Corneal warpage is a change in corneal shape caused by persistent mechanical compression and hypoxia from contact lens (CL) wear, especially long-term wear of hard contact lenses (HCLs). It is detected as irregular shape changes on corneal topography and is an important issue in eligibility evaluation before refractive surgery.
Corneal disorders caused or triggered by CLs range from asymptomatic mild cases to severe cases. Warpage itself is a functional concept of corneal shape change and is characterized by not necessarily involving clear corneal stromal lesions.
The Japanese Ophthalmological Society Guidelines for Refractive Surgery (8th edition) contraindicate refractive surgery in cases suspected of corneal ectasia such as keratoconus1), and reliable differentiation between CL-induced warpage and keratoconus is a core issue in preoperative evaluation. The AAO Corneal Ectasia PPP also strongly recommends topographic screening before refractive surgery 2).
Pathological Warpage
Cause: Unintentional corneal shape change due to long-term wear of HCL/SCL
Mechanism: Corneal stromal deformation and epithelial metabolic disorder due to mechanical pressure and hypoxia
Features: Refractive fluctuation and irregular pattern on topography
Management: Discontinue CL and confirm shape stability
Intentional Warpage (Orthokeratology)
Cause: Intentional central corneal flattening with overnight lenses
Mechanism: Central epithelial thinning and mid-peripheral corneal thickening
Management: Strict regular examinations and follow-up
QWhat is corneal warpage?
A
Corneal warpage is a condition in which the shape of the cornea is unintentionally deformed due to mechanical pressure and hypoxia from long-term wear of contact lenses (especially hard CLs). It is detected as an irregular pattern on corneal topography. Although correction with glasses or CLs may become unstable, it often recovers within weeks to months after discontinuing CL use. When considering refractive surgery, it is essential to confirm shape stability after CL discontinuation.
Pathological warpage is often asymptomatic and is frequently discovered incidentally during pre-refractive surgery examinations. The following symptoms may appear.
Subjective Symptoms
Characteristics/Frequency
Instability of refractive correction
Glasses or contact lenses no longer correct vision as well as before
Blurred vision, flickering
Light scatter due to increased higher-order aberrations
Glare, halos
Decreased visual function due to irregular astigmatism
Asthenopia (eye strain)
Accommodative fatigue due to unstable refraction
Corneal sensation is usually preserved, so there are no inflammatory symptoms such as pain or redness. The fact that it is often asymptomatic increases the importance of screening before refractive surgery.
Corneal topography findings: Asymmetric distortion, central flattening or steepening are observed. In HCL-induced cases, asymmetric patterns often appear on the nasal, temporal, superior, and inferior sides. With Placido disc systems, it is detected as irregularity of the contour pattern; with Scheimpflug systems, it is detected as abnormalities in topography, pachymetry, and elevation maps.
Use of epithelial thickness maps: Reinstein et al. showed that in corneal warpage, the epithelium accumulates centrally (becomes uniform and thickened), whereas in keratoconus, epithelial thinning occurs first, and this difference is useful for differentiation 3).
Normal findings after orthokeratology: A concentric pattern called a bull’s eye is observed with fluorescein staining. From the center to the periphery, it forms a pattern of four concentric circles: dark (base curve area) → bright (fluorescein ring) → dark (alignment curve area) → bright (edge clearance area).
Recovery after CL discontinuation: After discontinuing contact lenses, the shape recovers over several weeks to months. In HCL, recovery may take several months. In SCL, because changes are mainly epithelial, recovery tends to be relatively rapid.
HCL (hard contact lens)-induced warpage: The most pronounced shape change. The main mechanism is sustained deformation of the corneal stroma due to mechanical compression. It tends to occur with long-term wear (especially over 10 years). Improper fitting (flat fit) increases compression. Posterior corneal examination using Scheimpflug imaging is useful for differentiating warpage from keratoconus2).
