Descemet membrane endothelial keratoplasty (DMEK) is a type of corneal endothelial transplant performed for corneal endothelial dysfunction. It was first reported by Melles et al. in 20061). Only the Descemet membrane and corneal endothelial cell layer are separated from the donor cornea, and the recipient’s diseased Descemet membrane is removed. The graft is attached to the posterior corneal surface using gas tamponade. The graft thickness is approximately 15 μm, which is extremely thin compared to DSAEK (approximately 50–150 μm), which includes stroma1).
DMEK: Transplant includes only Descemet membrane + endothelium
Hyperopic shift: Smaller with DMEK1)
Rejection: DMEK has a lower frequency 1)
Corneal endothelial transplantation has two major surgical methods: DSAEK and DMEK. DMEK does not include stroma, so it is optically superior, induces minimal astigmatism, and is said to rarely cause rejection. On the other hand, intraoperative graft manipulation is difficult, and the risk of graft detachment is higher than DSAEK1).
Advantages of DMEK include lower technical equipment requirements and potential cost savings compared to DSAEK, as well as the possibility of split cornea transplantation (using one donor cornea for two patients: DMEK and DALK) 1).
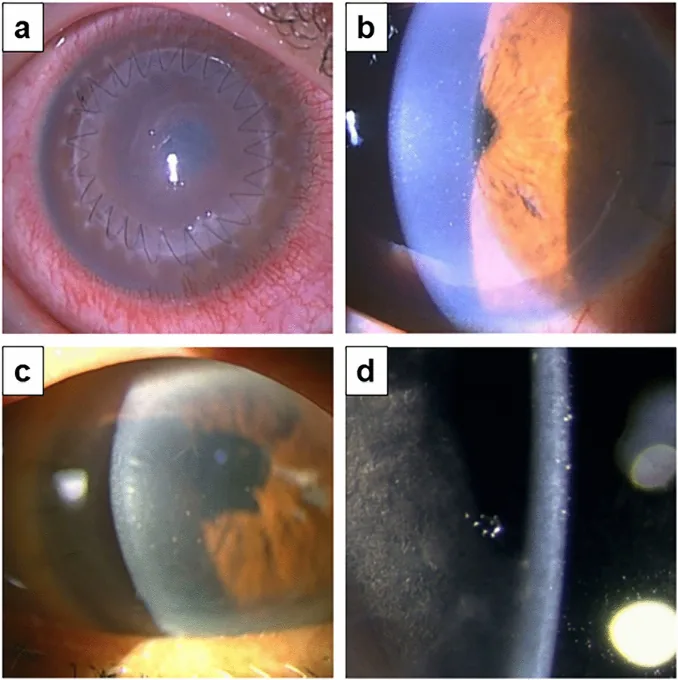
Haguku Wajima, Takahiko Hayashi, Akira Kobayashi, Tsubasa Nishino, et al. Graft rejection episodes after keratoplasty in Japanese eyes 2023 Feb 14 Sci Rep. 2023 Feb 14; 13:2635 Figure 1. PMCID: PMC9929100. License: CC BY.
a shows an overall view of the postoperative eye with sutures, showing diffuse corneal opacity. b and c are slit-lamp images from the side showing opacity on the posterior side, and d magnifies fine deposits.
The main indication for DMEK is corneal endothelial dysfunction.
Fuchs endothelial corneal dystrophy (FECD): The most common indication. It is the most frequent corneal endothelial dystrophy worldwide, usually developing in the 50s to 60s 8). More common in women (male:female ratio 1:3–4). Severity is assessed using the Krachmer classification 8)
Grade 0–1: Scattered or non-confluent guttae. Corneal transparency is maintained.
Grade 2–3: Confluent guttae in the central 1–5 mm. Beaten-metal appearance.
Grade 4: Confluent guttae exceeding 5 mm centrally. Stromal edema and epithelial bullae formation.
If there is scarring in the corneal stroma, DMEK may leave opacity or irregular astigmatism, so full-thickness corneal transplantation should be considered. In principle, pseudophakic eyes are preferable.
Scheimpflug tomography is useful for determining surgical indications for FECD. The following three findings strongly predict progression of FECD and the need for corneal transplantation 8).
Irregularity of isopachs within the central 4 mm
Displacement of the thinnest point (usually toward the nose)
Localized depression of the posterior corneal surface
When all three findings are present, the 5-year progression rate is approximately 90%; when none are present, it is approximately 7%. For patients with corneal thickness ≤640 μm, the probability of not requiring corneal transplantation within 1 year after cataract surgery is 95% 8).
