Conjunctivochalasis is a condition in which the bulbar conjunctiva loses its tension and forms folds. It commonly occurs in middle-aged and elderly individuals and causes various nonspecific ocular complaints. Its frequency increases with age, and it is present to some degree in almost all individuals aged 70 years or older. It is usually bilateral and commonly occurs in the inferotemporal conjunctiva.
A report from Kyoto Prefectural University of Medicine on Japanese dry eye patients indicates a prevalence of 54% 1). A large-scale hospital-based observational study in Japan also showed that the degree of laxity increases linearly with age 2).
A finding similar to conjunctivochalasis is lid-parallel conjunctival folds (LIPCOF). LIPCOF are regular, fine folds parallel to the lower eyelid margin, and their cross-sectional area is smaller than that of conjunctivochalasis. In contrast, conjunctivochalasis presents with more extensive and irregular folds, and management differs, so differentiation between the two is important 3).
Although many cases are asymptomatic, in middle-aged and elderly patients with vague complaints, it is necessary to always check for the presence of this condition.
QDoes conjunctivochalasis require treatment?
A
Conjunctivochalasis does not require treatment if asymptomatic. However, if symptoms such as foreign body sensation, tearing, or dryness are present, eye drops are used first, and if there is no improvement, surgery is considered. Because conjunctivochalasis presents symptoms similar to dry eye, it is often overlooked. In middle-aged and elderly patients with vague complaints, it is important to check for conjunctivochalasis.
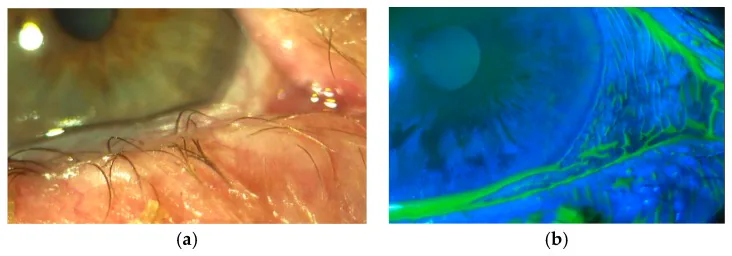
Georgios Dalianis, Alexandra Trivli, Chryssa Terzidou The Location of Conjunctivochalasis and Its Clinical Correlation with the Severity of Dry Eye Symptoms 2018 Jan 22 Medicines (Basel). 2018 Jan 22; 5(1):12 Figure 2. PMCID: PMC5874577. License: CC BY.
In image A, redundant folds of the inferior bulbar conjunctiva ride over the corneal limbus, and in image B, fluorescein staining shows disruption of the tear meniscus and contact sites. This indicates mechanical friction and tear abnormalities seen in conjunctivochalasis.
When the lax conjunctiva occupies the lower tear meniscus, an ectopic meniscus forms on top of it, reducing the stability of the adjacent tear film. Additionally, during blinking, the lax conjunctiva contacts the cornea and eyelid margin, increasing friction. If the lax conjunctiva is on the nasal side, tear flow to the punctum is suppressed, which can cause intermittent tearing.
Unlike typical dry eye, where symptoms worsen in the latter half of the day, conjunctivochalasis is characterized by strong ocular discomfort upon waking. Symptoms worsen with downward gaze, and blurring, burning, and dryness increase during reading.
A complication is idiopathic subconjunctival hemorrhage, which occurs due to the mechanism of increased friction. In cases of lax conjunctiva on the temporal side, lateral skin laxity may coexist, leading to dermatitis of the lateral canthus.
Patients with nasal conjunctivochalasis have more severe dry eye symptoms, and decreased Schirmer test values and increased meibomian gland dropout have been reported4,9).
Slit-lamp examination reveals redundant conjunctiva extending beyond the lower eyelid margin. The degree varies, from only at the 5 and 7 o’clock positions to severe cases with folds undulating at the 6 o’clock position.
