate (Adona® tablets 30 mg, 3 times daily) may be used. However, the level of evidence is not high, and its use is limited to empirical treatment of idiopathic recurrent cases.
In patients with hemophilia A, severe subconjunctival hemorrhage can occur after intravitreal injection. There are reports that prophylactic administration of factor VIII (intravenous administration 4 hours before injection) can prevent bleeding complications2). Close collaboration with a hematologist is important.
In patients taking warfarin who experience recurrent subconjunctival hemorrhage, a blood test should be performed to confirm that the INR (international normalized ratio) does not exceed the therapeutic range (typically 2.0–3.0). Discontinuing anticoagulants without medical advice is strictly prohibited as it carries a risk of cerebral infarction or cardioembolism; any dosage adjustment must be made in consultation with the prescribing physician. In patients taking DOACs, regular INR monitoring is unnecessary, but overdose detection tends to be delayed; therefore, strict dose adjustment according to renal function is essential.
There is no direct surgical indication for subconjunctival hemorrhage itself. When conjunctivochalasis is suspected and bleeding recurs repeatedly, conjunctivochalasis surgery (conjunctival resection) can reduce recurrence. The procedure involves crescent-shaped excision of the loose redundant conjunctiva in the inferior bulbar conjunctiva, followed by reattachment or spontaneous adhesion to Tenon’s capsule and the scleral surface. Cautery excision using a high-frequency radio-knife or thermoblade is also used.
QIs there a way to make subconjunctival hemorrhage heal faster?
A
At present, there is no established treatment that promotes absorption of subconjunctival hemorrhage. It usually resolves spontaneously within 1 to 4 weeks. During the absorption process, the color changes to pink, orange, or yellow, which is a normal course. There are anecdotal reports that warm compresses may promote absorption, but the evidence is limited.
Damage to conjunctival blood vessels causes bleeding between Tenon’s capsule and the conjunctiva. In younger individuals, bleeding rarely spreads across the entire conjunctiva, but in older adults, the elastic and connective tissues between Tenon’s capsule and the conjunctiva are fragile, making extensive spread more likely.
Blunt trauma to the chest and abdomen generates positive pressure within the mediastinum. This positive pressure causes blood to flow backward from the right atrium into the valveless brachiocephalic veins and jugular veins, resulting in a sudden pressure increase in the venous bed of the head and neck. This leads to the development of petechiae 6). The absence of petechiae in the lower body is thought to be because the valves of the lower extremity veins control the pressure increase 6).
The involvement of conjunctival lymphatic vessels in the absorption of subconjunctival hemorrhage has been reported. In a case of SCH that occurred after subconjunctival anesthesia during cataract surgery, intraoperative OCT revealed a sac-like blood-filled structure adjacent to the bleeding site. It was identified as a lymphatic vessel because it had a valve-like structure 4). Marked resolution of the SCH was observed from postoperative day 1 to day 2, suggesting that lymphatic vessels may facilitate blood clearance from the subconjunctival space 4).
In type 2 diabetes, dilation, heterogeneous distribution, increased tortuosity, and changes in blood flow velocity have been reported in conjunctival microvessels 8). These microvascular abnormalities increase the fragility of conjunctival blood vessels and raise the risk of subconjunctival hemorrhage. It is reported that the longer the duration of diabetes and the higher the HbA1c level, the higher the frequency of recurrent subconjunctival hemorrhage.
Systemic hypertension is the main cause of subconjunctival hemorrhage in people over 50 years old. Chronic blood pressure elevation causes intimal thickening and medial degeneration of arterioles, leading to reduced elasticity of conjunctival vessels. Sudden blood pressure fluctuations (coughing, straining, weightlifting, acute stress) cause fragile blood vessels to rupture. It has been suggested that some cases classified as idiopathic may include undiagnosed borderline hypertension.
Pathological Mechanism of Acute Hemorrhagic Conjunctivitis
Enterovirus 70 and Coxsackievirus A24 variant (CA24v) are single-stranded positive-sense RNA viruses belonging to the Picornaviridae family and have no envelope9). Infection of conjunctival epithelial cells releases local inflammatory cytokines, increasing conjunctival capillary permeability and causing petechial and patchy hemorrhages. After the third day of illness, viral RNA detection by RT-PCR becomes difficult, so specimen collection for diagnosis should be performed early in the course of the disease9).
QHow is subconjunctival hemorrhage absorbed?
A
It was previously thought that blood in the subconjunctival space was naturally broken down and absorbed. Recent studies have suggested that conjunctival lymphatic vessels may be involved in blood drainage4). Blood has been observed inside lymphatic vessels with valve-like structures on intraoperative OCT, and it has been reported that lymphatic vessels contribute to macromolecular clearance from the subconjunctival space.
