Rigid gas permeable contact lenses (RGP/HCL) are hard contact lenses made of oxygen-permeable material. They provide optical correction for keratoconus, post-traumatic corneal irregular astigmatism through the tear lens effect.
Soft contact lenses (SCLs) conform to the corneal shape and deform, so they have low ability to correct irregular astigmatism. In contrast, hard contact lenses (HCLs) form a stable tear film (tear lens) between the lens and the ocular surface during wear, masking corneal irregularities and providing a high-quality optical surface. According to Rabinowitz’s (1998) review of keratoconus, RGP lenses are established as a fundamental optical correction method for irregular astigmatism9). A review by Romero-Jiménez et al. (2010) also confirms that RGP fitting plays a central role in keratoconus management 10).
In cases where corneal astigmatism exceeds -3.0 D or keratoconus is suspected, even if SCLs provide some visual acuity, the quality of vision is inferior compared to HCLs. Moreover, as keratoconus progresses, SCLs may no longer provide sufficient vision, and switching to HCLs becomes difficult in many cases. When prescribing contact lenses for the first time, it is important to actively consider HCL prescription, taking into account the patient’s future quality of life.
QAfter a diagnosis of keratoconus, when are contact lenses needed?
A
In the early stages of keratoconus, glasses may provide adequate correction, but as irregular astigmatism progresses, glasses become insufficient. At that stage, HCLs (RGP lenses) become the first choice. If SCLs are used as a temporary measure while keratoconus progresses, switching to HCLs later may become difficult, so it is recommended to consult an ophthalmologist early and obtain a prescription.
At the stage when keratoconus patients become candidates for HCL fitting, the following subjective symptoms are typically observed.
Blurred or distorted vision: Decreased visual acuity due to irregular astigmatism, difficult to correct with glasses.
Monocular diplopia or polyopia: Multiple images due to light scattering from an irregular corneal surface.
Glare, halos, and glare: Ring-shaped or radial light disturbances around lights at night.
Difficulty wearing contact lenses: In advanced keratoconus, SCLs provide insufficient vision correction.
Frequent changes in glasses prescription: Rapid increase in myopia and astigmatism with progression.
In severe keratoconus, uncorrected visual acuity may decrease to counting fingers (CF), and improvement to 20/30 with scleral lenses has been reported (Almaweri 2025) 4). A review by Romero-Jiménez et al. (2010) also discusses the system of contact lens selection according to the stage of keratoconus progression 10).
Clinical Findings of Complications Associated with HCL Wear
Characteristic complication findings in eyes wearing HCLs are shown below.
3 and 9 o'clock staining
Location: Limited to the 3 and 9 o’clock positions of the corneal limbus
Cause: During blinking, the HCL moves up and down about 2 mm, causing local dryness when tears are drawn in from the 3 and 9 o’clock directions
Course: Mild cases heal in 3 to 5 days. If it progresses to erosion, it may take about 1 week and can leave corneal opacity
Corneal infiltration and infectious corneal ulcer
Non-infectious infiltration due to mechanical irritation: Mild hyperemia and white opacity of the peripheral cornea
Infectious corneal ulcer: Accompanied by the triad of hyperemia, discharge, and pain. Common causative organisms include Pseudomonas aeruginosa and Staphylococcus. Early initiation of culture testing and antimicrobial eye drops based on the AAO Bacterial Keratitis PPP (2024) 1) is important
Caution: If all three symptoms (hyperemia, discharge, pain) are present, suspect infectious keratitis and seek immediate medical attention
Other HCL-related findings include lens edge indentation when stuck, and pseudodendritic keratitis (which requires differentiation from herpetic keratitis).
All CLs reduce corneal sensitivity (hypoesthesia). Because reduced sensitivity may make it difficult for CL wearers to notice early symptoms of corneal damage, regular check-ups are especially important.
As keratoconus progresses, HCL wear becomes difficult in the following situations.
As the cone becomes more eccentric and asymmetric, poor centration and frequent lens dropout occur.
Insufficient apical clearance leads to direct contact of the HCL with the corneal apex (central touch).
In advanced cases (Amsler-Krumeich Grade 3–4; Kmax >55 D, corneal thickness <400 μm), achieving an appropriate fit becomes extremely difficult.