Fluorescein staining clearly shows an ectopic tear meniscus on the lax conjunctiva. The tear film is thinned adjacent to the lax conjunctiva, making epithelial damage more likely.
In moderate to severe conjunctivochalasis, dry eye symptoms are significantly increased, and tear film breakup time (TBUT) is significantly decreased3). A community-based cohort study has shown that patients’ quality of life (QOL) is significantly correlated with severity and tear abnormalities11).
The etiology of conjunctivochalasis is not fully understood. Histopathologically, the collagen and elastic fibers that make up the subepithelial matrix of the conjunctiva become sparse, and elastic fibers show fragmentation. These findings suggest that degeneration of the conjunctival matrix is involved in the pathogenesis. There are two main hypotheses for the mechanism.
Aging/Mechanical Theory
Claim: Age-related changes in the conjunctiva are superimposed by mechanical effects such as eye movement, blinking, and Bell’s phenomenon.
Evidence: Histological matrix degeneration corresponds to a linear increase in incidence with age.
Inflammatory Theory
Claim: Increased production of matrix metalloproteinases (MMPs) by subconjunctival fibroblasts promotes matrix degradation.
Evidence: There are findings of an imbalance between MMPs and their inhibitors (TIMPs).
Clinically, conjunctivochalasis does not always involve inflammation; rather, the mechanical action of loose conjunctiva is thought to often secondarily cause nonspecific inflammation.
Reported risk factors for conjunctivochalasis include aging, female sex, contact lens wear, dry eye, hyperopia, pinguecula, ultraviolet exposure, and eyelid disorders4).
A large observational study from the University of Tokyo (600 contact lens wearers and 579 non-wearers) found that the frequency and severity of conjunctivochalasis were significantly higher in wearers, especially in rigid gas permeable (RGP) lens wearers2). This is thought to be because the rigidity of RGP lenses enhances chronic irritation to the conjunctiva3).
Conjunctivochalasis is also closely associated with meibomian gland dysfunction (MGD) and meibomian gland dropout. Two hypotheses coexist: one that lipid layer deficiency reduces lubrication, increasing friction and causing traction on conjunctival tissue, and the other that conjunctivochalasis reduces blink integrity, secondarily leading to meibomian gland dropout4).
Diagnosis is generally made with slit-lamp microscopy. The extent and degree of redundant conjunctiva extending beyond the lower eyelid margin are observed. In early stages, loose conjunctiva may appear only intermittently, and the forced blink test (having the patient blink forcefully to bring out the redundant conjunctiva) is useful.
Fluorescein staining makes the diagnosis of conjunctivochalasis easier. After staining, the state of the loose conjunctiva occupying the inferior tear meniscus is observed, and the movement of the loose conjunctiva and its contact with the cornea are checked with a strong blink. On the nasal side, differentiation from disruption of the tear meniscus by the plica semilunaris is necessary.
Anterior segment optical coherence tomography (AS-OCT) is useful for quantitative assessment of tear meniscus height (TMH), and can objectively evaluate the reduction of the tear meniscus due to conjunctivochalasis 4).
In conjunctivochalasis presenting with epiphora, perform lacrimal irrigation before surgery to confirm that there is no obstruction in the lacrimal drainage system. Even a slight obstruction will not improve epiphora after conjunctivochalasis surgery. Conjunctivochalasis is one of the conditions easily overlooked in the differential diagnosis of epiphora in Japanese outpatient practice.
Normal structure, easily mistaken for tear meniscus disruption
QHow is conjunctivochalasis different from dry eye?
A
Conjunctivochalasis and dry eye often have overlapping symptoms and frequently coexist. Dry eye is primarily caused by abnormalities in tear quality or quantity, and symptoms typically worsen in the latter part of the day. In contrast, conjunctivochalasis tends to cause stronger symptoms upon waking because excess conjunctiva physically obstructs the tear meniscus. Fluorescein staining to check for loose conjunctiva is useful for differentiation.
