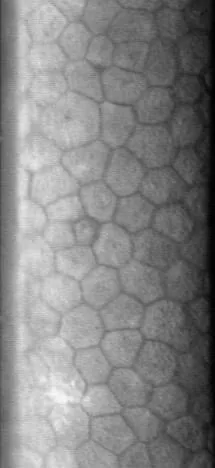
Specular reflection image of the corneal endothelial cell layer captured with a specular microscope. Normal endothelial cells form a regular hexagonal mosaic pattern, with cell boundaries appearing as dark lines. This corresponds to the visualization of endothelial cells using the specular reflection method discussed in the section “1. What is corneal endothelial cell examination?”
Corneal endothelial cell examination (specular microscopy) is a test that uses the principle of specular reflection to photograph and analyze corneal endothelial cells. It can non-invasively quantify cell density, morphology, and size variation.
Corneal endothelial cells are a monolayer on the posterior surface of the cornea, maintaining corneal transparency through pump and barrier functions. However, directly quantifying these functions is difficult. Therefore, endothelial function is typically assessed by parameterizing changes in morphology. Although qualitative evaluation of endothelial cells is possible with slit-lamp specular reflection, specular microscopy enables numerical quantification of morphological parameters.
Main indications:
Before cataract surgery: Evaluation of endothelial cell density (covered by insurance). Provides basis for surgical planning and patient explanation.
Before and after corneal endothelial transplantation (DSAEK/DMEK): Preoperative evaluation and postoperative longitudinal monitoring of endothelial density.
Fuchs endothelial corneal dystrophy and ICE syndrome: Detection of guttata and regular monitoring of density decline.
Long-term contact lens wearers: Assessment of endothelial changes due to chronic hypoxia.
QWhat is the role of corneal endothelial cells?
A
Corneal endothelial cells maintain corneal transparency through pump and barrier functions. The corneal stroma has a swelling pressure of about 50 mmHg, but in normal eyes, the endothelial pump overcomes this to remove excess water from the cornea. Endothelial cells have almost no regenerative capacity, so when damaged, remaining cells enlarge and flatten to compensate. However, if density decreases significantly, decompensation occurs, leading to corneal edema.
There are three main types of specular microscopes based on measurement principle and contact method.
Non-contact type
Features: Currently the mainstream type in clinical practice. No need for topical anesthesia and supports auto-alignment.
Advantages: Low patient burden, no infection risk, and allows repeated measurements in a short time.
Limitations: The imaging range is somewhat limited. Accurate imaging becomes difficult in cases of severe corneal edema or opacity.
Contact Type
Features: A method in which the lens is brought into direct contact with the cornea for imaging. Topical anesthesia (0.4% oxybuprocaine) is required.
Advantages: Allows wider and clearer imaging than the non-contact type. Reliable results can be obtained even in cases of corneal edema or opacity. In healthy eyes and post-transplant corneas, cell density measurements from contact and non-contact types are reported to be generally equivalent [4].
Limitations: Topical anesthesia is required. Skilled technique is necessary.
Confocal Microscope
Features: A special device that allows tomographic observation of each layer of the cornea.
Advantages: Enables three-dimensional evaluation of not only the endothelium but also the epithelium, stroma, and cells in each layer. It can also be used to observe the nerve plexus.
Limitations: The operation is more complex and the examination time is longer compared to a standard specular microscope. A dedicated machine is required.
For non-contact type: Topical anesthesia is not required. Fix the head with a chin rest and forehead strap, and have the patient look straight at the fixation light. Automatic alignment and imaging are performed.
For contact type: Perform topical anesthesia with 0.4% oxybuprocaine hydrochloride eye drops. The examiner brings the lens into contact with the cornea and captures images.
Automatic analysis: After imaging, the device automatically outputs cell density (CD), coefficient of variation (CV), and hexagonality (percentage of hexagonal cells).
Manual correction: If the accuracy of automatic analysis is low, manually correct the boundaries and recalculate using manual analysis.
Simultaneous CCT measurement: Many models support simultaneous measurement of central corneal thickness (CCT).
If the number of cells used for analysis is too small, the reliability of the examination decreases. Doughty et al. reported that with a non-contact specular microscope, the coefficient of variation is about ±10% when analyzing 25 cells, but converges to about ±2% when analyzing 75 or more cells [2]. Analysis by Abib et al. also indicates that although the required sample size varies by device, several hundred cells are desirable in all cases [3]. Always check the number of cells automatically recognized by the analysis software.
