Keratoconus is the most representative corneal ectatic disorder. The central or paracentral cornea progressively thins and steepens, causing the cornea to protrude forward in a conical shape. When the corneal shape is distorted due to stromal weakening, high irregular astigmatism occurs and visual function is impaired1).
Onset is typically during adolescence, with progression through the 20s and 30s, and progression often halts or slows around age 301). Onset before age 10 is rare, and the typical age at diagnosis is 15 to 30 years. There is a slight male predominance.
Prevalence varies significantly by region and ethnicity: 1:375 (approximately 265 per 100,000) in the Netherlands, 1:84 among the 20-year-old population in Australia, and up to 1:45 in certain ethnic groups2). With the recent spread of corneal tomography, detection of early cases has advanced, and the number of diagnoses and prevalence rates are increasing1). A family history was noted in 14% of 1,209 participants in the CLEK study, and the prevalence among first-degree relatives has been reported at 20.5%1).
Keratoconus is bilateral in the vast majority of cases but often presents with interocular asymmetry in severity, and some cases may appear to have clinical findings in only one eye. However, detailed corneal tomography often detects mild abnormalities in the fellow eye as well. Discordant cases in monozygotic twins have been reported, indicating that environmental factors play a decisive role in pathogenesis in addition to genetic predisposition6). Most cases are sporadic, but familial occurrence is also observed1).
The prevalence of keratoconus is being revised upward with the widespread use of corneal tomography. It was once estimated at approximately 5 per 10,000 people, but it is now recognized as a more frequently encountered disease1). This is interpreted not as an actual increase in incidence but as a result of improved detection sensitivity for forme fruste and early-stage cases. Since the 2000s, with the growing demand for screening prior to corneal refractive surgery, three-dimensional corneal analysis using Scheimpflug imaging and anterior segment OCT has been integrated into routine clinical practice. This has shifted the diagnostic landscape from identifying only moderate-to-advanced cases with subjective symptoms to detecting asymptomatic or mildly symptomatic early-stage cases.
In contrast to typical keratoconus, which is characterized mainly by protrusion of the anterior corneal surface, posterior keratoconus is a rare, non-progressive corneal ectasia characterized by an increase in posterior corneal curvature. It is primarily congenital, unilateral, and sporadic, and is usually asymptomatic without causing visual impairment. Clinically, differentiation from typical keratoconus is important, and management consists of observation and refractive correction when needed.
QDoes keratoconus occur in both eyes?
A
Keratoconus is bilateral in most cases, but interocular asymmetry is common. Even when it appears to affect only one eye, detailed corneal topography or tomography often reveals mild abnormalities in the fellow eye. Discordant cases have been reported in monozygotic twins where only one twin develops the condition, suggesting that environmental factors such as eye rubbing play an important role in pathogenesis alongside genetic predisposition.
In the early stage, frequent changes in spectacle prescription over a short period and the inability to achieve adequate corrected visual acuity are characteristic 1). As the disease progresses, myopia and irregular astigmatism increase, necessitating a transition from soft contact lenses to toric lenses and then to rigid gas-permeable contact lenses. Some patients report a distinctive visual phenomenon in which point light sources or targets appear to have a comet-like tail extending downward, caused by a marked increase in higher-order corneal aberrations, particularly vertical coma.
Visual impairment is often a late finding that appears after morphological changes have already occurred 1). Acute corneal hydrops presents with sudden vision loss, photophobia, pain, and conjunctival injection.
Slit-lamp microscopy reveals thinning and anterior protrusion of the central corneal stroma. A practical technique involves rotating the observation system nearly 90 degrees toward the patient’s temporal side, which allows easier visualization of the conical corneal protrusion from a lateral perspective. In the early stage, even the contralateral eye that appears normal may show a characteristic pattern of focal steepening on corneal topography.
Early Findings
Irregular astigmatism: High-degree astigmatism that is non-orthogonal, with the sum of the principal meridians not equaling 180 degrees.
Scissor reflex: A scissor-like movement of the red reflex observed on retinoscopy.
Corneal thinning: Focal thinning is observed slightly inferior to the center, with the area of maximal thinning coinciding with the area of maximal steepening 1).
Fleischer ring: An annular iron deposition in the subepithelial layer at the base of the cone. It is clearly observed under a cobalt blue filter 1).