Asymptomatic conjunctivochalasis does not require treatment 3,5). For symptomatic cases, first perform eye drop treatment for about one month, and consider surgery if the effect is insufficient.
Because symptoms of conjunctivochalasis can be exacerbated by nonspecific inflammation due to tear film instability and increased friction, first treat with a combination of preservative-free artificial tears, mucosal epithelial repair agents, and low-potency steroids for about one month.
Artificial tears / Tear secretion promotion
Preservative-free artificial tears: 7 times a day
Diquafosol sodium (3%): 6 times a day. Useful for cases with decreased tear secretion
Mucosal epithelial repair
Rebamipide (2%): 4 times a day
Expected to be effective for foreign body sensation
Anti-inflammatory
Fluorometholone (0.1%): twice daily
As a low-potency steroid, used in combination with any of the above
The actual prescription is recommended to be a combination of “artificial tears, mucosal epithelial repair agents, or tear secretion stimulants” plus a “low-potency steroid” for one month. When using steroids, monitor for increased intraocular pressure.
Clinical evidence for eye drop treatment reports that three-month administration of artificial tears containing isotonic glycerol and 0.015% sodium hyaluronate significantly reduced conjunctivochalasis grade from 3 to 2 or lower, and improved OSDI, TBUT, and corneal staining 3,10). On the other hand, combination of 0.5% ketorolac and 0.15% sodium hyaluronate improved OSDI but did not produce a significant change in conjunctivochalasis grade itself 3).
Surgery is considered when there are chronic symptoms that do not improve with eye drop treatment (especially foreign body sensation, intermittent epiphora, and recurrent spontaneous subconjunctival hemorrhage). Multiple surgical techniques are used, including resection, suturing, cauterization, and high-frequency radiofrequency electrosurgery (HFR-ES), chosen based on the degree of laxity and whether glaucoma is present5,6,13). In Japan, lacrimal meniscus reconstruction (3-block resection method) is widely performed, which involves resecting subconjunctival fibrous tissue including Tenon’s capsule to obtain adhesion with the sclera.
This method most strongly promotes adhesion between the conjunctiva and sclera, and is the only method that can address all variations of conjunctivochalasis. The procedure is as follows:
Divide the lax area of the inferior conjunctiva into three blocks, and excise the subconjunctival fibrous tissue including Tenon’s capsule
Perform conjunctival resection according to the degree of laxity in each block, and suture with 9-0 silk
Resect the plica semilunaris on the nasal side (suturing is generally unnecessary), and resect and suture the junction of the superior and inferior conjunctiva on the temporal side
If there is superior conjunctival laxity, perform additional resection as needed
In this procedure, by excising the subconjunctival fibrous tissue including Tenon’s capsule, the conjunctiva adheres tightly to the scleral tissue, and tight adhesion is obtained postoperatively, so recurrence is rare.
In cases where filtration surgery (for glaucoma) may be performed in the future, the resection method is not appropriate; instead, choose a suturing method in which the lax conjunctiva is gathered toward the fornix and sutured to the sclera. Because subconjunctival lymphangiectasia remains, complete flattening is more difficult to achieve compared to the 3-block resection method.
For mild cases, a method of cauterizing and shrinking the lax conjunctiva is used. The reported rate of resolution of conjunctival redundancy after surgery is 80.6% 3). Derived techniques such as the paste-pinch-cut method and ultrasonic cauterization have also been reported 6).
This is a new treatment using a 4.0 MHz radio wave system (Ellman International), which reduces the lax conjunctiva with a thin electrode. Since it does not involve tissue carbonization, complications are fewer than with conventional methods. Youm et al. reported 90% complete resolution and significant improvement in OSDI scores in a study of 20 eyes from Korea 7). Trivli et al. also reported significant improvement in 40 eyes, with only mild conjunctival hyperemia as a postoperative complication 12). Ji et al. reported complete resolution in all cases in 40 eyes, with significant improvement in OSDI, TBUT, corneal staining, and tear meniscus area 8).