In cases with corneal edema or opacity, accurate imaging is difficult, and the reliability of the analysis results is low. In such cases, attempt imaging again in an area with higher transparency. Using a contact-type specular microscope allows wider and clearer imaging and is therefore useful.
QIs corneal endothelial cell examination painful?
A
With the non-contact type, no topical anesthesia is required, and although you may feel glare, there is basically no pain. With the contact type, topical anesthesia with 0.4% oxybuprocaine eye drops is applied before contacting the lens, so pain is less likely while the anesthesia is effective. Both examinations are completed in a short time.
Cell density is a central indicator for endothelial evaluation. Multiple studies have shown that it physiologically decreases with age [1][6], roughly following the trend below.
Newborns: 3,500–4,000 cells/mm²
20s: approximately 2,700 cells/mm²
70 years or older: average 2,200 cells/mm²
Normal annual decrease rate: 0.5%/year
After cataract surgery: 2%/year (accelerated decrease)
After glaucoma surgery: 10%/year (further acceleration)
When cell density falls below 400–500 cells/mm², it becomes impossible to maintain corneal transparency, leading to bullous keratopathy.
The CV value is the coefficient of variation, calculated by dividing the standard deviation of cell area by the mean cell area, and indicates anisocytosis (variation in cell size). An increase suggests greater cell stress. The normal range is 0.2–0.3, and a value of 0.35 or higher is considered abnormal.
Normal corneal endothelial cells are arranged in a regular hexagonal pattern. A decrease in the percentage of hexagonal cells indicates greater disruption of cell morphology. The normal range is 60–70%, and a value of 50% or lower is considered abnormal.
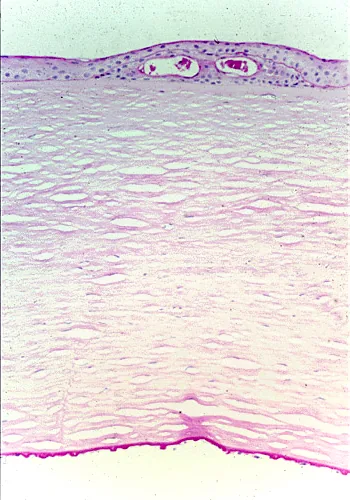
Specular Findings in Fuchs Endothelial Corneal Dystrophy
Light micrograph of PAS-stained Fuchs endothelial corneal dystrophy. Numerous guttata protrude from the posterior surface of Descemet’s membrane, accompanied by epithelial cysts and basement membrane displacement. This corresponds to the guttata formation and dark areas on specular microscopy discussed in section “4. Interpretation of Results and Normal Values” for Fuchs endothelial corneal dystrophy.
In Fuchs endothelial corneal dystrophy, the following characteristic findings are observed with a specular microscope:
Guttata (corneal guttae): Elevated areas of the endothelium (Descemet’s wart-like thickening) appear as dark circular regions (dark areas).
Decreased cell density: The endothelial cell density is apparently lower because the area occupied by guttata is excluded from measurement.
Increased CV and decreased hexagonality: Endothelial cells become deformed and enlarged to compensate for the defects, worsening morphological indices.
QWhat is a safe corneal endothelial cell density before cataract surgery?
A
There is no clear universal standard, and it varies among institutions. Generally, a CD below 1,000 cells/mm² is considered high risk for surgery. It requires careful selection of surgical technique (e.g., reducing ultrasound time in phacoemulsification, using additional viscoelastic agents) and thorough informed consent with the patient. If CD drops to 400–500 cells/mm² or lower, there is a risk of bullous keratopathy after surgery, and combined cataract surgery with corneal endothelial transplantation (DSAEK/DMEK) may be considered.
Based on abnormal test results, consider the following management strategies.
CD < 1,000 cells/mm² (before cataract surgery):
This indicates a high surgical risk. Adjust the surgical technique by shortening ultrasound time and selecting appropriate viscoelastic materials, and fully explain the risks to the patient. Since criteria vary by facility, the attending physician’s comprehensive judgment is important.
CD < 400–500 cells/mm²:
The risk of bullous keratopathy is imminent. Actively consider corneal endothelial transplantation (DSAEK/DMEK). Compared to penetrating keratoplasty (PKP), DSAEK/DMEK has higher endothelial cell survival rates and faster visual recovery.
CV > 0.35 or Hexagonality < 50%:
Indicates endothelial stress. Investigate causes such as Fuchs endothelial corneal dystrophy, ICE syndrome, long-term contact lens wear, or history of intraocular surgery.
Postoperative follow-up:
After cataract surgery, check endothelial density at 1–3 months and 1 year postoperatively. Endothelial cell loss is greatest in the first year and then gradually progresses over several years. Preoperative endothelial density, age, and ultrasound time have been identified as independent risk factors [5].