SCL (soft contact lens)-induced warpage: The main mechanism is metabolic disturbance of the corneal epithelium and stroma due to hypoxia, leading to edematous shape change. It is often milder than HCL-induced warpage. Hypoxia-related warpage has decreased since the widespread use of silicone hydrogel lenses 4).
Orthokeratology (intentional warpage): Wearing overnight reverse-geometry lenses thins the central corneal epithelium and increases corneal thickness in the mid-periphery, reducing myopia and improving uncorrected visual acuity. This is intentionally induced warpage and is reversible after discontinuation of CL wear.
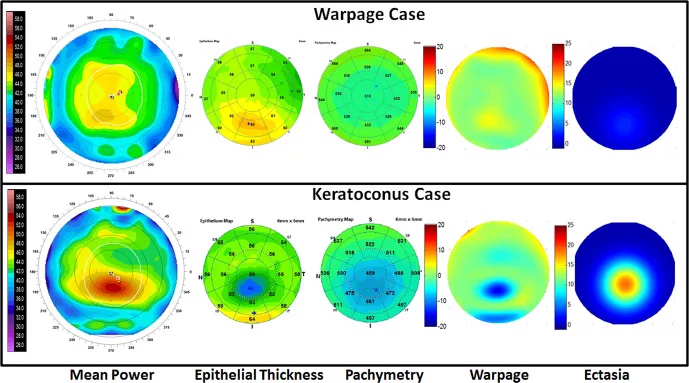
Reinstein DZ, et al. Differentiating Keratoconus and Corneal Warpage by Analyzing Focal Change Patterns in Corneal Topography, Pachymetry, and Epithelial Thickness Maps. Invest Ophthalmol Vis Sci. 2016;57(9):OCT544-OCT549. Figure 1. PMCID: PMC4978086. License: CC BY 4.0.
CL-induced warpage (top row) and keratoconus (bottom row) both show inferior corneal steepening, but the epithelial thickness map shows epithelial thickening in warpage and epithelial thinning in keratoconus, and only the ectasia index clearly distinguishes the two. This corresponds to the differential diagnosis of corneal warpage and keratoconus discussed in the section “4. Diagnosis and Examination Methods.”
Corneal topography (essential): Placido disc or Scheimpflug type. Comparison before and after CL discontinuation is important. Evaluate for irregular patterns and asymmetric shape changes. Scheimpflug type allows evaluation of both anterior and posterior corneal surfaces; posterior elevation changes are important early signs of keratoconus2).
Subjective refraction: Fluctuation in refractive values (multiple measurements). Comparison during CL wear and after discontinuation is useful.
Pachymetry (corneal thickness measurement): Useful for evaluating corneal edema and stromal changes. If the thinnest corneal thickness location is displaced, suspect keratoconus.
Slit-lamp microscopy: Check for epithelial damage, stromal opacity, and corneal neovascularization. Use fluorescein staining to confirm the bull’s-eye pattern after orthokeratology.
Epithelial thickness map (OCT): Warpage shows a pattern of uniform thickening, while keratoconus shows thinning3).
Corvis ST (corneal biomechanical assessment): Evaluation of corneal biomechanical weakness is becoming a complementary indicator for differentiating warpage from early keratoconus5).
When considering refractive surgery (LASIK, SMILE, PRK, etc.), surgery is contraindicated in cases suspected of keratoconus1). In cases with warpage, irregular shape persisting after sufficient CL discontinuation may be a contraindication for surgery, requiring careful evaluation.
QHow do you differentiate corneal warpage from keratoconus?
A
The most important method is to evaluate corneal shape over time after discontinuation of contact lenses. In corneal warpage, the shape normalizes within weeks to months after CL cessation. In keratoconus, the shape does not stabilize and progressive changes continue. Evaluation of the posterior corneal surface with Scheimpflug camera (e.g., Pentacam) is useful for differentiation; in keratoconus, posterior elevation changes may precede anterior changes. Since refractive surgery is contraindicated in suspected keratoconus, careful differentiation is necessary.
