Laser peripheral iridotomy (LPI) is a procedure in which a laser creates a hole in the peripheral iris, forming a pathway for aqueous humor to flow directly from the posterior chamber to the anterior chamber. This relieves pupillary block, eliminates the pressure difference between the anterior and posterior chambers, and widens the angle 3).
In 1857, Albrecht von Graefe reported surgical iridectomy through a corneal incision. In the 1970s, the argon laser enabled noninvasive iridotomy. In the 1980s, the Q-switched Nd:YAG laser was introduced, allowing efficient perforation in all iris colors due to its photodisruptive effect independent of iris melanin content. Currently, the Nd:YAG laser is the mainstream method for iridotomy.
In the Tajimi Study of Japanese individuals aged 40 years and older, the prevalence of primary angle closure suspect (PACS) was 0.2%, primary angle closure (PAC) was 0.5%, and primary angle closure glaucoma (PACG) was 0.6%. Risk factors include older age, female sex, short axial length, and hyperopia.
Acute primary angle closure (APAC): Perform promptly after diagnosis. LPI is also essential for the fellow eye. Without treatment, 50% experience a contralateral attack within 5 years.
Primary angle closure (PAC) and primary angle closure glaucoma (PACG): All patients require relief of pupillary block. LPI may be sufficient if peripheral anterior synechiae involve less than 50% of the angle.
Primary angle closure suspect (PACS): In the ZAP trial, LPI reduced the risk of progression to PAC by 47% at 6 years and 69% at 14 years 2). However, routine prophylactic LPI is not recommended 2)3).
Other Indications
Iris bombé due to posterior synechiae: Useful for preventing recurrence of secondary pupillary block associated with uveitis.
Plateau iris: LPI is performed to eliminate the pupillary block component. However, about one-third of patients still have residual iridotrabecular contact (ITC) after LPI7).
Pigment dispersion syndrome: Performed to relieve reverse pupillary block, but evidence of efficacy is insufficient.
Aqueous misdirection (malignant glaucoma): LPI is important to rule out the possibility of pupillary block.
Contraindications include opacities of the optical media (corneal edema, intraocular inflammation), extremely shallow anterior chamber preventing safe procedure, and uncooperative patients 3). In cases with corneal endothelial cell density <2,000 cells/mm², consider peripheral iridectomy or lens reconstruction.
QShould LPI be performed prophylactically?
A
Routine prophylactic LPI for all narrow angles is not recommended. The ZAP trial showed a preventive effect of LPI for primary angle closure suspects (PACS), but the incidence itself is low (4–8 per 1,000 eye-years), and the number needed to treat (NNT) over 6 years was 44. Current recommendations are to consider prophylactic LPI only in high-risk eyes (very narrow angle, shallow anterior chamber, tendency for elevated intraocular pressure).
Instill 1–2% pilocarpine eye drops 2–4 times every 15 minutes starting 1 hour before the procedure to induce miosis 3). However, if intraocular pressure is extremely high (≥40 mmHg), the pupillary sphincter may be ischemic and paralyzed, and pilocarpine may not be effective. In such cases, first lower intraocular pressure with a hyperosmotic agent, then use miotics. To prevent postoperative intraocular pressure elevation, instill apraclonidine 1 hour before and immediately after the procedure 3). Perform topical anesthesia with oxybuprocaine hydrochloride eye drops. If corneal edema is present, improve corneal clarity with 10% glycerin eye drops or systemic administration (acetazolamide, mannitol 1.0–3.0 g/kg intravenously over 30–45 minutes) 2). Use mannitol with caution in patients with renal impairment.
Attach an iridotomy contact lens (Abraham, Wise, or Goldmann three-mirror lens) 3). Select a thin area of the iris, such as an iris crypt, in the superior quadrant between 11 and 1 o’clock 2). Avoid the 12 o’clock position because bubbles tend to accumulate there. Avoid iris blood vessels; a location completely covered by the upper eyelid is desirable 2).
The total number of argon laser shots should ideally be kept below 100 to avoid corneal endothelial damage.
Nd:YAG laser alone: 1–3 pulses at 1–6 mJ2)4). Focus the beam within the iris stroma. Energies above 2 mJ carry a risk of lens capsule damage2). Either multiple low-energy shots (10–30) or a few high-energy shots (2–3) are used2).
Argon + Nd:YAG combination: Recommended for dark irides3)4). Stage 1: stretch the iris; Stage 2: prepare for perforation (coagulation provides hemostasis); Stage 3: complete perforation with Nd:YAG laser (2–4 mJ)3).
Full-thickness perforation is confirmed when pigment-laden aqueous humor flows from the posterior chamber into the anterior chamber2). After perforation, the opening expands horizontally to about 200 μm. Transillumination is not a reliable indicator of patency2).