After corneal endothelial transplantation (DSAEK/DMEK), continue endothelial density monitoring every 6 months to 1 year.
The specular microscope uses specular reflection of light to visualize endothelial cells. When illumination light is directed at the interface between the corneal stroma and aqueous humor (endothelial cell layer), some light is reflected at the boundary of media with different refractive indices. By receiving this reflected light, an image of the endothelial cells is obtained.
At cell boundaries (intercellular spaces), reflection is weak and appears dark (dark line), while the cell body appears bright. This outlines the cells. The captured cell image is automatically recognized and quantified by image analysis software to calculate CD, CV, and Hexagonality.
The corneal stroma always has a swelling pressure (SP) of about 50 mmHg. In normal eyes, the corneal endothelial pump actively transports Na⁺ and HCO₃⁻ to the aqueous humor side, overcoming this swelling pressure to maintain the cornea at physiological thickness and transparency.
When endothelial cell density drops below 500 cells/mm², the pump function of the remaining endothelial cells becomes insufficient. Water exceeding the swelling pressure of the corneal stroma flows in, leading to stromal edema and formation of subepithelial bullae. This is bullous keratopathy. Rupture of bullae causes severe pain and loss of the ocular surface barrier function.
Conventional automated analysis software has had challenges in recognition accuracy, especially in areas with low cell density or in cases of edema. In recent years, research on automated cell boundary recognition using machine learning and deep learning has progressed. Good correlation with manual analysis has been reported, and future clinical implementation is expected.
Basic research has shown that Rho-associated kinase (ROCK) inhibitors promote adhesion and proliferation of corneal endothelial cells. In Japan, clinical development of ROCK inhibitor eye drops (Y-27632 derivative) aimed at promoting corneal endothelial cell proliferation is underway. Application to bullous keratopathy and recovery of endothelial density after corneal endothelial transplantation is attracting attention as a research stage, but at present it has not reached widespread use in general practice.
Endothelial Changes in Long-Term Contact Lens Wearers
Long-term contact lens wear (especially hard lenses) has been reported to cause increased polymegethism (variation in cell size) and pleomorphism (increase in non-hexagonal cell shapes) due to chronic corneal oxygen deprivation. This appears as an increase in CV value and decrease in hexagonality, but cell density itself often remains within the normal range.
Corneal endothelial damage has been reported with long-term use of amantadine (a Parkinson’s disease medication) and some antipsychotic drugs. It may be detectable as decreased cell density and morphological changes on specular microscopy, and the usefulness of regular monitoring in patients receiving these drugs is being studied.
Sanchis-Gimeno JA, Lleó-Pérez A, Alonso L, Rahhal MS, Martínez Soriano F. Corneal endothelial cell density decreases with age in emmetropic eyes. Histol Histopathol. 2005;20(2):423-427. PMID: 15736046. https://pubmed.ncbi.nlm.nih.gov/15736046/
Doughty MJ, Müller A, Zaman ML. Assessment of the reliability of human corneal endothelial cell-density estimates using a noncontact specular microscope. Cornea. 2000;19(2):148-158. PMID: 10746445. https://pubmed.ncbi.nlm.nih.gov/10746445/
Abib FC, Holzchuh R, Schaefer A, Schaefer T, Godois R. The endothelial sample size analysis in corneal specular microscopy clinical examinations. Cornea. 2012;31(5):546-550. PMID: 22333658. https://pubmed.ncbi.nlm.nih.gov/22333658/
Módis L Jr, Langenbucher A, Seitz B. Corneal endothelial cell density and pachymetry measured by contact and noncontact specular microscopy. J Cataract Refract Surg. 2002;28(10):1763-1769. PMID: 12388025. https://pubmed.ncbi.nlm.nih.gov/12388025/
Lee NS, Ong K. Risk factors for corneal endothelial cell loss after phacoemulsification. Taiwan J Ophthalmol. 2024;14(1):83-87. PMID: 38654985; PMCID: PMC11034697. https://pmc.ncbi.nlm.nih.gov/articles/PMC11034697/
Chaurasia S, Vanathi M. Specular microscopy in clinical practice. Indian J Ophthalmol. 2021 Mar;69(3):517-524. doi:10.4103/ijo.IJO_574_20. PMID:33595465; PMCID:PMC7942069.
Copy the article text and paste it into your preferred AI assistant.
Article copied to clipboard
Open an AI assistant below and paste the copied text into the chat box.

{kind=link}
{kind=link}