Vogt striae: Fine vertical striae observed in the mid to deep corneal stroma. They characteristically disappear temporarily with gentle digital pressure on the globe and reappear upon release 1).
Late Findings
Munson sign: A non-specific finding in which the lower eyelid protrudes conically forward on downward gaze 1).
Rizzuti sign: A focused beam of light appears at the nasal limbus via the cone apex when a slit beam is directed from the temporal side.
Corneal opacity: Reticular scarring at the apex due to Bowman layer rupture, and scarring of the mid to deep stroma.
Acute corneal hydrops: Aqueous humor flows into the corneal stroma through a rupture in the Descemet membrane, causing severe corneal edema and opacity.
Prominent corneal nerves: Corneal nerves are observed more prominently than usual due to thinning of the corneal stroma1).
In children and adolescents, progression is faster than in adults, and a higher proportion are already in the progressive stage at the time of diagnosis. Meyer et al. followed 148 eyes of children and adolescents for a mean of 2.9 years and found tomographic progression in 77.0% 3). Even in the subgroup aged under 16 years, 77.6% showed progression 3). In children, the cone also tends to form more centrally on the cornea. The pattern of bilateral progression is also characteristic: when at least one eye is severe (Amsler-Krumeich Stage III or IV), the rate of bilateral progression reaches 73.9%, significantly exceeding the 36.8% rate when both eyes are mild 3). A severe unilateral case should be regarded as a marker of potential progression in the fellow eye.
In progressive cases, when Kmax at the initial visit is 55 D or greater, the progression rate is significantly higher compared to cases with Kmax under 55 D (82% vs 62%, p=0.02) 3). In other words, the severity at the initial presentation itself serves as a predictor of future progression risk. On the other hand, multivariate analysis showed that age, sex, atopy, and reported eye rubbing were not independent predictors of progression 3). In a large systematic review and meta-analysis by Ferdi et al., natural history data from 11,529 eyes were aggregated, deepening the understanding of progression patterns in the absence of therapeutic intervention 13).
Keratoconus is a multifactorial disease involving a combination of genetic, biochemical, and biomechanical factors1). An autosomal dominant inheritance pattern with reduced penetrance is considered the best fit.
Regarding genetic background, polymorphisms in multiple genes including LOX (lysyl oxidase), CAST, VSX1, DOCK9, and TGFBI have been reported1). An FDA-approved genetic test evaluating over 2,000 variants across 75 genes is currently available1).
Eye rubbing and environmental factors
Accumulation of microtrauma: Mechanical stimulation from eye rubbing causes microtrauma to the corneal epithelium and stroma, increasing protease activity and promoting collagen degradation.
Involvement of allergic diseases: Ocular itching associated with hay fever, atopic dermatitis, bronchial asthma, vernal keratoconjunctivitis, and other conditions triggers eye rubbing1).
Sleeping position: Side-sleeping with the face pressed against the pillow can also act as continuous mechanical compression6).
Genetic predisposition
Family history: The CLEK study found a family history in 14% of cases1). The prevalence among first-degree relatives is clearly higher than in the general population.
Associated genes: Polymorphisms in LOX, CAST, VSX1, TGFBI, and others1).
Inheritance pattern: Autosomal dominant with reduced penetrance is considered the best fit1).
Associated systemic diseases
Chromosomal abnormalities: Down syndrome is the most strongly associated condition1).
Lifestyle-related: Obstructive sleep apnea syndrome, high BMI1).
Eye rubbing is the most important and modifiable environmental factor1, 6). In a discordant monozygotic twin case reported by Bitton et al., the affected twin had a strong eye rubbing habit and consistently slept in a left lateral position due to night shift work, whereas the unaffected twin had only mild eye rubbing and slept in a supine position6). This case, in which disease onset differed despite identical genetic backgrounds, demonstrates the decisive influence of environmental factors6).
QDoes eye rubbing cause keratoconus?
A
Eye rubbing is considered a critically important environmental factor in the onset and progression of keratoconus. However, genetic predisposition is also involved, and not everyone who rubs their eyes develops keratoconus. In studies of monozygotic twins, cases have been reported in which, among twins sharing the same genes but with different eye rubbing habits, only the twin with stronger eye rubbing developed keratoconus. Once diagnosed, patients are generally instructed to completely stop eye rubbing.