Measure intraocular pressure 1–3 hours after surgery to check for transient IOP elevation3). Administer carbonic anhydrase inhibitors or hyperosmotic agents as needed3). Prescribe topical corticosteroids 3–4 times daily for 4–7 days. Evaluate anterior chamber depth and angle opening by anterior segment OCT at 1 week.
If high IOP persists, consider chronic angle closure due to peripheral anterior synechiae (PAS) and promptly refer to a facility capable of lens reconstruction. If the fellow eye is also at risk for angle closure, consider early prophylactic LPI or lens reconstruction10). Paralytic mydriasis may persist after the attack.
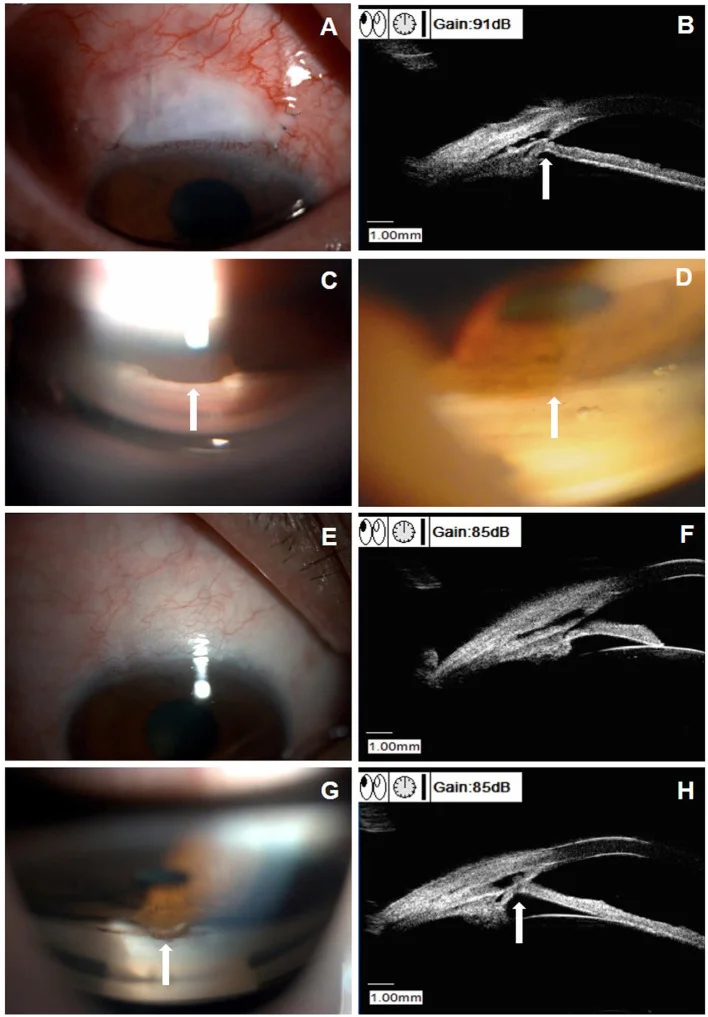
Chen M, Gu Y, Yang Y, et al. Management of Intraocular Pressure Elevation After CO(2) Laser-Assisted Sclerectomy Surgery in Patients With Primary Open-Angle Glaucoma. Front Med (Lausanne). 2021;8:806734. Figure 3. PMID: 35004782; PMCID: PMC8740123; DOI: 10.3389/fmed.2021.806734. License: CC BY.
Multi-panel image showing PAS on slit-lamp (A), UBM (B), and gonioscopy (C), and iris retraction after Nd:YAG laser synechialysis (D). Corresponds to plateau iris re-occlusion and PAS-related peripheral iris closure discussed in section “4. Complications”.
Transient intraocular pressure elevation: This is the most frequent complication. It usually peaks 1 to 4 hours after surgery and returns to preoperative levels within about 6 hours 3). An elevation of 8 mmHg or more from baseline has been reported in 6–10% of cases. It can be prevented by preoperative and postoperative administration of alpha-2 agonists.
Hyphema: Bleeding from the iridotomy site, which is mostly mild. Hemostasis can be achieved by light pressure with a contact lens. Discontinuation of anticoagulants or antiplatelet agents is not necessary.
Postoperative iritis: This is inevitable but usually mild and managed with steroid eye drops 3).
Bullous keratopathy: Risk factors include excessive energy output, preexisting corneal endothelial damage (including cornea guttata), history of acute attack in the affected eye, and diabetes 3). It has been reported that more than 40% of eyes require cataract surgery within 3 years after LPI.
