Acute glaucoma attack is an ophthalmic emergency characterized by a sudden and severe elevation of intraocular pressure due to rapid angle closure. Intraocular pressure often reaches 40–80 mmHg, and without appropriate treatment within hours, irreversible optic nerve damage occurs. It is considered one of the most urgent conditions in ophthalmic care.
The Asia-Pacific Glaucoma Society (APGS) and the Academy of Asia-Pacific Professors of Ophthalmology (AAPPO) proposed in the 2025 international consensus to unify the terminology to acute primary angle closure attack (APACA)1). This term emphasizes the acute and urgent nature of the disease and intentionally excludes the word “glaucoma,” as prompt treatment may prevent glaucomatous optic neuropathy1). The APGS 2025 panel vote adopted it with 94.11% agreement.
Epidemiologically, it is most common in Chinese and Asian populations, with an annual incidence reported as 6 to 16 per 100,000 people 1). In contrast, the incidence in Western Caucasians is only 2 to 4.1 per 100,000, meaning Asians have about 3 to 4 times higher risk 1, 14). A systematic review by Day et al. reported the prevalence of primary angle-closure glaucoma in European-derived populations, revealing significant racial differences 14). Furthermore, Asian patients are known to have worse visual outcomes compared to Western patients. In a long-term follow-up study by Aung et al. in Singapore, at 4 to 10 years of follow-up, 17.8% of affected eyes were blind, 47.8% had glaucomatous optic neuropathy, and 57% had corrected visual acuity worse than 6/9 Snellen 1, 7). In Japan, the Tajimi Study reported a prevalence of primary angle-closure glaucoma (PACG) of 0.6% in those aged 40 and older, while the Kumejima Study reported 2.2%, showing regional differences, with particularly high frequency of angle-closure glaucoma in Okinawa Prefecture 2). According to global estimates by Quigley et al., the number of primary angle-closure glaucoma patients worldwide was projected to reach approximately 21 million by 2020, with the majority in Asia 10).
An attack occurs when some trigger overlaps in an anatomically predisposed eye. Typically, elderly women with short axial length, shallow anterior chamber, and hyperopia develop an attack after administration of anticholinergic or mydriatic drugs, or triggered by prolonged downward gaze work or nocturnal physiological mydriasis. Animal experiments have shown that when intraocular pressure remains at 50 mmHg or higher for more than 12 hours, irreversible damage occurs to retinal nerve fibers, ganglion cells, and the optic nerve1). Therefore, the time from onset to treatment initiation greatly influences visual prognosis.
The concept of acute attack has been recognized historically for a long time, and various terms have been used, such as “acute angle-closure glaucoma (AACG),” “acute glaucoma attack,” “acute angle-closure crisis (AACC),” and “acute primary angle closure (APAC)” 1). The APGS 2025 positions APACA as the recommended term to organize these mixed terminologies, clarifying its acute, emergent, and primary nature 1). Furthermore, by deliberately not including “glaucoma,” it suggests the possibility of avoiding glaucomatous optic neuropathy through prompt treatment 1). However, it should be noted that even after normalization of intraocular pressure, loss of retinal ganglion cells may progress due to ischemia-reperfusion injury 1).
This disease has a worse prognosis the later it develops. In elderly patients with many comorbidities who present late with high intraocular pressure, conventional drug therapy alone often fails to achieve sufficient intraocular pressure reduction 1). Educational background, time from symptom onset to treatment, and intraocular pressure at presentation have been identified as independent risk factors for blindness 1), making public awareness campaigns and rapid treatment access a public health challenge.
In the APGS 2025 Consensus 1.3, the statement “Acute glaucoma attack is an ophthalmic emergency, and immediate intraocular pressure reduction is essential” was adopted with 100% agreement 1). Furthermore, Consensus 1.9 confirmed with 100% agreement that “Although accurate diagnosis is important, when this disease is clinically suspected, rapid intraocular pressure reduction should be prioritized” 1).