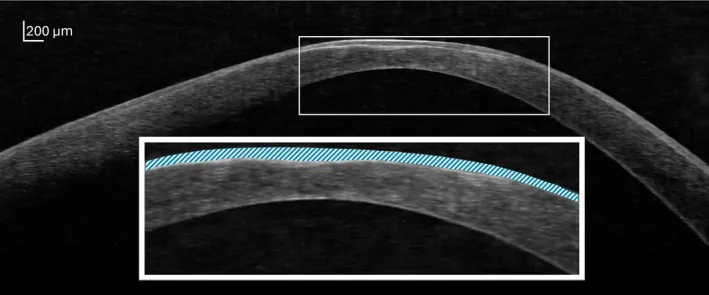
Gavin Swartz, Khyber Alam, Alex Gentle, Laura E Downie Impact of contact lens correction on wavefront aberrations and vision quality in keratoconus 2025 Oct 29 Ophthalmic Physiol Opt. 2025 Nov 29; 45(7):1811-1828 Figure 1. PMCID: PMC12682100. License: CC BY.
OCTB-scan image showing variability in corneal epithelial thickness in keratoconus. In the inset image magnifying the area outlined by the white border, the corneal epithelium is highlighted with light blue diagonal lines. In this region, the epithelium has thickened over the thinned corneal stroma, smoothing the contour of the anterior corneal surface. In contrast, the curvature of the posterior corneal surface is observed to be markedly steep.
The diagnosis of keratoconus is based on characteristic patient history, slit-lamp microscopy findings, and corneal topography and tomography findings1). Ideally, early diagnosis before the onset of subjective symptoms is desirable, but a cost-effective and simple screening method has not yet been established1).
Thin epithelium over the thinned area, with donut-shaped thickening around it
Wavefront aberration analysis
Higher-order aberrations
Marked increase in vertical coma aberration
Corneal biomechanical assessment
CH, CRF, CBI, TBI
Decreased biomechanical stiffness
Corneal topography/topometry: Comprehensive evaluation of the anterior and posterior surfaces is important for diagnosis1). An inferior/superior curvature ratio (I/S ratio) of ≥1.2 and a skew of the radial axis ≥21° are typical of keratoconus1). Posterior elevation mapping shows relatively high sensitivity and specificity, but has limitations in detecting forme fruste keratoconus1). The Klyce/Maeda method and the Smolek/Klyce method are widely used as keratoconus screening algorithms.
Anterior segment OCT: Provides high-resolution corneal cross-sectional images1). Corneal epithelial thickness mapping shows a donut-shaped pattern with thin epithelium over the area of stromal thinning and a rim of thickened epithelium around it1). Because epithelial remodeling partially masks anterior surface irregularities, posterior surface analysis is key to early diagnosis.
Corneal biomechanical assessment: Corneal hysteresis (CH), corneal resistance factor (CRF), and dynamic deformation analysis using Corvis ST are used8). The tomographic biomechanical index (TBI) and corneal biomechanical index (CBI), which combine corneal tomography and biomechanical assessment, are recommended as comprehensive screening indicators8). Biomechanical changes are believed to precede morphological changes, and their application to early detection is anticipated1).
IOP measurement considerations: Due to corneal thinning and biomechanical weakening, intraocular pressure is underestimated by Goldmann applanation tonometry1). The use of non-contact tonometry or dynamic contour tonometry (DCT) is recommended1).
According to the international consensus on the definition of progression (2015), progression is defined as changes in at least 2 of the following 3 items exceeding the measurement variability of the instrument9).
Steepening of the anterior corneal surface
Steepening of the posterior corneal surface
Decrease in corneal thickness, or increase in the rate of corneal thickness change from the periphery to the thinnest point
Meyer et al. calculated test-retest variability thresholds using the Orbscan tomographer in a pediatric and adolescent cohort and established the following thresholds for determining progression: Flat K +1.30 D, Steep K +1.88 D, Kmax +1.20 D, central K +0.87 D, anterior elevation +11.7 µm, posterior elevation +24.3 µm, central pachymetry −28.1 µm, and thinnest pachymetry −30.5 µm3). The distribution by severity according to the Amsler-Krumeich classification was Stage I 37.8%, Stage II 39.9%, Stage III 9.5%, and Stage IV 12.8%3).
