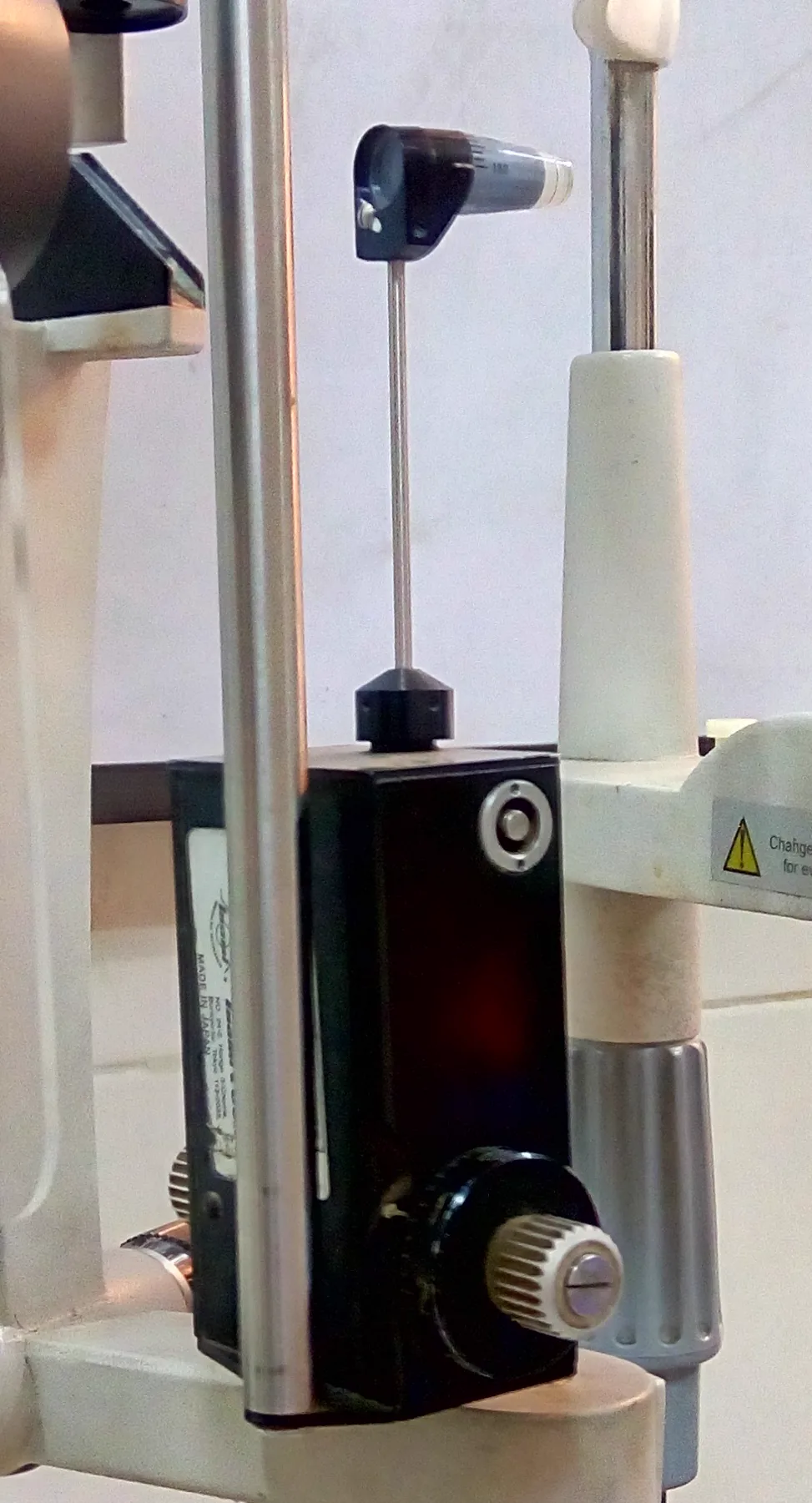
Actual photograph of a Goldmann applanation tonometer attached to the arm of a slit-lamp microscope, showing the measurement drum, applanation prism holder, and adjustment mechanism. This corresponds to the appearance of the slit-lamp-mounted contact tonometer discussed in the section “1. Goldmann Applanation Tonometer (GAT).”
The Goldmann applanation tonometer (GAT) is considered the most accurate and reproducible tonometer. GAT should be selected for cases requiring precise intraocular pressure measurement. It is a contact applanation tonometer used with a slit-lamp microscope and is positioned as the standard intraocular pressure measurement method in the 5th edition of the Glaucoma Clinical Practice Guidelines (recommendation level 1B)1).