If corneal scarring appears, visual improvement becomes limited.
In such cases, consider transitioning to scleral lenses. Almaweri (2025) reported improvement from CF to corrected 20/30 with scleral lenses in severe keratoconus (Kmax 69.3 D)4).
Mechanical stimulation during blinking: HCL moves approximately 2 mm vertically with each blink, drawing in tears at the 3 and 9 o’clock positions. This localized dryness causes punctate superficial keratopathy.
Infection risk: Biofilm formation in the lens case is the main cause of infectious keratitis. Regular case replacement is essential.
Corneal hypoesthesia: Long-term HCL wear reduces corneal sensation (hypoesthesia), making it difficult to notice early symptoms of damage.
The CL prescription program “Itoi Method” built into the anterior segment OCT (CASIA, Tomey Corporation) uses BFS (best fit sphere) values that reflect corneal shape including paracentral and peripheral areas, and displays first trial lenses for lens diameters of 8.5 mm, 8.8 mm, and 9.4 mm. It is also effective in keratoconus and irregular astigmatism cases where keratometer values are not useful.
For normal cases where keratometer values can be used, there are the following three methods.
In keratoconus cases with large corneal astigmatism, fitting tends to be steep, so it is advisable to choose a value close to the flattest meridian value R1. Ultimately, the BC and size are determined by trial and error while checking the fitting pattern.
Fitting approach: apical clearance vs apical touch
There are two main approaches to HCL fitting for keratoconus.
Approach
Characteristics
Indications
Apical clearance type
The cone apex is vaulted to maintain clearance. Fluorescein shows green pooling at the apex.
Mild to moderate. Minimizes mechanical stimulation to the apex.
Apical touch type (three-point touch)
Support at three points: cone apex, mid-periphery, and far periphery. Centration is more stable.
Advanced cases. However, apical stimulation carries a risk of scar formation.
Recently, many facilities recommend the apical clearance type. To prevent corneal scarring and nipple formation due to mechanical stimulation of the apex, fitting that maintains a slight clearance is preferred. In a comparative study by Yıldız Taşcı et al. (2023), there was no significant difference in corrected visual acuity between RGP and hybrid CLs in advanced keratoconus, and selection according to the patient’s lifestyle and tolerance is appropriate8).
Criteria for considering transition to scleral lenses:
Recurrent pain and corneal epithelial damage during HCL wear
Clear apical scar and unavoidable central touch
In a report by Almaweri (2025), even in severe cases with Kmax 69.3 D, visual acuity improvement to 20/30 was achieved with scleral lenses 4), making it a viable option to avoid surgery.
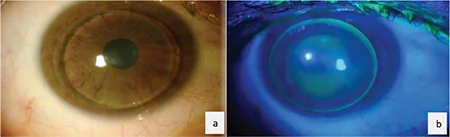
Almaweri A, Muacevic A, Adler JR, et al. Interpalpebral Fitting Philosophy: A Rarely Used Approach to Keratoconus Management With Corneal Rigid Gas-Permeable (RGP) Contact Lenses. Cureus. 2025;17:e91961. Figure 3. PMID: 41080328; PMCID: PMC12512222. DOI: 10.7759/cureus.91961. License: CC BY 4.0.
Slit-lamp findings (a) and fluorescein staining pattern under cobalt blue light (b) of a Rose K2 RGP lens worn on a progressive keratoconus eye. In (b), green fluorescein pooling (clearance) is observed at the corneal apex (center of the cone), while the peripheral area appears as a dark band with a thin tear layer. This pattern is a typical finding of the apical clearance type, which is the standard for RGP fitting evaluation. This corresponds to the fluorescein fitting evaluation discussed in the “Diagnosis and Examination Methods” section.
Fitting examination is first performed at low magnification to check the balance between the palpebral fissure width and the HCL without staining. Fitting is confirmed with fluorescein staining, but excessive tearing can lead to misjudgment, so wait until tearing subsides or use topical anesthetics to achieve an appropriate tear volume before evaluation.
The relationship between the base curve (BC) and corneal curvature is determined by the positional relationship when the lens is centered.