The Amsler-Krumeich classification is a classic 4-stage severity classification that combines K value, refraction, pachymetry, and the presence or absence of corneal opacity. The newer ABCD classification (2016) independently evaluates four parameters: A: anterior corneal curvature radius, B: posterior corneal curvature radius, C: thinnest pachymetry, and D: best corrected visual acuity (BCVA)1). The mild/moderate/severe classification based on the CLEK study is also used in routine clinical practice.
Patients at high risk of rapid progression require closer follow-up. Shorter follow-up intervals are recommended for patients under 17 years of age and those with Kmax exceeding 55 D1). In clinical practice, follow-up intervals of 1 to 3 months for children and 6 to 12 months for adults are generally used as a guideline.
Pellucid marginal degeneration (PMD): Characterized by band-like thinning in the inferior peripheral cornea, with the thinned area located more peripherally than in keratoconus. Age of onset is also somewhat later, in the 30s to 50s.
Keratoglobus: A congenital condition in which the entire cornea is thinned in both eyes from birth, without Fleischer ring or Vogt striae.
Post-refractive surgery corneal ectasia (post-LASIK ectasia): May progress postoperatively in eyes with a predisposition to keratoconus, or result from corneal thinning due to excessive ablation.
Secondary keratoconus: Corneal thinning occurring during the scarring process of the primary disease such as herpes keratitis, accompanied by vascularization and scarring.
Contact lens-induced corneal warpage: Shows similar color-coded maps due to poor centration of rigid contact lenses (especially superior positioning), but is reversible without corneal thinning.
Corneal biomechanical assessment plays an important role in detecting keratoconus in early and questionable cases. Comprehensive preoperative screening combining corneal tomography and biomechanical assessment is recommended to avoid false negatives and improve diagnostic accuracy. 8)
The two mainstays of treatment are vision correction to maintain visual function and progression control to halt progression1). Mild irregular astigmatism can be managed with glasses or soft toric contact lenses, but as irregular astigmatism worsens, rigid contact lenses become necessary, and with further progression, interventions such as CXL, ICRS, and corneal transplantation are considered.
Glasses and contact lenses are the mainstay of treatment for most patients1). Mild cases can be managed with glasses or soft toric contact lenses, but as irregular astigmatism worsens, rigid gas-permeable (RGP) contact lenses become the first choice. Most patients achieve dramatic visual improvement with RGP lenses.
Fitting rigid contact lenses is technically more challenging than in normal myopia10), and determining the base curve from the measured corneal radius tends to result in a tight fit. The practical principle is to aim for good centration and movement rather than adhering strictly to the corneal curvature. In cases where spherical lenses are inadequate, multi-curve lenses may be considered.
In cases where rigid contact lens wear is difficult, specialty lenses such as scleral lenses, hybrid lenses, and the piggyback method (rigid lens over a soft lens) are selected1). Scleral lenses are worn on the sclera outside the limbus, causing less mechanical stimulation to the cornea and accommodating severe corneal irregularities; with their increasing popularity, they have been reported to contribute to a reduction in the rate of corneal transplantation1). More than 90% of patients are reported to maintain functional vision with some type of contact lens.
Corneal cross-linking for progressive keratoconus is a treatment that induces cross-links between corneal collagen fibers to enhance biomechanical stiffness, and is currently the first choice for progression control1, 2, 4). CXL halts or slows disease progression and reduces the future need for corneal transplantation1). In addition to corneal stabilization, CXL may induce 1.0–2.5 D of corneal flattening, potentially leading to visual improvement1). National data from the Netherlands reported a significant reduction in the number of corneal transplantations for keratoconus after the introduction of CXL12).
Remove the corneal epithelium over an 8–9 mm diameter
Instill 0.1% riboflavin ophthalmic solution (with 20% dextran) every 2 minutes for 30 minutes
Irradiate with UV-A (wavelength 365 nm) at 3 mW/cm² continuously for 30 minutes
Total energy dose is 5.4 J/cm²
After the procedure, wear a bandage contact lens to protect the cornea until epithelial regeneration is complete
Follow up with antibiotic and steroid eye drops postoperatively
Accelerated CXL: Developed to shorten the standard protocol time, using irradiation conditions such as 9 mW/cm² for 10 minutes or 18 mW/cm² for 5 minutes. Many comparative studies have shown equivalent efficacy to the standard protocol5). However, high-fluence conditions such as 30 mW/cm² for 3 minutes are considered less effective due to tissue oxygen depletion, and a pulsed irradiation method that replenishes oxygen has been developed5).