The normal range of intraocular pressure (IOP) is 10–21 mmHg, based on Goldmann tonometry measurements1). If two or more measurements exceed 21 mmHg, further glaucoma evaluation (visual field test, OCT) is indicated1). Elevated IOP is the only proven modifiable risk factor for glaucoma, and myopia and corneal hysteresis have also been identified as high-evidence-level risk factors2).
The Ocular Hypertension Treatment Study (OHTS) showed that IOP-lowering treatment reduced the risk of progression to glaucoma from 9.5% to 4.4% over 5 years. This is a key evidence demonstrating the importance of IOP management2).
QWhy is the Goldmann tonometer the most trusted?
A
The basis is its theoretical design based on the Imbert-Fick law. By setting the applanated area to 15.09 mm² (diameter 3.06 mm), the surface tension of the tear film and the ocular rigidity of the cornea cancel each other out in nearly equal amounts. As a result, a simple relationship W = A × Pt holds between the applanation force W, the applanated area A, and the IOP Pt, allowing accurate IOP calculation. Due to decades of clinical experience and high reproducibility, it is used as the gold standard for evaluating all other tonometers.
The most accurate values are obtained at the design reference corneal thickness of 520 μm. The allowable error range is within ±1 mmHg for three repeated measurements, and the measurable range is 0–80 mmHg (drum scale range). In the presence of pulse variation, the midpoint of the semicircle moving with the heartbeat is taken as the measurement value.
When intraocular pressure exceeds the normal upper limit but both the optic nerve and visual field are normal, the condition is called ocular hypertension1). Thin CCT is associated with an increased risk of progression from ocular hypertension to glaucoma2). Even if GAT readings exceed 21 mmHg, in patients with thick CCT this may be an apparent high value, so judgment should be made in conjunction with CCT measurement.
When an infinitely thin sphere with no wall rigidity is flattened by a plane, the following relationship holds among the flattening force W, the flattened area A, and the internal pressure Pt of the sphere.
W = A × Pt
In the actual eye, in addition to the flattening force W applied to the cornea, the surface tension s of the tear film and the corneal resistance (ocular rigidity) b must be considered. However, by setting the flattened area to 15.09 mm² (diameter 3.06 mm), GAT makes s and b equivalent and cancel each other out. As a result, the design allows the Imbert-Fick law to be applied directly.
CCT is a parameter that affects the accuracy of many tonometers 2). An error of approximately 0.2 mmHg occurs per 10 μm of CCT. The following are sometimes used as correction guidelines.
CCT 500 μm → true IOP ≈ measured value + 1 mmHg