If the spherical power of the additional correction exceeds ±3.0 to 4.0 D, the effect of corneal vertex distance (12 mm) becomes significant. Calculation using a corneal vertex distance correction table is necessary.
Depending on the HCL fitting pattern, the tear film may act like a lens (tear lens effect), and note that changing the BC alters the spherical power. Flattening the BC by 0.05 mm makes the tear lens act as a concave lens (-0.25 D), while steepening by 0.05 mm makes it act as a convex lens (+0.25 D).
QI heard that cataract surgery after LASIK often results in refractive errors. Is this also a problem with RGP lenses?
A
In RGP lens fitting after LASIK, the flattening of the anterior corneal surface makes BC selection different from usual. Fitting must be performed after understanding the actual corneal shape through corneal topography. Rather than relying solely on keratometer values, using anterior segment OCT enables appropriate fitting.
Basic care of HCL involves cleaning and rinsing. Disinfection is generally not required, but for lenses with complex shapes such as orthokeratology lenses, disinfection is recommended even for HCL.
For stubborn deposits that do not come off with routine care, use of a dedicated cleaner is recommended. However, caution is needed because abrasive cleaners cannot be used with some HCL. Early diagnosis and treatment of contact lens-related infectious keratitis should follow the Infectious Keratitis Clinical Practice Guidelines (3rd edition)11). Sonsino and Mathe (2013) provide guidance on corneal clearance management during scleral lens wear12). Schornack (2015) also reviews scleral lens design, prescribing, and management13). Visser et al. (2007) describe clinical characteristics of scleral lenses, and the AAO Corneal Ectasia PPP (2024)7) provides evidence-based recommendations for keratoconus management15).
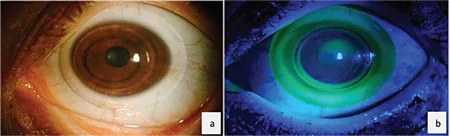
Şengör T, Aydın Kurna S, Aksoy S. Update on Contact Lens Treatment of Keratoconus. Turk J Ophthalmol. 2020;50(4):234-244. Figure 8. PMID: 32854468; PMCID: PMC7469902. DOI: 10.4274/tjo.galenos.2020.70481. License: CC BY 2.5.
Slit-lamp findings (a) and fluorescein staining pattern under cobalt blue light (b) of an AirFlex hybrid contact lens worn on a progressive keratoconic eye. In (b), green pooling (clearance over the corneal apex) is observed under the central rigid zone, and the boundary with the peripheral soft skirt appears as a ring. Hybrid lenses are an option for patients who have difficulty wearing RGP lenses alone, maintaining RGP optics while improving stability. This corresponds to an alternative option before transitioning to scleral lenses, discussed in the section “Standard Treatment.”
For advanced irregular astigmatism and keratoconus cases that are difficult to manage with HCL, scleral contact lenses become a strong option. Scleral lenses are rigid gas-permeable lenses that vault over the entire cornea and rest on the sclera, forming a fluid reservoir between the lens and the cornea6).
In a study of 846 eyes, only 1.65% required corneal transplantation after using scleral lenses, suggesting that even advanced keratoconus may avoid corneal transplantation 4).
BostonSight PROSE (Prosthetic Replacement of the Ocular Surface Ecosystem) is a treatment model using a highly customizable prosthetic device that received FDA approval in 1994 3). It allows specification across up to eight independent meridians, accommodating complex ocular surface shapes compared to the 2-4 meridians of commercially available scleral lenses 3).
Scleral lenses can be prescribed as self-pay treatment at some specialized facilities and are also used for severe dry eye conditions such as ocular cicatricial pemphigoid and Stevens-Johnson syndrome6). The TFOS DEWS III Management and Treatment Report (2025) describes the role of scleral lenses in managing severe dry eye6). Schornack and Patel (2010) provided practical guidelines for scleral lens management in keratoconus15), serving as a useful reference for treatment strategies to avoid corneal transplantation. The AAO Corneal Edema and Opacity PPP (2024) 2) is also referenced as a criterion for corneal transplantation indications.
Initial trial: Start with a standard design of 16-18 mm diameter. Assess clearance with fluorescein and anterior segment OCT.