Laser-induced visual disturbances (LIVD): Glare, halos, and linear shadows have been reported in 2–16% of cases 10). There is no significant difference in incidence based on LPI location (superior vs. temporal), and most are transient, resolving spontaneously within 6 months 10).
Retinal misdirection: A complication in which laser irradiation passes through the iris and reaches the retina, included in the list of complications 3). It can be prevented by appropriate site selection and focus adjustment.
Transient optic disc edema: A transient optic disc edema may occur due to a rapid decrease in intraocular pressure following LPI after an acute angle-closure attack 5). A case has been reported in a 65-year-old woman in whom optic disc edema appeared after a rapid drop in intraocular pressure from 54 mmHg to 9 mmHg, which improved within 4 weeks 5). The mechanism is speculated to be exudation from the choroidal capillaries or recovery of axonal flow 5).
Ocular decompression retinopathy (ODR): A rare complication presenting with scattered intraretinal hemorrhages, optic disc edema, and macular edema after LPI6). A case has been reported in a 56-year-old woman whose visual acuity dropped to 20/400 after LPI from an intraocular pressure of 46 mmHg, recovering to 20/40 after one month 6). FA and OCT are useful for differentiation from central retinal vein occlusion6).
Serous ciliochoroidal detachment: A case has been reported in a 78-year-old man who developed extensive ciliochoroidal detachment and macular edema after Nd:YAG LPI8). It improved with systemic and topical steroids 8). Although reports with Nd:YAG are fewer than with argon laser, multifactorial involvement of intraocular pressure fluctuation, inflammation, and vascular stasis is suggested 8).
Re-occlusion due to plateau iris syndrome: Angle closure may still occur upon dilation even after a patent LPI7). A case has been reported of a 41-year-old woman who developed acute angle closure after dilation despite a patent LPI, ultimately requiring trabeculectomy combined with cataract surgery 7). Evaluation of plateau iris by UBM is important 7).
QIs LPI painful? Are complications common?
A
LPI is performed under topical anesthesia, so severe pain is rare. Some patients may feel slight pressure or a momentary sting during the laser application. Most complications, such as transient intraocular pressure elevation or mild iritis, resolve spontaneously. The most serious complication is bullous keratopathy, but it can be prevented by preoperative corneal endothelial evaluation and appropriate laser energy settings.
5. Treatment Outcomes and Comparison with Other Treatments
A multicenter RCT involving 419 patients aged 50 years or older with PAC (IOP ≥30 mmHg) or PACG2). Three-year outcomes were compared between the clear lens extraction (CLE) group and the LPI group.
The CLE group outperformed the LPI group in both QoL and intraocular pressure control 2). For patients aged 50 years or older with high-tension PAC/PACG, CLE is supported as initial treatment 2). However, it should be noted that lens extraction is technically challenging 2). A cost-effectiveness analysis in the UK estimated that CLE is cost-effective at 3 years and cost-saving at 10 years 10).
LPI alone may be insufficient in the long term. Up to 58% of patients who underwent LPI after an acute attack progressed to chronic angle-closure glaucoma (CACG), requiring additional interventions such as medication, trabeculectomy, or lens extraction 11). Early lens extraction may reduce progression to CACG, decrease medication dependence, and lead to better long-term outcomes 11). The optimal timing for lens extraction is 1 to 3 months after the attack 11).
This RCT randomized 889 Chinese PACS patients to LPI in one eye and no treatment in the fellow eye 2)3). At 6 years, PAC progression occurred in 19 eyes in the LPI group vs. 36 eyes in the untreated group (4.19 vs. 7.97 per 1,000 eye-years), a significant difference 2)3). Extended follow-up to 14 years showed 33 eyes in the LPI group vs. 105 eyes in the control group, a 69% relative risk reduction 2). However, the incidence rate itself was low, with an NNT of 44 3). Generalizability to non-Chinese populations is unknown 2).
Alternatives when LPI is difficult during an APAC attack include argon laser peripheral iridoplasty (ALPI) and anterior chamber paracentesis1). ALPI can be performed even in the presence of corneal edema and may lower intraocular pressure at a rate comparable to medical therapy 1).
QWhich is better, LPI or cataract surgery?
A
Based on the EAGLE trial results, for patients aged 50 years or older with high intraocular pressure and primary angle closure (suspect) or primary angle closure glaucoma, lens extraction (cataract surgery) is superior to LPI in terms of intraocular pressure control and the need for additional treatments. However, this does not apply to all angle closure cases; decisions should be individualized considering age, intraocular pressure, extent of peripheral anterior synechiae, and presence of cataract.