Transepithelial CXL (epi-on): A method of performing CXL while preserving the corneal epithelium, offering advantages such as reduced postoperative pain and lower infection risk. However, because riboflavin penetration is reduced, randomized controlled trials have shown a tendency toward inferior efficacy compared with the standard epi-off method, and some studies have reported worsening of Kmax5).
KERALINK trial was an observer-masked randomized controlled trial comparing CXL with standard treatment (glasses and contact lenses) in 60 eyes of patients aged 10–16 years with progressive keratoconus2). Cases with an increase of ≥1.5 D in K2 or Kmax over an interval of 3 months or more were enrolled as progressive cases, and eyes meeting the criteria of corneal apex thickness ≥400 µm and K2 ≤62 D were included2). The intervention was performed using the Avedro KXL device with irradiation of 10 mW/cm² for 9 minutes (total dose 5.4 J/cm²) and riboflavin eye drops2).
At 18 months, the adjusted mean difference in K2 was −3.0 D (95% CI −4.93 to −1.08 D, p=0.002), significantly lower in the CXL group2), and both uncorrected and corrected visual acuity (logMAR) were significantly better in the CXL group (both p=0.002)2). The odds of progression were 90% lower in the CXL group (OR 0.1, 95% CI 0.02–0.48, p=0.004), and the Cox proportional hazards model showed an 87% reduction in the hazard of progression over time in the CXL group2). No serious adverse events were observed2). CXL showed no interaction with atopic history or ethnicity, indicating efficacy in young patients from diverse backgrounds2). The US multicenter CXL trial also confirmed efficacy in adults4). Based on these results, CXL is recommended as first-line treatment for progressive cases in young patients2). The KERALINK results strongly support the current clinical practice of considering CXL promptly upon confirmation of progression.
Surgical intervention is considered when adequate vision cannot be achieved with contact lenses, or when contact lens wear becomes difficult1).
Intrastromal Treatment
Intracorneal ring segments (ICRS): Semi-arcuate synthetic segments such as Intacs, Ferrara, and Keraring are inserted into intrastromal tunnels created by femtosecond laser. Indications include mild to moderate cases with a clear central cornea and corneal thickness ≥400 µm at the insertion site1). They flatten the cornea, reduce irregular astigmatism, and facilitate contact lens wear.
CAIRS (Corneal Allogenic Intrastromal Ring Segments): Biological ring segments prepared from donor cornea, reported as a new alternative to synthetic rings. Safety and efficacy have been reported when combined with CXL.
Refractive Correction
Phakic intraocular lens (ICL): Toric ICL and iris-claw type (Artiflex) intraocular lens implantation have been reported as refractive correction options after shape stabilization with CXL5). Since corneal refractive surgeries such as LASIK are contraindicated, lens-based correction is an option.
Combined treatment: The Athens protocol combining topography-guided PRK with CXL, the Cretan protocol combining transepithelial PTK with CXL, and combined decentered individualized sphero-cylindrical (DISC) ablation with CXL have also been reported11).
Corneal Transplantation
Deep anterior lamellar keratoplasty (DALK): A procedure that replaces only the anterior corneal stroma while preserving the patient’s corneal endothelium. There is theoretically no risk of endothelial rejection, and the risk of traumatic rupture is lower than with PK. In cases without acute hydrops, DALK has recently tended to be chosen as the first-line option1).
Penetrating Keratoplasty (PK): It has a high success rate and long-term track record, and is established as a standard corneal transplantation procedure. There are risks of infection, rejection, and traumatic rupture, and irreversible postoperative mydriasis occasionally becomes a problem. Refractive correction with contact lenses is often still needed postoperatively.