Customization: Adjust the landing zone curve to achieve a stable fit without compression or air bubbles.
Wear training: Practice insertion and removal. Use assistive devices such as a plunger if removal is difficult.
Regular follow-up: Check corneal endothelial density and clearance changes every 3-6 months.
Measures for midday fogging: Minimizing air bubble entrapment during fitting and using lenses with SmartChannels design can be expected to improve this condition6). Replacing the filling solution is also effective. In the clinical characteristics report by Visser et al. (2007), the 1-year continuation rate was 73%, and the main reason for discontinuation was difficulty in insertion and removal14).
QBy when should IOL exchange be performed (in case of transition to scleral lenses)?
A
When HCL becomes difficult to wear in keratoconus, transitioning to scleral lenses is recommended. Even in advanced keratoconus (Amsler-Krumeich Grade 4), improvement from uncorrected visual acuity (counting fingers) to corrected visual acuity of 20/30 has been reported with scleral lenses4). Consult an ophthalmologist when HCL fitting becomes difficult to determine the timing of transition.
When wearing HCL, the front surface of the lens provides a stable optical surface, and a tear lens is formed between the back surface of the lens and the front surface of the cornea. This tear lens corrects corneal irregular astigmatism, thereby exerting the corrective effect of HCL.
The three-zone structure of scleral lenses is as follows:
Optical zone: The front surface is a spherical or aspherical design responsible for optical correction. It forms a fluid vault between the back surface and the front surface of the cornea.
Landing zone (haptic): The peripheral portion that rests on the corneoscleral limbus and sclera. It provides lens stability and centration. SmartChannels (radial grooves) facilitate tear exchange.
Edge zone: The outer edge of the landing zone. Designed to minimize pressure on the ocular surface.
The clearance of the fluid vault is generally considered appropriate at 200–500 μm. Since it decreases by approximately 100–150 μm due to settling into the conjunctival tissue several hours after insertion, the initial setting must account for this change. Sonsino and Mathe (2013) measured clearance changes after insertion and reported the importance of appropriate initial settings12).
The combination of high Dk materials (Dk 141–180) and low center thickness (CT 0.30–0.35 mm) maximizes oxygen supply to the cornea3).
Friction between the HCL and the ocular surface during blinking causes epithelial damage. With HCL, the lens moves approximately 2 mm vertically with each blink, drawing in tears from the 3 and 9 o’clock directions. At that time, tears become depleted in those areas, leading to punctate keratopathy. When mechanical stimulation from the lens edge is added, it can progress to corneal erosion or corneal infiltration.
Biofilm formation in lens cases is an important risk factor for infectious keratitis, and regular replacement of the lens case is key to prevention.
Before wearing: Rub the lens with a dedicated cleaner and rinse thoroughly with saline solution.
After wearing: After cleaning, store the lens in a dedicated storage solution (do not use tap water or distilled water).
Lens case management: Rinse the case with dedicated solution after daily use, and let it dry upside down. Replace every 1 to 3 months.
Special cleaners: Perform protein removal treatment once a week. Some abrasive cleaners cannot be used with certain lens materials, so confirmation is necessary.
Emergency response: If eye discharge, redness, pain, or decreased vision occurs, immediately discontinue use and visit a doctor on the same day, suspecting infectious keratitis1).
In infectious keratitis associated with keratoconus, there is a risk of rapid progression due to structural corneal weakness, so early consultation, early culture, and early antimicrobial treatment are key to improving visual prognosis.
Research is underway to utilize the fluid reservoir of scleral lenses as a drug delivery platform. Improvements in corneal neovascularization by filling the reservoir with bevacizumab (anti-VEGF drug) and application of cyclosporine 0.05% for dry eye treatment have been reported6).
SmartChannels (radial grooves on the back surface of the haptic) are designed to promote tear exchange and reduce suction pressure under the lens3). Fenestrations (small holes of 0.25–0.50 mm diameter) for air ventilation are also used in cases with corneal endothelial dysfunction.