Discontinuation of CL use: The most important treatment. For HCL, at least 4 weeks of discontinuation is recommended. For SCL, 1–2 weeks or more. After discontinuation, repeat topography until shape stabilizes.
Confirmation of shape recovery: Check recovery with regular topography. Initially every 2 weeks, then monthly once stable. Do not evaluate surgical candidacy until shape stabilizes.
Resuming CL use: After shape recovery, consider refitting and appropriate lens type selection. If improper fitting was the cause, adjust the fit.
Management before refractive surgery: Determine surgical candidacy after adhering to CL discontinuation period and confirming shape stability with repeated topography 1).
Contraindications for orthokeratology include active keratitis, significant dry eye, and other conditions similar to those for regular contact lenses, as well as cases where uncorrected refractive values or corneal shape are outside the indicated range. The Japan Contact Lens Society’s Orthokeratology Guidelines (2nd edition) recommends cleaning with a surfactant, disinfection with povidone-iodine, and regular lens case replacement and drying 6).
The 8th edition of the Refractive Surgery Guidelines states that refractive surgery is contraindicated in cases of suspected keratoconus1). In cases with warpage, irregular corneal shape that persists after sufficient discontinuation of contact lenses may be a contraindication, requiring careful evaluation.
QDoes the cornea return to its original shape after stopping orthokeratology?
A
Yes, corneal shape changes induced by orthokeratology are reversible. When lens wear is discontinued, central epithelial thinning and mid-peripheral thickening resolve, and the corneal shape returns to its original state. The recovery time varies among individuals, but in most cases, the original shape is restored within a few days to weeks. However, patients should be informed in advance that uncorrected visual acuity may fluctuate during the recovery period.
The main mechanisms of warpage caused by HCL are the following two.
Mechanical compression: The lens directly contacts the cornea, applying continuous physical stress to the corneal stroma. Inappropriate fitting (flat fit) increases compression. Prolonged continuous compression alters the arrangement of collagen fibers in the corneal stroma, deforming the corneal shape.
Hypoxia: Insufficient oxygen supply to the cornea due to low Dk HCL or extended wear. Hypoxia causes metabolic disturbances in the corneal epithelium, leading to epithelial and stromal edema that induces shape changes. Chronic hypoxia leads to corneal stromal thinning and changes in fiber arrangement 4).
The main cause is metabolic disturbance of the corneal epithelium and stroma due to hypoxia, with edematous changes in the epithelium affecting the anterior corneal shape. Compared to mechanical compression from HCL, it is often milder. With the widespread use of silicone hydrogel lenses, SCL-induced warpage has decreased, but it can still occur with extended wear or overnight wear 4).
By wearing reverse geometry lenses at night, the central corneal epithelium becomes mechanically thinner (central epithelial thinning), and the displaced epithelium moves to the mid-periphery, causing thickening (formation of a bearer zone). This results in a decrease in central corneal curvature (flattening), reducing the spherical equivalent of myopia. These changes are reversible and primarily involve the epithelium; after lens discontinuation, the original shape is restored.
In pathological warpage, when CL use is discontinued and mechanical compression and hypoxic stimulation are removed, corneal stromal and epithelial homeostasis is restored and the shape returns to normal. In HCL, stromal deformation may be present and recovery takes time, whereas in SCL, changes are mainly epithelial, so recovery tends to be relatively rapid.
Individual differences in recovery speed are determined by the following factors.
If HCL-induced warpage takes more than 3 months to recover, consider additional tests (confocal microscopy, Corvis ST, etc.) to rule out keratoconus or other corneal diseases.
The TFOS CLEAR report suggests that long-term CL wear affects corneal biomechanical properties, potentially leading to changes in corneal hysteresis and corneal resistance factor 8). These changes can be measured with Corvis ST and are expected to be applied as complementary indicators for warpage evaluation in the future 5).
Orthokeratology has been reported to suppress myopia progression by intentionally altering corneal shape (warpage). In particular, evidence for its effectiveness in inhibiting axial elongation in children and young adults is accumulating, and its indications are expanding in Japan. It is important to perform it safely under strict management according to the Orthokeratology Guidelines (2nd edition) 6).