Treatment of Acute Corneal Hydrops: For acute corneal hydrops due to Descemet membrane rupture, a pressure patch is worn for approximately one month, and acetazolamide (Diamox®) is administered orally as needed. Hypertonic saline eye drops (5% NaCl) and steroid eye drops may also be used to reduce edema. Once natural scarring occurs, contact lenses are prescribed anew. In recent years, intracameral air injection and amniotic membrane transplantation have also been reported as options. Post-hydrops scarring may involve the central cornea, but ironically, in some cases the scarring naturally reduces the corneal steepening; the refractive status after scar stabilization should be evaluated before determining the next treatment plan.
The cornerstone of progression prevention is complete cessation of eye rubbing1, 6). When allergic conjunctivitis or atopic conjunctival disease is the cause of ocular itching, symptoms should be adequately controlled with anti-allergy eye drops and antihistamines to reduce opportunities for eye rubbing. For severe ocular itching, systemic allergy management including antigen avoidance and skincare optimization should also be considered in addition to eye drops. Attention should also be paid to sleeping posture, and patients should be instructed to avoid side-sleeping positions that press the face against a pillow or arm6). It is effective to explain the pathology and importance of prevention not only to the patient but also to family members and caregivers, and to review the entire home environment for habits that trigger eye rubbing.
When a keratoconus patient develops cataract, corneal curvature instability and high irregular astigmatism make both intraocular lens power calculation and surgical manipulation difficult. It is recommended to stabilize the cornea with CXL or ICRS preoperatively, allow a contact lens-free period (at least 2 weeks for soft lenses and 5 weeks or more for rigid lenses), and confirm the stability of biometry before proceeding7). For IOL power calculation, standard formulas tend to cause postoperative hyperopic surprise; the use of keratoconus-specific formulas such as Barrett True-K and Kane keratoconus formula with a target of mild myopia is recommended7). Multifocal IOLs are not recommended due to increased higher-order aberrations7).
In terms of surgical technique, clear corneal incision in a thinned cornea carries a risk of wound leakage, so a sclerocorneal tunnel incision is recommended7). When corneal opacity reduces the visibility of capsulorhexis, anterior capsule staining with trypan blue and application of dispersive viscoelastic to the corneal surface are useful. In severe cases requiring corneal transplantation, triple surgery combining cataract surgery, IOL implantation, and corneal transplantation performed simultaneously is also an option.
QDoes corneal cross-linking hurt?
A
In the standard epi-off method, the corneal epithelium is removed, so pain, foreign body sensation, and tearing often occur for several days postoperatively. Pain is managed with a bandage contact lens, cooling, and analgesics. Epithelial regeneration is usually complete within 3 to 5 days, after which the pain subsides. In the epi-on method, the epithelium is not removed, so postoperative pain is reduced, but its efficacy may be inferior to the epi-off method.
QCan contact lenses be used with keratoconus?
A
Contact lenses play a central role in visual correction for keratoconus. Rigid gas permeable (RGP) lenses, which neutralize irregular astigmatism, are most commonly used and often provide dramatic visual improvement. When RGP lens wear is difficult, specialty lenses such as scleral lenses, hybrid lenses, and the piggyback method (rigid lens placed over a soft lens) can also be selected. Visual correction with some type of contact lens is reportedly possible in over 90% of cases.
QHow does keratoconus in children differ from that in adults?
A
Keratoconus in children and adolescents progresses faster than in adults. Corneal biomechanical rigidity increases with age, making pediatric corneas more susceptible to collagen degradation. In a study of 148 eyes of children and adolescents followed for a mean of 2.9 years, progression was observed in 77.0%, and the proportion already in the progressive stage at diagnosis was also high. While follow-up intervals for adults are 6 to 12 months, close follow-up every 1 to 3 months is recommended for children. When progression is confirmed, prompt corneal cross-linking is the only intervention that reduces the risk of corneal transplantation.
6. Pathophysiology and Detailed Mechanisms of Onset
In keratoconus, degradation of corneal collagen forms the basis of corneal thinning1). In the healthy corneal stroma, collagen fiber bundles composed predominantly of type I collagen are stacked three-dimensionally, maintaining corneal rigidity and shape. In the superficial layer adjacent to Bowman’s layer, the collagen fiber bundles are relatively narrow, steeply angled, and multidirectional, whereas in the deep layer, the fiber bundles become wider and flatter—a structural gradient. This steep, fine fiber bundle structure in the superficial layer contributes significantly to maintaining the anterior corneal shape, but in keratoconus, these structures are known to be altered.