Scleral lenses are also useful for Stevens-Johnson syndrome, Sjögren’s syndrome, chronic ocular GVHD, and exposure keratopathy (CPEO), with dramatic improvements in OSDI (Ocular Surface Disease Index) scores (95.83 → 4.17) reported5). In KID syndrome, PROSE wear maintained regression of corneal epithelial plaques and long-term stability of the ocular surface3).
In a report on the clinical characteristics of scleral lenses by Visser et al. (2007), high continuation rates and patient satisfaction were reported 14), contributing to improved quality of life in cases of advanced irregular astigmatism.
For cases where RGP lenses alone are difficult to wear, hybrid contact lenses with a central RGP and a peripheral soft skirt are an option. A comparative study by Yıldız Taşcı et al. (2023) showed that corrected visual acuity with RGP and hybrid CLs was equivalent in moderate and advanced keratoconus8). Hybrid CLs may cause less foreign body sensation and offer better wearing comfort than RGP lenses.
Midday fogging of scleral lenses, a phenomenon of decreased vision during the day, is caused by debris accumulation in the tear reservoir. Adding SmartChannels and proper fitting are countermeasures 6). High-quality comparative studies supporting the use of scleral lenses in dry eye management are currently lacking 6), and prospective long-term studies are expected in the future. The AAO Corneal Ectasia PPP (2024) 7) states that contact lenses play a central role in the management of keratoconus, and a stepwise approach from RGP to scleral lenses is recommended.
American Academy of Ophthalmology. Bacterial Keratitis Preferred Practice Pattern. Ophthalmology. 2024;131(2):P265-P330.
American Academy of Ophthalmology. Corneal Edema and Opacification Preferred Practice Pattern. Ophthalmology. 2024.
Gagliardi M, Asghari B. Two cases of therapeutic scleral lenses for KID syndrome. American journal of ophthalmology case reports. 2025;37:102261. doi:10.1016/j.ajoc.2025.102261. PMID:39927073; PMCID:PMC11804770.
Almaweri A. Avoiding Surgery: Successful Management of a Patient With Severe Keratoconus Using Scleral Contact Lenses. Cureus. 2025;17(8):e90263. doi:10.7759/cureus.90263. PMID:40964594; PMCID:PMC12438945.
Erdinest N, Shemesh N, London N, Landau D, Lavy I. Chronic Progressive External Ophthalmoplegia (CPEO): Rehabilitation utilizing scleral contact lenses. American journal of ophthalmology case reports. 2025;39:102411. doi:10.1016/j.ajoc.2025.102411. PMID:41017819; PMCID:PMC12460078.
Tear Film & Ocular Surface Society. TFOS DEWS III Management and Therapy Report. Am J Ophthalmol. 2025;279:72-178.
Jhanji V, Ahmad S, Amescua G, et al. Corneal Ectasia Preferred Practice Pattern. Ophthalmology. 2024 Apr;131(4):P205-P246. doi:10.1016/j.ophtha.2023.12.038. PMID:38349299.
Taşcı YY, Saraç Ö, Çağıl N, Yeşilırmak N. Comparison of Hybrid Contact Lenses and Rigid Gas-Permeable Contact Lenses in Moderate and Advanced Keratoconus. Turkish journal of ophthalmology. 2023;53(3):142-148. doi:10.4274/tjo.galenos.2022.82754. PMID:37345297; PMCID:PMC10286838.
Sonsino J, Mathe DS. Central corneal clearance in patients successfully wearing scleral lens for keratoconus. Optom Vis Sci. 2013;90:e272-e278.
Schornack MM. Scleral lenses: a literature review. Eye Contact Lens. 2015;41(1):3-11. doi:10.1097/ICL.0000000000000083. PMID:25536528.
Visser ES, Visser R, van Lier HJ, Otten HM. Modern scleral lenses part I: clinical features. Eye & contact lens. 2007;33(1):13-20. doi:10.1097/01.icl.0000233217.68379.d5. PMID:17224674.
Schornack MM, Patel SV. Scleral lenses in the management of keratoconus. Eye Contact Lens. 2010;36(1):39-44. doi:10.1097/ICL.0b013e3181c786a6. PMID:20009945.
Copy the article text and paste it into your preferred AI assistant.
Article copied to clipboard
Open an AI assistant below and paste the copied text into the chat box.