DMEK is also effective for early-onset Fuchs endothelial corneal dystrophy associated with the COL8A2 gene mutation (p.Leu450Trp), with reports achieving good visual acuity of 20/20 to 20/30 in all eyes 7). Despite long-term corneal edema, the cornea can become clear after surgery 7).
DMEK is superior in terms of speed of visual recovery and final visual acuity. However, in eyes with aniridia, extensive anterior synechiae, after vitrectomy, or with poor anterior chamber visibility, DSAEK can be performed more safely. If there is severe corneal stromal scarring, visual improvement is limited with either endothelial transplant, so full-thickness corneal transplantation should be considered.
The SCUBA method (submerged cornea using backgrounds away technique) is widely used. With the endothelial side of the donor corneoscleral button facing up, a shallow 360° incision is made in the Descemet membrane inside the Schlemm’s canal using a crescent knife or golf knife 1). The inner part is slowly lifted with non-toothed forceps to peel off the Descemet membrane. The peeled Descemet membrane forms a scroll with the endothelial cells on the outside.
Stain with 0.06% trypan blue, cut into a circular shape of appropriate diameter for the patient using a trephine, and set in a Jones tube. Marking the stromal side of the Descemet membrane with “S” or “F” using trypan blue reduces the risk of misidentifying the graft orientation in the anterior chamber.
Retrobulbar or Tenon’s capsule anesthesia is used. In cases where high vitreous pressure is expected, preoperative intraocular pressure is lowered with a Honan balloon.
Since FECD and cataract often occur at similar ages, the following three strategies are selected based on the corneal condition 8).
Cataract surgery first: For mild FECD (Krachmer grade 1-2) where cataract is the main cause of visual loss. However, in grades 2.5-4, about 20% of cases require corneal endothelial transplantation postoperatively.
DMEK first: When corneal edema is the main cause and cataract is mild. Postoperative steroid use may worsen cataract.
Simultaneous surgery (Triple-DMEK): Considered when corneal thickness is ≥640 μm, endothelial cell density <1,000 cells/mm², and morning foggy vision is present.
Soft-shell technique: Coat the corneal endothelium with a dispersive OVD and maintain the anterior chamber with a cohesive OVD. Useful for endothelial protection during phacoemulsification
Under BSS (balanced salt solution) or air perfusion, use an inverted Sinskey hook to create a circular descemetorhexis in the recipient cornea. The diameter is typically around 8.0 mm.
Graft Insertion
Insertion device: Jones tube (glass tube) or glass injector
Incision width: 2.2–2.4 mm is sufficient
Pre-placed suture: Place a 10-0 nylon suture for rapid closure after insertion
Procedure: Flush the graft into the anterior chamber with the stromal side up using a fluid stream
Unfolding and Gas Injection
Unfolding maneuver: Alternate between tapping the corneal surface and BSS injection/aspiration1)
Orientation check: Confirm with intraoperative OCT or S/F mark
Gas tamponade: Injection of 20% SF6 gas or air
Postoperative positioning: Maintain supine position for 30–60 minutes
After graft insertion, remove a small amount of aqueous humor from the side port to induce hypotony and prevent graft extrusion. Close the corneal incision with 10-0 nylon. Peripheral iridectomy is usually performed after graft unfolding and gas injection.
Graft detachment and rebubbling: This is the most frequent complication of DMEK. Graft detachment is more common in DMEK than in DSAEK1). A meta-analysis showed that the odds ratio for rebubbling (repeat gas injection) was 2.76 (95% CI 1.46–5.22), significantly higher in DMEK2). When graft detachment occurs, early rebubbling often achieves reattachment.
Postoperative intraocular pressure elevation: Occurs in 20–30% of patients after corneal endothelial transplantation. It is important to differentiate between steroid-induced glaucoma and secondary glaucoma due to postoperative inflammation. Evaluate for anterior synechiae using anterior segment OCT.
Rejection: The rejection rate after DMEK is approximately 1%, lower than after DSAEK (5–10%). The 5-year rejection episode rate has been reported as 2.6%6). Unlike full-thickness corneal transplantation, rejection after corneal endothelial transplantation often resolves with steroid eye drops alone.
COVID-19 vaccine-related rejection: There is a report of bilateral DMEK rejection after BNT162b2 mRNA vaccination6). A 94-year-old woman developed bilateral graft rejection 2 weeks after vaccination, ultimately requiring re-DMEK6). Increased steroid eye drops before and after vaccination are recommended6).
Cystoid macular edema (CME): Occurs in approximately 10–13.8% of cases after DMEK4). Frequent steroid eye drops are effective for prevention, but secondary CME associated with herpes virus reactivation has also been reported4).