At the molecular level, increased matrix metalloproteinases (MMPs) and decreased tissue inhibitors of metalloproteinases (TIMPs) are involved in collagen degradation of the corneal stroma1). Elevated concentrations of inflammatory mediators such as IL-6, TNF-α, and MMP-9 have been found in the tear fluid of keratoconus patients1). These inflammatory mediators induce apoptosis of corneal stromal cells (keratocytes), leading to a decrease in cell density1).
Keratoconus has traditionally been classified as a “non-inflammatory” corneal thinning disease, but recent studies have revealed the presence of inflammatory elements directly or indirectly involved in the development and progression of the pathology.1)
Histopathologically, Bowman’s layer shows rupture or loss, disorganization of collagen fiber alignment, scarring, and stromal thinning. In advanced cases, folds or rupture of Descemet’s membrane may also occur.
From a corneal biomechanical perspective, a localized decrease in elastic modulus is associated with collagen fiber collapse and degeneration8). Once localized rigidity loss occurs, stress concentrates and redistributes to the weakened area under the constant load of intraocular pressure, leading to corneal steepening and thinning—a “biomechanical failure cycle” has been proposed8).
In addition to genetic predisposition, repetitive mechanical stress such as eye rubbing is thought to trigger this biomechanical failure1, 6). The cornea in young individuals has a low collagen cross-link density, and rigidity increases with age, making the cornea of children and adolescents more susceptible to mechanical and enzymatic degradation1). This forms the biological basis for the faster progression observed in pediatric cases. Abnormalities in defense mechanisms against oxidative stress, particularly decreased superoxide dismutase activity and abnormalities in glutathione metabolism, have also been suggested to be involved in the pathology. These molecular pathways may form a vicious cycle that amplifies the production of inflammatory mediators and the activation of collagen-degrading enzymes.
Apoptosis of corneal stromal cells (keratocytes) is the direct cellular mechanism underlying the decrease in keratocyte density and stromal thinning in keratoconus1). Bowman’s layer is normally an extracellular matrix layer approximately 10 µm thick, but in keratoconus, rupture and loss are observed from the early stage, disrupting the anterior corneal shape-maintenance mechanism. Descemet’s membrane is a basement membrane that can be divided electron microscopically into an anterior banded layer and a posterior non-banded layer; when this membrane ruptures during acute hydrops, aqueous humor flows into the stroma, causing transient dramatic vision loss.
Early CXL in Children and Adolescents: The KERALINK trial demonstrated the efficacy of CXL for patients aged 10–16 years with high-level evidence2). The high progression rate of 77% in children and adolescents reported by Meyer et al. provides the rationale for early intervention before progression is confirmed3). If the long-term stabilizing effect of corneal cross-linking is sustained, it may eliminate the future need for regular contact lens wear or corneal transplantation2). The systematic review and meta-analysis by Ferdi et al. aggregated data from 11,529 eyes with natural history data, but pediatric data remain limited, and further accumulation of long-term follow-up is needed13).
Biomechanical Early Detection: Advances in corneal biomechanical assessment are enabling early detection at the “biomechanical stage,” preceding conventional morphological changes (corneal topography and tomography)1, 8). Establishing a comprehensive screening approach that combines corneal tomography with biomechanical assessment remains a future challenge8).
Genetic Screening: An FDA-approved genetic test evaluating 75 genes and over 2,000 variants is now available1). Early diagnostic approaches integrating environmental factors with genetic risk scores are still in the research phase and require further validation of clinical utility1).
Optimization of CXL Protocols: Active research is underway on optimizing accelerated protocols, improving oxygen supply through pulsed irradiation, and enhancing the permeability of the epi-on method5). Under high-fluence conditions, intra-tissue oxygen becomes depleted, reducing the efficiency of cross-linking reactions, and intermittent irradiation cessation (pulsed CXL) is being investigated as a method to replenish oxygen supply5). Combined treatments such as the Athens protocol (topography-guided PRK with CXL), the Cretan protocol (trans-epithelial PTK with CXL), and decentered individualized sphero-cylindrical (DISC) ablation with CXL have been reported as attempts to achieve both progression arrest and visual function improvement11). Since these combined treatments involve additional corneal tissue ablation, they are limited to cases with sufficient residual corneal thickness.