QWho is prone to acute glaucoma attacks?
A
It commonly occurs in elderly women with hyperopia who have short axial length, shallow anterior chamber, and thick lens. Background factors include age-related thickening and forward movement of the lens, increased contact between the iris and lens at the pupillary margin, and anterior displacement of the ciliary processes. Family history and a history of an attack in the fellow eye are also risk factors. Known precipitating drugs include mydriatics, anticholinergics, tricyclic antidepressants, SSRIs, nasal decongestants (containing antihistamines), and antiemetics. Attacks may be triggered by premedication for gastroscopy, sleeping pills, or antipsychotics 1). Prolonged reading, sewing, or other downward-facing postures, as well as natural mydriasis at night, can also induce attacks.
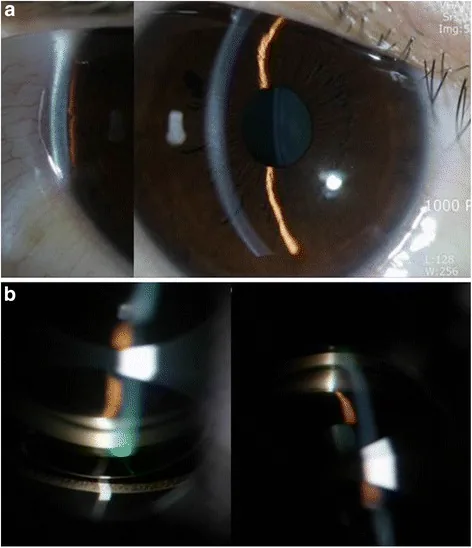
Han YS, et al. Secondary angle closure glaucoma by lupus choroidopathy as an initial presentation of systemic lupus erythematosus: a case report. BMC Ophthalmol. 2015. Figure 2. PMCID: PMC4625431. License: CC BY.
The slit-lamp photograph shows a shallow anterior chamber and a very narrow angle. Gonioscopy demonstrates angle closure by the peripheral iris, suitable for explaining the clinical findings of acute angle-closure attack.
Acute glaucoma attack is characterized by both severe subjective symptoms and objective findings. However, atypical cases lacking all findings may be missed by inexperienced clinicians 1).
The following severe subjective symptoms appear due to rapid intraocular pressure elevation.
Severe eye pain: Intense pain in the unilateral eyeball or deep orbit
Ipsilateral headache: Radiating to the frontal or temporal region
Nausea and vomiting: Gastrointestinal symptoms may be prominent, leading to misdiagnosis as acute gastroenteritis or subarachnoid hemorrhage 1)
Blurred vision and visual loss: Due to corneal edema
Halos around lights: Seeing rainbow-colored rings around light sources
Conjunctival injection
When severe headache, nausea, and vomiting precede as systemic symptoms, there is a risk of misdiagnosis as neurological or gastrointestinal disease1). APGS 2025 emphasizes that these systemic symptoms are important diagnostic clues1).
Ciliary injection and conjunctival vascular congestion
Angle
Extensive angle closure (confirmed in both eyes)
Lens
Glaukomflecken (ischemic necrosis of lens epithelium) 1)
Optic disc
In the acute phase, optic disc edema, venous engorgement, and disc hemorrhage may be observed
Moderate mydriasis is a position where both the sphincter and dilator muscles are co-activated, resulting in maximal relative pupillary block and iris-lens contact at the pupillary margin. Additionally, severe intraocular pressure elevation causes ischemia of the pupillary sphincter, leading to loss of the light reflex. Intraocular pressure measurement and recording with a Goldmann applanation tonometer is recommended in APGS 2025 Consensus 1.6 1).
In chronic angle-closure glaucoma (CACG), intraocular pressure elevation is moderate (20–30 mmHg), hyperemia is mild or absent, and subjective symptoms are scarce, distinguishing it from acute attacks.
QWhat are the typical symptoms of an acute glaucoma attack?