Herpes virus reactivation and recurrent graft failure: A case of recurrent graft failure after DMEK for FECD has been reported, in which anterior chamber PCR was positive for herpes simplex virus-14). When recurrent DMEK failure without technical cause, corneal edema in both host and graft, and mild anterior chamber reaction with elevated intraocular pressure are observed, herpetic uveitis should be considered in the differential diagnosis4).
Intraoperative anterior chamber fibrin reaction: Spontaneous intraoperative fibrin formation can occur in approximately 3.7% of DMEK cases 5). Fibrin fibers derived from the iris can impede graft unfolding, leading to graft failure in 80% of cases 5). Chronic breakdown of the blood-aqueous barrier (BAB) is thought to be the underlying cause 5). In advanced FECD, elevated cytokine levels in the anterior chamber have been reported, and minor iris trauma can trigger fibrin formation 5). Preoperative NSAID eye drops, intraoperative triamcinolone acetonide, and r-TPA (recombinant tissue plasminogen activator) have been proposed for prevention 5).
Postoperative corneal thickness improvement and graft adhesion are checked every 2–3 days using anterior segment OCT. Even if the graft appears adherent, if edema does not improve, graft detachment may occur later.
Frequent steroid eye drops (loteprednol or dexamethasone) are started and gradually tapered. Slow tapering is very important to prevent rejection. Graft infection is rare but often donor-derived. If Candida or other organisms are detected in corneal storage medium culture, antifungal eye drops are prescribed.
QWhat happens if graft detachment occurs?
A
Graft detachment is a relatively common complication after DMEK. If detected early, most cases can be reattached by rebubbling (reinjection of air into the anterior chamber). If complete detachment makes reattachment difficult, repeat DMEK may be necessary. Partial detachment may spontaneously reattach with observation.
In a multicenter randomized controlled trial by Dunker et al. (54 eyes), the mean best-corrected visual acuity (BCVA) (logMAR) at 12 months postoperatively was 0.08 in the DMEK group vs 0.15 in the UT-DSAEK group, with no significant difference 3). However, the proportion achieving BCVA of 20/25 or better was significantly higher in the DMEK group (66% vs 33%, P=0.02) 3). Endothelial cell density (ECD) at 12 months showed no significant difference between groups (DMEK 1870 cells/mm² vs UT-DSAEK 1612 cells/mm²) 3).
In a meta-analysis by Sela et al. (8 studies, 376 eyes), the best corrected visual acuity at 12 months was significantly better in the DMEK group (mean difference −0.06 logMAR; 95% CI −0.10 to −0.02)2). However, the rebubbling rate was significantly higher in the DMEK group (OR 2.76; 95% CI 1.46-5.22), highlighting the importance of appropriate patient selection2). With ultrathin DSAEK grafts less than 70 μm, no significant difference in best corrected visual acuity was observed2).
Both procedures induce a mild hyperopic shift, but the shift is smaller with DMEK (DMEK +0.22D vs UT-DSAEK +0.58D)3). Five-year graft survival rates and endothelial cell loss rates are reported to be comparable between the two procedures1).
DMEK was performed in 4 eyes (2 patients) with early-onset Fuchs endothelial corneal dystrophy due to a COL8A2 gene mutation (p.Leu450Trp)7). The mean preoperative central corneal thickness (CCT) decreased from 713 μm to 529 μm at 1 month postoperatively, and all eyes achieved a best corrected visual acuity of 20/20 to 20/307). However, refractive fluctuations of 3 to 3.6 D were observed during the first postoperative year, indicating that refractive stabilization may take longer in patients with COL8A2 mutations7).
QHow much vision improvement can be expected with DMEK?
A
Many patients achieve a best corrected visual acuity of 20/25 (0.8) or better within 12 months after surgery. In a multicenter RCT, 66% of eyes achieved 20/25 or better. However, recovery may be limited if there are irreversible changes such as corneal stromal scarring or long-standing edema.
Normal corneal endothelial cells pump water from the corneal stroma into the anterior chamber via Na⁺/K⁺-ATPase pumps, maintaining corneal hydration at approximately 78%. In FECD and PBK, this pump function fails, leading to excessive fluid accumulation in the stroma, resulting in corneal edema and opacity.
In DMEK, the diseased Descemet’s membrane and dysfunctional endothelium are removed by Descemetorhexis, and a healthy donor Descemet’s membrane-endothelium complex is transplanted to restore the pump function of the cornea. Once the graft adheres to the posterior corneal surface, endothelial cells resume water drainage, and corneal edema rapidly improves.