CCT 540 μm → true IOP ≈ measured value − 1 mmHg
However, the World Glaucoma Association IOP Consensus states that there is no generally accepted correction formula and that correction factors should not be applied to individual patient measurements 2). After corneal transplantation or LASIK, the physical properties of the cornea change, making correction more complex.
Corneal hysteresis provides independent information associated with the risk of primary open-angle glaucoma (POAG) 2).
QWhy are the semicircles of different thickness?
A
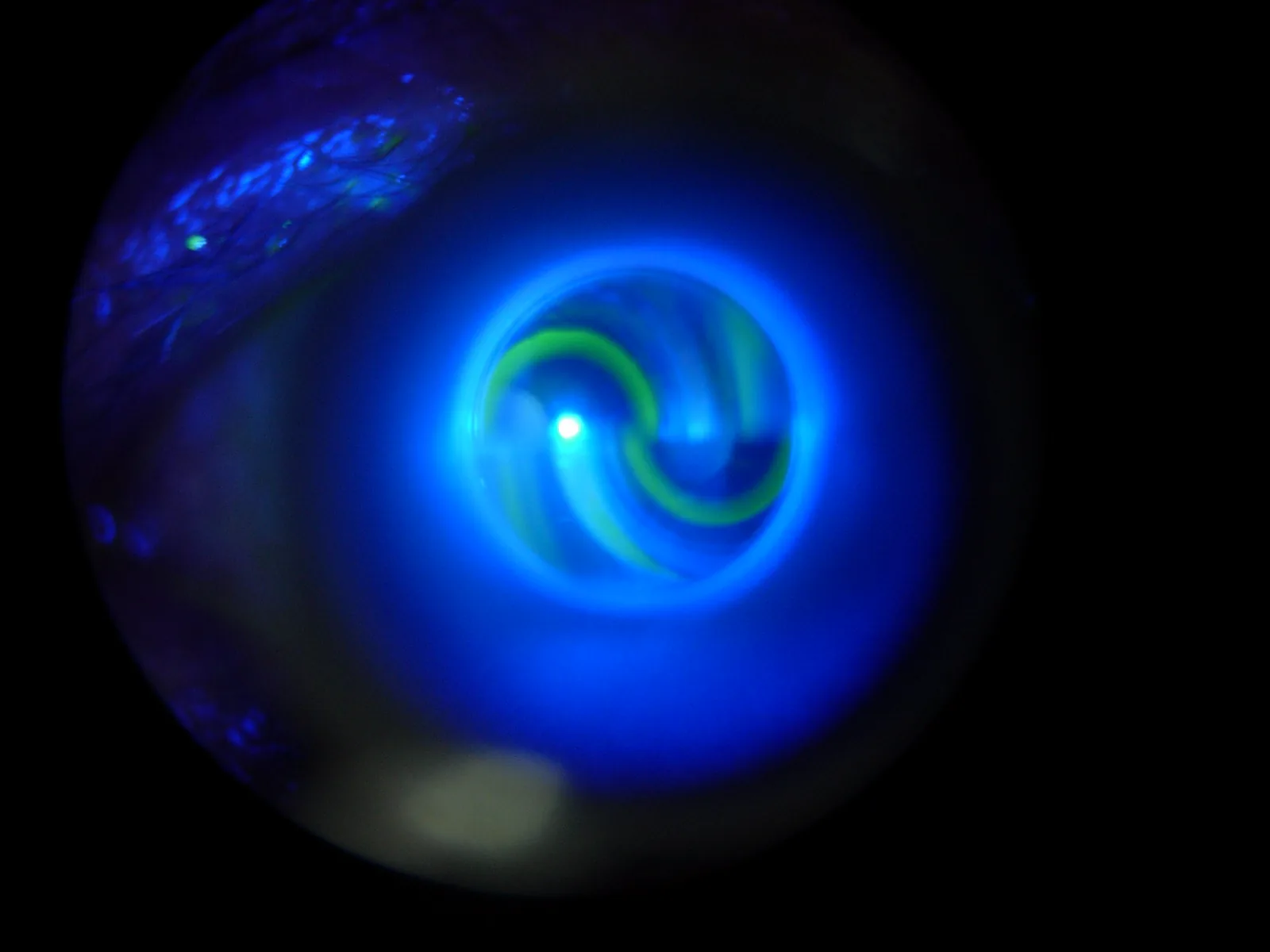
This is due to an excess or deficiency of fluorescein. The width of the semicircles observed through the applanation prism is approximately 0.2 mm with the appropriate amount. If staining is excessive, the width becomes thicker, leading to overestimation of intraocular pressure. If staining is insufficient, the width becomes thinner, leading to underestimation. When staining, it is important to adjust the amount appropriately using physiological saline or distilled water.
Manimury. Goldmann mires — semicircles seen during Goldmann tonometry through slit lamp. Wikimedia Commons. 2006. Figure 1. Source ID: commons.wikimedia.org/wiki/File:Goldmann_mires.jpg. License: Public Domain.
Under blue filter illumination of the slit lamp, two semicircular images (mires) are observed through the fluorescein-stained tear film, showing the upper and lower inner edges in contact (intraocular pressure reading point). This corresponds to the reading procedure by inner edge contact of the fluorescein semicircles described in the section “4. Examination Methods and Procedures.”
Preparation and Pretreatment
Attaching the applanation prism: Insert it into the support frame and align the scale at 0° or 180° with the white line.
If astigmatism is 3 D or more: Align the angle of the flattest meridian with the red line on the support frame.
Fluorescein staining: Adjust to an appropriate amount with physiological saline or distilled water and stain the ocular surface. Aim for a staining amount that results in a semicircle width of approximately 0.2 mm.
Measurement Procedure
Lighting settings: Insert a blue filter into the light source of the slit lamp microscope, open the slit width fully, and illuminate from a 60° angle.
Initial setting: Set the drum scale to 1 g (10 mmHg).
Corneal contact: Bring the tip of the applanation prism into contact with the central cornea. Two semicircles, upper and lower, are observed.
Reading: Adjust the position so that the upper and lower semicircles are the same size, rotate the drum until the inner edges touch, and read the value. Repeat three times and confirm that the error is within ±1 mmHg.
As a precaution during measurement, eyelid compression and Valsalva maneuver (straining) increase intraocular pressure, so instruct the patient to relax 2).