Combined with corneal biomechanical evaluation using Corvis ST, the accuracy of differentiating CL-induced warpage from early keratoconus has improved 5). Biomechanical vulnerability assessment is becoming a complementary indicator for warpage diagnosis. The AAO Corneal Ectasia PPP emphasizes the importance of biomechanical evaluation before refractive surgery 2).
Machine learning and deep learning applied to corneal topography data are being attempted for automated differentiation of warpage patterns and keratoconus. Implementation as a diagnostic support tool is expected.
TFOS CLEAR classifies warpage as a “mechanical/hypoxic disorder” in the classification of CL-related complications 8), and points out the importance of risk factor stratification and prevention through changes in CL material and wearing schedule. Although hypoxic-related warpage has decreased with the widespread use of SiHy lenses, HCL-induced warpage due to mechanical compression can still be problematic 8).
Corneal warpage can be understood as a form of CL intolerance. Long-term HCL wear causing mechanical warpage can contribute to CL intolerance through a pathway of corneal shape instability → difficulty in refractive correction → wearing discomfort. When warpage is detected, revision of CL prescription (change to SCL, higher Dk value, improved fitting) should be actively considered, and evaluation of dry eye background is also important 9).
Corneal warpage itself is a non-infectious change, but long-term HCL wearers also have an infection risk associated with CL use. The AAO Bacterial Keratitis PPP identifies CL wear as the greatest risk for infectious keratitis 10), and appropriate CL care and regular examinations are essential for infection prevention even in warpage patients. The Infectious Keratitis Clinical Practice Guidelines (3rd edition) strongly recommend culture testing for CL-related keratitis 7), and in CL wearers with warpage who present with the triad of hyperemia, discharge, and pain, culture should be performed promptly. Extended wear of SiHy lenses has been shown to increase the annual incidence of CIE 11), and continuous wear should be avoided in warpage patients.
TFOS DEWS III explicitly states that contact lens wear is a risk factor for dry eye12), and dry eye is frequently comorbid in contact lens wearers with corneal warpage. Dry eye reduces tear film protection, creating a vicious cycle that promotes mechanical warpage. It is desirable to incorporate dry eye evaluation and treatment into the management of warpage patients.
AK is a serious complication in contact lens wearers 13). For patients found to have warpage, individual guidance on prohibiting overnight wear, proper care, and regular check-ups is necessary when planning contact lens reuse.
The TFOS Lifestyle report provides a detailed analysis of the relationship between the digital environment and contact lens-related complications 14). The combination of prolonged screen work and HCL wear may increase the risk of corneal shape changes due to hypoxia and dryness.
Preoperative topographic screening is essential for evaluating candidacy for keratorefractive lenticule extraction (KLEx) such as SMILE15). In cases with warpage, sufficient evaluation after contact lens discontinuation is necessary.
Warpage resulting from long-term HCL wear causes discomfort due to unstable vision correction with glasses or contact lenses, manifesting as a symptom of contact lens intolerance. Management strategies are as follows:
Switch to SCLs: Changing from HCL to SCL eliminates mechanical compression and prevents progression of warpage.
Active recommendation of daily disposable lenses: Eliminates the risk of poor care and prevents infectious complications.
Optimization of fitting: Correction of improper fitting (flat fit).
Setting a contact lens-free period: Once warpage is confirmed, discontinue contact lenses for a certain period to stabilize corneal shape before re-evaluating contact lens prescription.
If a patient with warpage desires refractive surgery, it is essential to follow the above steps: sufficient contact lens discontinuation → confirmation of shape stability → preoperative examination 1).
QHow long before refractive surgery should contact lens use be discontinued?
A
When considering refractive surgery (such as LASIK or SMILE), it is recommended to stop wearing hard contact lenses (HCL/RGP) for at least 4 weeks 1). For soft contact lenses, a discontinuation period of 1 to 2 weeks or more is recommended. However, since the time required for the cornea to stabilize varies among individuals, it is important to confirm stability through multiple corneal topography measurements before evaluating surgical candidacy. Those who have used orthokeratology may need a longer discontinuation period.