Sutures are removed 2 weeks after surgery. Until then, infection prevention and anti-inflammatory measures are thoroughly implemented. To prevent wound dehiscence, an eye patch is worn at bedtime for 1 week, and eye washing is permitted from 3 days after surgery. Patients are instructed not to rub their eyes when instilling eye drops.
The following postoperative prescriptions are recommended (when Tenon’s capsule excision is performed):
Levofloxacin (0.5%): 4 times daily
Betamethasone (0.1%): 6 times daily
If Tenon’s capsule excision is not required, fluorometholone (0.1%) 4 times daily is used instead of betamethasone. For 1 week after suture removal, levofloxacin 2 times daily and betamethasone 4 times daily are continued while tapering, until conjunctival hyperemia resolves.
Postoperative complications rarely include secondary lymphangiectasia and granuloma formation around sutures. The former is treated by drainage with a needle puncture, and the latter with steroid eye drops; if ineffective, excision is performed.
QCan conjunctivochalasis recur after surgery?
A
With the 3-block resection method (tear meniscus reconstruction), which excises subconjunctival fibrous tissue including Tenon’s capsule and achieves tight adhesion to the sclera, recurrence is considered rare. On the other hand, with suturing methods alone, lymphangiectasia under the lax conjunctiva may persist, leading to recurrence or incomplete flattening of the bulbar conjunctiva. The choice of surgical technique is determined based on the degree of laxity in each case and the presence or absence of glaucoma.
Histopathologically, the collagen and elastic fibers that make up the subconjunctival matrix become sparse, and the elastic fibers show fragmentation. In specimens from severe cases, subconjunctival microcapillary dilatation without inflammatory findings is partially observed, and a collection of fragmented elastic fibers and sparse collagen fibers is seen in many specimens. It has been proposed that mechanical forces between the lower eyelid and conjunctiva gradually impair lymphatic flow, leading to lymphatic dilatation and clinical conjunctivochalasis.
Conjunctivochalasis causes disturbances in three stages of tear film dynamics.
First, it impedes the flow of tears from the fornix to the tear meniscus, depleting the tear reservoir in the fornix. Symptomatic patients have a significantly slower tear meniscus recovery rate compared to asymptomatic patients1).
Second, the loose conjunctiva occupies the lower tear meniscus, causing the normal meniscus to disappear and an ectopic meniscus to form. This secondarily reduces tear film stability9).
Third, the nasal loose conjunctiva blocks tear flow to the punctum, causing epiphora. Surgical removal often improves this epiphora4).
The Japanese dry eye treatment guidelines state that in age-related conjunctivochalasis where the superior bulbar conjunctiva detaches from the sclera, and in superior limbic keratoconjunctivitis, increased friction during blinking also occurs in the Kessing space between the upper palpebral conjunctiva and bulbar conjunctiva, potentially causing epithelial damage and inflammation in both the palpebral and bulbar conjunctiva. Therefore, in superior limbic keratoconjunctivitis with superior conjunctivochalasis, surgery for superior conjunctivochalasis is effective.
Conjunctivochalasis is closely associated with meibomian gland dysfunction and meibomian gland dropout. Two hypotheses coexist: one that reduced lubrication due to lipid layer deficiency causes increased friction and traction on conjunctival tissue, and another that conjunctivochalasis affects blink completeness, secondarily causing meibomian gland dropout4). There are also reports that after conjunctival resection for conjunctivochalasis, OSDI, TBUT, corneal staining, and tear meniscus area all improved at 3 months4).