The drainage mechanism of subconjunctival hemorrhage via conjunctival lymphatics was first demonstrated using intraoperative OCT4). This finding may also be applied to predicting the prognosis of blebs in glaucomafiltration surgery. It has been hypothesized that healthy conjunctival lymphatics may help drain aqueous humor and inflammatory mediators, potentially improving filtration surgery outcomes4).
Anticoagulant and Antiplatelet Therapy in Ophthalmic Procedures
With the widespread use of direct oral anticoagulants (DOACs), evaluating the safety of ophthalmic surgery and intravitreal injections under continued anticoagulation, including warfarin, has become a challenge. According to the AAO Preferred Practice Pattern, based on meta-analysis results of cataract surgery, it is recommended in principle to perform surgery without discontinuing anticoagulants or antiplatelet agents7). Most hemorrhagic complications are limited to spontaneously resolving subconjunctival hemorrhages and rarely cause significant vision loss7).
In Japan, molecular epidemiological analysis using RT-PCR for acute hemorrhagic conjunctivitis has been established since 1996, enabling phylogenetic analysis of viral strains and tracking of epidemic patterns9,11). The 2025 edition of the Clinical Practice Guidelines for Viral Conjunctivitis states that although rapid diagnostic kits for EV70 and CA24v have not been developed, genotyping is possible through testing requests to research institutions9).
It has been suggested that the anti-adhesive effect and local fibrinolytic stimulation of anti-VEGF drugs may influence bleeding risk, but systemic anti-VEGF concentrations after intravitreal injection are extremely low, and the impact in clinical practice remains unclear2). Further accumulation of data on the safety of ophthalmic procedures in patients with coagulation disorders is needed.
Redzuwan NS, Ahmad Tarmizi NA, Mohd Khialdin S. From Simple to Sinister: Kaposi Sarcoma Masquerading as a Subconjunctival Hemorrhage. Cureus. 2023;15(9):e45296. doi:10.7759/cureus.45296. PMID:37846262; PMCID:PMC10576943.
Kesav N, Mehra AA, Schmaier AH, Sobol W. Severe Subconjunctival Hemorrhage After Intravitreal Injection in a Patient With Hemophilia A. J VitreoRetinal Dis. 2023;7(4):333-336. doi:10.1177/24741264231159218.
Sharma M, Viswanath S, Singh R. Eyes are a window to the body: A journey from subconjunctival hemorrhage to SLE and inferior vena cava stenting. Indian J Ophthalmol. 2024;72:1390. doi:10.4103/ijo.ijo_486_24.
Lau AZ, Tang GY, Morgan WH, Chan GZ. Drainage of subconjunctival hemorrhage through conjunctival lymphatic pathways. American journal of ophthalmology case reports. 2025;39:102368. doi:10.1016/j.ajoc.2025.102368. PMID:40686767; PMCID:PMC12272577.
Celebi ARC, Aygun EG. A rare cause of recurrent subconjunctival hemorrhage: ocular vicarious menstruation. GMS ophthalmology cases. 2023;13:Doc05. doi:10.3205/oc000213. PMID:36875630; PMCID:PMC9979076.
Çik N, Başerdem O, Duman M, Yilmaz D. Traumatic asphyxia with a “masque ecchymotique” in a 14-year-old adolescent. Ulus Travma Acil Cerrahi Derg. 2023;29(4):543-545. doi:10.14744/tjtes.2022.53099. PMID:36995196; PMCID:PMC10214897.
Miller KM, Oetting TA, Tweeten JP, Carter K, Lee BS, Lin S, et al. Cataract in the Adult Eye Preferred Practice Pattern. Ophthalmology. 2022;129(1):P1-P126. doi:10.1016/j.ophtha.2021.10.006. PMID:34780842.
Bron AJ, de Paiva CS, Chauhan SK, Bonini S, Gabison EE, Jain S, et al. TFOS DEWS II pathophysiology report. The ocular surface. 2017;15(3):438-510. doi:10.1016/j.jtos.2017.05.011. PMID:28736340.
Mimura T, Usui T, Yamagami S, Funatsu H, Noma H, Honda N, et al. Recent causes of subconjunctival hemorrhage. Ophthalmologica. Journal international d’ophtalmologie. International journal of ophthalmology. Zeitschrift fur Augenheilkunde. 2010;224(3):133-7. doi:10.1159/000236038. PMID:19738393.
Uchio E, Yamazaki K, Aoki K, Ohno S. Detection of enterovirus 70 by polymerase chain reaction in acute hemorrhagic conjunctivitis. American journal of ophthalmology. 1996;122(2):273-5. doi:10.1016/s0002-9394(14)72026-4. PMID:8694103.
Tarlan B, Kiratli H. Subconjunctival hemorrhage: risk factors and potential indicators. Clinical ophthalmology (Auckland, N.Z.). 2013;7:1163-70. doi:10.2147/OPTH.S35062. PMID:23843690; PMCID:PMC3702240.
Copy the article text and paste it into your preferred AI assistant.
Article copied to clipboard
Open an AI assistant below and paste the copied text into the chat box.