Long-term Stability Verification: Observational data spanning over 10 years are accumulating on the long-term stabilizing effect of CXL, with reports of sustained treatment efficacy, although some cases show gradual reprogression over time5). Future research challenges include determining the appropriateness of repeat CXL for reprogression, identifying predictors of reprogression, and developing more durable protocols. The widespread adoption of scleral lens technology is also expected to further reduce the number of cases requiring corneal transplantation1).
Jhanji V, Ahmad S, Amescua G, et al. Corneal Ectasia Preferred Practice Pattern. Ophthalmology. 2024 Apr;131(4):P205-P246. doi:10.1016/j.ophtha.2023.12.038. PMID:38349299.
Larkin DFP, Chowdhury K, Burr JM, Raynor M, Edwards M, Tuft SJ, Bunce C, Caverly E, Doré C, KERALINK Trial Study Group.. Effect of Corneal Cross-linking versus Standard Care on Keratoconus Progression in Young Patients: The KERALINK Randomized Controlled Trial. Ophthalmology. 2021;128(11):1516-1526. doi:10.1016/j.ophtha.2021.04.019. PMID:33892046.
Meyer JJ, Gokul A, Vellara HR, McGhee CNJ. Progression of keratoconus in children and adolescents. The British journal of ophthalmology. 2023;107(2):176-180. doi:10.1136/bjophthalmol-2020-316481. PMID:34479856.
Hersh PS, Stulting RD, Muller D, Durrie DS, Rajpal RK, United States Crosslinking Study Group. United States Multicenter Clinical Trial of Corneal Collagen Crosslinking for Keratoconus Treatment. Ophthalmology. 2017;124(9):1259-1270. doi:10.1016/j.ophtha.2017.03.052. PMID:28495149.
Lim L, Lim EWL. A Review of Corneal Collagen Cross-linking - Current Trends in Practice Applications. The open ophthalmology journal. 2018;12:181-213. doi:10.2174/1874364101812010181. PMID:30123383; PMCID:PMC6062907.
Bitton K, Dubois M, Moran S, Gatinel D. Discordant Keratoconus in Monozygotic Twins. Case reports in ophthalmology. 2022;13(1):313-317. doi:10.1159/000524116. PMID:35702523; PMCID:PMC9149403.
Findl O, Buehl W, Bauer P, et al. ESCRS Clinical Guidelines for Prevention and Treatment of Cataract. Vienna: European Society of Cataract & Refractive Surgeons; 2024.
AAO Refractive Management/Intervention PPP Panel. Evidence-Based Guidelines for Keratorefractive and Lens-Based Surgery. Ophthalmology. 2024.
Gomes JAP, Tan D, Rapuano CJ, Belin MW, Ambrosio R Jr, Guell JL, et al. Global consensus on keratoconus and ectatic diseases. Cornea. 2015;34(4):359-369. doi:10.1097/ICO.0000000000000408. PMID: 25738235.
Usgaonkar U, Chodankar S, Shetty A. Online survey about keratoconus management by optometrists. Indian journal of ophthalmology. 2023;71(1):86-90. doi:10.4103/ijo.IJO_525_22. PMID:36588214; PMCID:PMC10155547.
Knezović I, Djurić S. Decentered Individualized Sphero-Cylindrical (DISC) Ablation and Corneal Crosslinking in Patient with Progressive Keratoconus. Case reports in ophthalmological medicine. 2022;2022:1839848. doi:10.1155/2022/1839848. PMID:35912299; PMCID:PMC9334114.
Godefrooij DA, Gans R, Imhof SM, Wisse RP. Nationwide reduction in the number of corneal transplantations for keratoconus following the implementation of cross-linking. Acta ophthalmologica. 2016;94(7):675-678. doi:10.1111/aos.13095. PMID:27213687.
Ferdi AC, Nguyen V, Gore DM, Allan BD, Rozema JJ, Watson SL. Keratoconus Natural Progression: A Systematic Review and Meta-analysis of 11,529 Eyes. Ophthalmology. 2019;126(7):935-945. doi:10.1016/j.ophtha.2019.02.029. PMID:30858022.
Copy the article text and paste it into your preferred AI assistant.
Article copied to clipboard
Open an AI assistant below and paste the copied text into the chat box.