Descemetorhexis without endothelial keratoplasty (DWEK)
Cases have been reported where the cornea spontaneously clears after graft detachment following endothelial transplantation or after Descemetorhexis alone 1). This phenomenon occurs in FECD but not in bullous keratopathy, suggesting that residual endothelial cells in the peripheral cornea of FECD may migrate to the center and restore function 1).
Meta-analyses suggest that with ultrathin Descemet stripping automated endothelial keratoplasty grafts less than 70 μm, the visual acuity difference with DMEK may disappear 2). Nanothin DSAEK (less than 50 μm) may achieve outcomes comparable to DMEK, but it remains an additive transplant rather than a true replacement surgery.
DMEK was performed for the first time in early-onset Fuchs endothelial corneal dystrophy (COL8A2 p.Leu450Trp mutation), and good visual acuity was achieved in all eyes 7). Due to significant postoperative refractive changes, intraocular lens power calculation and follow-up strategies are topics for future investigation 7).
Multiple cases of DMEK graft rejection after COVID-19 vaccination have been reported 6). Vaccine-induced immune response changes may trigger graft rejection, and increased steroid eye drops before and after vaccination are recommended 6).
Intraoperative anterior chamber fibrin formation occurs in approximately 3.7% of DMEK cases and leads to a high rate of graft failure 5). Prophylaxis with preoperative NSAID eye drops, detection of fibrin with intraoperative triamcinolone acetonide, and fibrin dissolution with r-TPA have been proposed as new management strategies 5).
QWhat should patients after DMEK who are scheduled for vaccination do?
A
When receiving vaccination (especially mRNA vaccines) after DMEK, be aware of the risk of rejection. It is recommended to add steroid eye drops (dexamethasone 0.1% 2-4 times daily) before and after vaccination. If you experience decreased vision or redness after vaccination, seek medical attention immediately.
Deng SX, Lee WB, Hammersmith KM, et al. Descemet membrane endothelial keratoplasty: safety and outcomes: a report by the American Academy of Ophthalmology. Ophthalmology. 2018;125(2):295-310. doi:10.1016/j.ophtha.2017.08.015. PMID:28923499.
Sela TC, Iflah M, Muhsen K, Zahavi A. Descemet membrane endothelial keratoplasty compared with ultrathin Descemet stripping automated endothelial keratoplasty: a meta-analysis. BMJ open ophthalmology. 2023;8(1). doi:10.1136/bmjophth-2023-001397. PMID:37914389; PMCID:PMC10626808.
Dunker SL, Dickman MM, Wisse RPL, Nobacht S, Wijdh RHJ, Bartels MC, et al. Descemet Membrane Endothelial Keratoplasty versus Ultrathin Descemet Stripping Automated Endothelial Keratoplasty: A Multicenter Randomized Controlled Clinical Trial. Ophthalmology. 2020;127(9):1152-1159. doi:10.1016/j.ophtha.2020.02.029. PMID:32386811.
Trinh L, Bouheraoua N, Muraine M, Baudouin C. Anterior chamber fibrin reaction during Descemet membrane endothelial keratoplasty. American journal of ophthalmology case reports. 2022;25:101323. doi:10.1016/j.ajoc.2022.101323. PMID:35146197; PMCID:PMC8818478.
Forshaw TRJ, Jørgensen C, Kyhn MC, Cabrerizo J. Acute Bilateral Descemet Membrane Endothelial Keratoplasty Graft Rejection After the BNT162b2 mRNA COVID-19 Vaccine. International medical case reports journal. 2022;15:201-204. doi:10.2147/IMCRJ.S362698. PMID:35444474; PMCID:PMC9015040.
Dzhaber D, Fliotsos MJ, Abousy M, Kancherla S, Siadati S, Eberhart CG, et al. Descemet membrane endothelial keratoplasty in eyes with COL8A2-associated corneal dystrophy. American journal of ophthalmology case reports. 2022;26:101544. doi:10.1016/j.ajoc.2022.101544. PMID:35540705; PMCID:PMC9079234.
Matthaei M, Hribek A, Clahsen T, Bachmann B, Cursiefen C, Jun AS. Fuchs Endothelial Corneal Dystrophy: Clinical, Genetic, Pathophysiologic, and Therapeutic Aspects. Annual review of vision science. 2019;5:151-175. doi:10.1146/annurev-vision-091718-014852. PMID:31525145.
Copy the article text and paste it into your preferred AI assistant.
Article copied to clipboard
Open an AI assistant below and paste the copied text into the chat box.