When using reusable prisms, sterilize with chemical disinfection (e.g., 3% hydrogen peroxide) or 70% isopropanol after each measurement. Using disposable prisms such as TonoSafe® (Haag-Streit) or TonoJet® (Luneau) can avoid the risk of cross-infection between patients. Disposable prisms are especially recommended for patients with infectious diseases such as herpes simplex or adenovirus.
Target intraocular pressure is set as the upper limit of IOP that sufficiently delays the progression of visual field deterioration to maintain the patient’s quality of life (QoL) 1)2). There is no uniform target value for all patients; it is set individually for each eye of each patient 1)2).
Criteria for Setting Target Intraocular Pressure
Early glaucoma: 18–20 mmHg, with a reduction of 20% or more from baseline as a guide 1).
Moderate glaucoma: 15–17 mmHg, with a reduction of 30% or more from baseline required 1).
Advanced glaucoma: A lower target intraocular pressure is needed.
Reassessment: The target intraocular pressure should be reviewed at each follow-up visit. Adjust it when progression is confirmed or when new systemic diseases develop 1)2).
Factors Influencing Target Intraocular Pressure
Age: Younger patients have longer life expectancy and need lower targets, but older patients also have a higher risk of progression 1).
Central corneal thickness: Thin CCT is a risk factor. It provides a basis for setting a lower target 2).
Rate of progression: The faster the progression, the lower the target IOP should be set1).
IOP-independent factors: Attention should also be paid to factors other than IOP, such as circulatory disorders and pseudoexfoliation1).
The extent of initial visual field damage is the most important predictor of blindness from glaucoma1). At the time of new diagnosis, the rate of progression is unknown, so the target IOP is set based on risk factors, and after 2–3 years of follow-up, it is readjusted based on the rate of progression1). The same tonometer should be used for follow-up of the same patient2).
QWhat if glaucoma progresses despite reaching the target IOP?
A
If progression is confirmed despite reaching the target IOP, the target value should be set even lower and the treatment plan reviewed. Discuss with the patient and weigh the risks and benefits of additional interventions. Conversely, if the target is not reached but the condition is stable, the target value may be adjusted upward. The target IOP is not fixed; it is a concept that is dynamically reassessed over time. Also evaluate the possibility that IOP-independent factors (e.g., circulatory disorders) are involved in progression1).
After refractive surgery (0.3–0.4 mmHg lower per 10 μm of LASIK ablation)2)
Winter/seasonal variation1)
After exercise/alcohol consumption
Eyelid compression/Valsalva maneuver2)
General anesthesia
Diurnal variation can reach 4–5 mmHg even in healthy individuals. In glaucoma patients, the variation is even larger, so measurements at multiple times and on multiple occasions improve diagnostic accuracy.
After refractive surgery (RK, PRK, LASIK), intraocular pressure is measured lower than actual. The main causes are corneal flattening and central corneal thinning. Even if the measured pressure appears “normal,” glaucoma may still progress, requiring careful visual field and OCT monitoring2).
In cases of corneal irregularity or scarring, or after corneal transplantation, measurement accuracy decreases. Inter- and intra-observer variability also exists, so for follow-up of the same patient, it is desirable to use the same examiner and the same tonometer2).
Pascal Dynamic Contour Tonometer (DCT): Measures dynamic pulsatile fluctuations in intraocular pressure using a piezoelectric sensor. It is said to be less affected by CCT and corneal curvature, and can also measure ocular pulse amplitude.
Standardization of disposable prisms: With the spread of Tonosafe® and Tonojet®, infection control measures in contact tonometry are becoming standardized.
24-hour intraocular pressure monitoring: A soft contact lens sensor (CLS) that records changes in corneal curvature has been approved in Europe. Efforts are underway to understand intraocular pressure fluctuations including nighttime and during sleep.
Gedde SJ, Vinod K, Wright MM, et al. Primary Open-Angle Glaucoma Preferred Practice Pattern. Ophthalmology. 2021 Jan;128(1):P71-P150. doi:10.1016/j.ophtha.2020.10.022. PMID:34933745.
Shahid A, Patel K, Kingra RK, Rozwat AS, Roberts DK. Even-number measurement bias with Goldmann applanation tonometry in patients with glaucoma and glaucoma suspects. Clin Exp Optom. 2024;107(2):192-195. PMID: 38207086.
Copy the article text and paste it into your preferred AI assistant.
Article copied to clipboard
Open an AI assistant below and paste the copied text into the chat box.