High-frequency radiofrequency electrosurgery (HFR-ES) can reduce redundant conjunctiva without tissue carbonization compared to conventional cautery or excision methods, with reported complete resolution rates of 90–100% and few postoperative complications, attracting attention3,7,8,12). New minimally invasive treatments such as plasma-based conjunctivoplasty, argon laser photocoagulation, and the paste-pinch-cut method have also been reported6).
There are still many unknowns regarding the basic biological mechanisms of LIPCOF and conjunctivochalasis and the boundary between them, and large-scale multicenter prospective studies using standardized evaluation methods are needed3).
Yokoi N, Komuro A, Nishii M, Inagaki K, Tanioka H, Kawasaki S, et al. Clinical impact of conjunctivochalasis on the ocular surface. Cornea. 2005;24(8 Suppl):S24-S31. doi:10.1097/01.ico.0000178740.14212.1a. PMID:16227820.
Mimura T, Yamagami S, Usui T, et al. Changes of conjunctivochalasis with age in a hospital-based study. Am J Ophthalmol. 2009;147(1):171-177.e1.
Ballesteros-Sánchez A, Sánchez-González JM, Borrone MA, Borroni D, Rocha-de-Lossada C. The influence of lid-parallel conjunctival folds and conjunctivochalasis on dry eye symptoms with and without contact lens wear: a review of the literature. Ophthalmol Ther. 2024;13(3):651-670.
Jones L, Downie LE, Korb D, et al. TFOS DEWS III management and therapy report. Am J Ophthalmol. 2025;269:341-396.
Marmalidou A, Kheirkhah A, Dana R. Conjunctivochalasis: a systematic review. Survey of ophthalmology. 2018;63(4):554-564. doi:10.1016/j.survophthal.2017.10.010. PMID:29128574.
Marmalidou A, Palioura S, Dana R, Kheirkhah A. Medical and surgical management of conjunctivochalasis. The ocular surface. 2019;17(3):393-399. doi:10.1016/j.jtos.2019.04.008. PMID:31009751.
Youm DJ, Kim JM, Choi CY. Simple surgical approach with high-frequency radio-wave electrosurgery for conjunctivochalasis. Ophthalmology. 2010;117(11):2129-33. doi:10.1016/j.ophtha.2010.02.023. PMID:20570365.
Ji YW, Seong H, Lee S, Alotaibi MH, Kim TI, Lee HK, et al. The correction of conjunctivochalasis using high-frequency radiowave electrosurgery improves dry eye disease. Scientific reports. 2021;11(1):2551. doi:10.1038/s41598-021-82088-5. PMID:33510304; PMCID:PMC7844232.
Chhadva P, Alexander A, McClellan AL, McManus KT, Seiden B, Galor A. The impact of conjunctivochalasis on dry eye symptoms and signs. Investigative ophthalmology & visual science. 2015;56(5):2867-71. doi:10.1167/iovs.14-16337. PMID:26024073; PMCID:PMC4419777.
Kiss HJ, Németh J. Isotonic Glycerol and Sodium Hyaluronate Containing Artificial Tear Decreases Conjunctivochalasis after One and Three Months: A Self-Controlled, Unmasked Study. PloS one. 2015;10(7):e0132656. doi:10.1371/journal.pone.0132656. PMID:26172053; PMCID:PMC4501551.
Le Q, Cui X, Xiang J, Ge L, Gong L, Xu J. Impact of conjunctivochalasis on visual quality of life: a community population survey. PloS one. 2014;9(10):e110821. doi:10.1371/journal.pone.0110821. PMID:25330252; PMCID:PMC4203838.
Trivli A, Dalianis G, Terzidou C. A Quick Surgical Treatment of Conjunctivochalasis Using Radiofrequencies. Healthcare (Basel, Switzerland). 2018;6(1). doi:10.3390/healthcare6010014. PMID:29439532; PMCID:PMC5872221.
Copy the article text and paste it into your preferred AI assistant.
Article copied to clipboard
Open an AI assistant below and paste the copied text into the chat box.