Jhanji V, Ahmad S, Amescua G, et al. Corneal Ectasia Preferred Practice Pattern. Ophthalmology. 2024 Apr;131(4):P205-P246. doi:10.1016/j.ophtha.2023.12.038. PMID:38349299.
Tang M, Li Y, Chamberlain W, Louie DJ, Schallhorn JM, Huang D. Differentiating Keratoconus and Corneal Warpage by Analyzing Focal Change Patterns in Corneal Topography, Pachymetry, and Epithelial Thickness Maps. Investigative ophthalmology & visual science. 2016;57(9):OCT544-9. doi:10.1167/iovs.15-18938. PMID:27482824; PMCID:PMC4978086.
Stapleton F, Bakkar M, Carnt N, Chalmers R, Vijay AK, Marasini S, et al. CLEAR - Contact lens complications. Contact lens & anterior eye : the journal of the British Contact Lens Association. 2021;44(2):330-367. doi:10.1016/j.clae.2021.02.010. PMID:33775382.
Renato Ambrósio Jr, Isaac Ramos, Allan Luz, Fernando Correa Faria, Andreas Steinmueller, Matthias Krug, Michael W. Belin, Cynthia Jane Roberts. Dynamic ultra high speed Scheimpflug imaging for assessing corneal biomechanical properties. Rev. bras.oftalmol. 2013;72(2):99-102. doi:10.1590/s0034-72802013000200005.
James S. Wolffsohn, Philip B. Morgan, Melissa Barnett, Laura E. Downie, Deborah S. Jacobs, Lyndon Jones, Kathryn Richdale, Fiona Stapleton, et al. Contact Lens Evidence-Based Academic Reports (CLEAR). Contact Lens and Anterior Eye. 2021;44(2):129-131. doi:10.1016/j.clae.2021.02.011.
American Academy of Ophthalmology. Bacterial Keratitis Preferred Practice Pattern. Ophthalmology. 2024;131(2):P265-P330.
Loretta Szczotka‐Flynn, Mireya Diaz. Risk of Corneal Inflammatory Events with Silicone Hydrogel and Low Dk Hydrogel Extended Contact Lens Wear: A Meta‐Analysis. OVS. 2007;84(4):247-256. doi:10.1097/opx.0b013e3180421c47.
Jones L, Craig JP, Markoulli M, Karpecki P, Akpek EK, Basu S, et al. TFOS DEWS III: Management and Therapy. American journal of ophthalmology. 2025;279:289-386. doi:10.1016/j.ajo.2025.05.039. PMID:40467022.
Carnt N, Minassian DC, Dart JKG. Acanthamoeba Keratitis Risk Factors for Daily Wear Contact Lens Users: A Case-Control Study. Ophthalmology. 2023;130(1):48-55. doi:10.1016/j.ophtha.2022.08.002. PMID:35952937.
Wolffsohn JS, Lingham G, Downie LE, et al. TFOS Lifestyle: Impact of the digital environment on the ocular surface. Ocul Surf. 2023;28:213-252. doi:10.1016/j.jtos.2023.04.004.
Wang Y, Xie L, Yao K, Sekundo W, Alió JL, Mehta JS, Goel S, Elmassry A, Schallhorn J, Shilova T, Cao H, Xu L, Chen X, Zhang F, Bai J, Zhang W, Liu Q, Zhou X, Chen Y, Wang Z, Jhanji V, Yang K, Writing Committee for the Guideline Working Group. Evidence-Based Guidelines for Keratorefractive Lenticule Extraction Surgery. Ophthalmology. 2025;132(4):397-419. doi:10.1016/j.ophtha.2024.11.016. PMID:39577672.
Copy the article text and paste it into your preferred AI assistant.
Article copied to clipboard
Open an AI assistant below and paste the copied text into the chat box.