When resistance to aqueous humor outflow between the iris and lens increases, relative pupillary block increases. Elevated posterior chamber pressure causes the iris to bow forward, and the peripheral iris occludes the angle. LPI creates a hole in the peripheral iris, forming a direct aqueous pathway from the posterior chamber to the anterior chamber. This equalizes the pressure difference between the anterior and posterior chambers, flattens the iris, and widens the angle 3).
In plateau iris, the ciliary body is displaced anteriorly, pushing the iris root forward. Therefore, relieving pupillary block with LPI alone does not resolve angle closure 7). After LPI, evaluate for plateau iris and add laser iridoplasty if necessary.
The 14-year extended follow-up data from the ZAP trial have been reported, confirming that the preventive effect of LPI persists long-term 2). In the LPI group, acute attack occurred in only one eye, while in the control group, it occurred in five eyes 2). High intraocular pressure, shallow anterior chamber depth, and narrow angle width have been identified as indicators for high-risk PACS 2).
A case has been reported in which angle closure was detected during a home visit for a 97-year-old nursing home resident, and LPI was performed 9). Remote follow-up using a portable slit lamp and iCare tonometer maintained good intraocular pressure control up to 102 days postoperatively 9). This report demonstrates the potential of home-based ophthalmic care in an aging society 9).
In addition to conventional medical therapy, immediate intraocular pressure-lowering methods such as ALPI, anterior chamber paracentesis, and laser pupilloplasty are being considered as alternative approaches 1). These are particularly useful when LPI is difficult due to corneal edema1). If rapid intraocular pressure reduction is achieved, definitive treatment (LPI or lens extraction) can be performed under safer conditions 1).
Chan PP, Zhang X, Tham CCY. Acute Primary Angle-Closure Attack: Management and Prevention. Asia Pac J Ophthalmol. 2025;14:100223.
Pazos M, Traverso CE, Viswanathan A; European Glaucoma Society. European Glaucoma Society - Terminology and guidelines for glaucoma, 6th Edition. Br J Ophthalmol. 2025;109(Suppl 1):1-212. doi:10.1136/bjophthalmol-2025-egsguidelines. PMID:41026937.
European Glaucoma Society. European Glaucoma Society Terminology and Guidelines for Glaucoma, 5th Edition. Br J Ophthalmol. 2021 Jun;105(Suppl 1):1-169. doi:10.1136/bjophthalmol-2021-egsguidelines. PMID:34675001.
Tsuchiya S, Makino S. Transient Optic Disc Swelling After Laser Iridotomy for the Treatment of Acute Angle Closure Glaucoma. Cureus. 2024;16(3):e55765. doi:10.7759/cureus.55765. PMID:38586752; PMCID:PMC10998980.
Ersan S, Zhang C, Sieminski SF. Visually significant ocular decompression retinopathy following laser peripheral iridotomy in a patient with primary acute angle-closure glaucoma. Am J Ophthalmol Case Rep. 2024;36:102215. doi:10.1016/j.ajoc.2024.102215.
Sen S, Das M, Singh Chugh TM. Angle Closure with Patent Laser Peripheral Iridotomy - An Unusual Complication. International journal of applied & basic medical research. 2021;11(4):270-272. doi:10.4103/ijabmr.IJABMR_733_20. PMID:34912693; PMCID:PMC8633701.
Betsch D, Zaki A, Murphy J, Lakosha H, Gupta RR. Extensive serous ciliochoroidal detachments and macular subretinal and intraretinal fluid following laser peripheral iridotomy. American journal of ophthalmology case reports. 2022;26:101483. doi:10.1016/j.ajoc.2022.101483. PMID:35313475; PMCID:PMC8933816.
Nishimura H, Khemukani RJ, Yokoiwa R, Nakayama S, Shimizu E. Primary Angle Closure Observed During a House Visit: A Case Treated With Laser Iridotomy. Cureus. 2024;16(8):e66321. doi:10.7759/cureus.66321. PMID:39246965; PMCID:PMC11377127.
American Academy of Ophthalmology Glaucoma Panel. Primary Angle-Closure Disease Preferred Practice Pattern. San Francisco, CA: American Academy of Ophthalmology; 2025.
Poemen P. Chan, Xiulan Zhang, Tin Aung, Paul T.K. Chew, Nathan Congdon, Tanuj Dada, Seng Kheong Fang, Mingguang He, et al. Controversies, consensuses, and guidelines for acute primary angle closure attack (APACA) by the Asia-Pacific Glaucoma Society (APGS) and the Academy of Asia-Pacific Professors of Ophthalmology (AAPPO). Asia-Pacific Journal of Ophthalmology. 2025;14(6):100223. doi:10.1016/j.apjo.2025.100223.
Copy the article text and paste it into your preferred AI assistant.
Article copied to clipboard
Open an AI assistant below and paste the copied text into the chat box.