A
The classic triad is eye pain, headache, and nausea/vomiting. This is accompanied by blurred vision, halos, decreased visual acuity, and conjunctival injection. Because severe headache and vomiting may dominate the systemic symptoms, it can be misdiagnosed as a neurological disease or acute gastroenteritis 1). Objective findings include marked intraocular pressure elevation of 40–80 mmHg, corneal edema, shallow anterior chamber, moderate fixed mydriasis, diminished light reflex, conjunctival ciliary injection, extensive angle closure, and occasionally glaukomflecken. Not all of these signs are always present; atypical cases may show only some findings, so if suspicious, immediate intraocular pressure measurement is necessary.
Sympathomimetics and antiemetics: Both enhance pupillary block and angle crowding via mydriatic effects 1).
Situational triggers: Prolonged reading, sewing, or other downward-gaze activities; natural mydriasis in dark rooms or at night.
APGS 2025 Consensus 1.8 confirmed with 88.24% agreement that drugs with mydriatic and cycloplegic effects can induce APACA in eyes with anatomical predisposition 1). A detailed medication history is an important clue for diagnosis.
Further breaking down anatomical factors, the progressive thickening of the lens throughout life with aging is decisive. In hyperopic eyes, the axial length is short and the anterior chamber is shallow, making them more susceptible to the effects of lens thickening. The thickened lens pushes the entire iris forward, a factor called the lens factor. In addition, increased iris-lens contact at the pupillary margin increases resistance to aqueous outflow, leading to relative pupillary block. Histological and imaging studies have shown that the position of the ciliary processes shifts forward with age, and the Kumejima Study confirmed this as a characteristic of eyes with angle closure 2). Quantitative iris parameter studies by Wang et al. showed that iris thickness, iris curvature, and iris area are significantly associated with narrow angles, and anterior segment OCT image analysis has confirmed that cases with greater anterior iris bowing have a higher risk of attack 12).
Myopic eyes are generally considered to have a lower risk of attack, but they are not exempt. In a cross-sectional study by Yong et al., among 427 patients with angle closure, 94 had myopia, and 11 of these (11.7%) had myopia exceeding −5.0 D 1). APGS 2025 Consensus 4.1 adopted with 94.11% agreement that myopic eyes are not completely excluded from angle closure attacks 1). The risk depends mainly on anatomical predisposition such as shallow anterior chamber, not on refraction or axial length1).
QAre there any medications that can easily trigger an acute glaucoma attack?
A
Caution is needed with drugs that have mydriatic or anticholinergic effects. Specific examples include mydriatic eye drops (tropicamide, phenylephrine), anticholinergic drugs used as premedication for gastroscopy, tricyclic antidepressants, SSRIs, nasal decongestants and cold medications containing antihistamines, antipsychotics, benzodiazepine hypnotics, antiemetics, and sympathomimetics 1). These cause moderate mydriasis due to paralysis of the pupillary sphincter or overaction of the dilator muscle, and in eyes with anatomical predisposition, they enhance pupillary block and angle crowding 1). When prescribing at-risk drugs, check for shallow anterior chamber or narrow angle, and educate patients to consult an ophthalmologist immediately if eye pain, vision loss, or rainbow-colored halos occur.
The diagnosis of acute glaucoma attack is primarily based on clinical diagnosis combining acute intraocular pressure elevation with subjective symptoms and objective findings. In APGS 2025 Consensus 1.6, it was adopted with 94.11% agreement that “APACA is a clinical diagnosis based on symptoms and signs” 1). However, multiple examinations are necessary to differentiate from other diseases that cause severe intraocular pressure elevation.
Anterior segment OCT: Quantifies anterior chamber depth. During an attack, ACD may shallow to 1.3–1.5 mm, and findings of near contact between cornea and iris can be observed.
Axial length measurement: Supports short axial length (typically less than 22 mm)
Gonioscopy of both eyes: APGS 2025 Consensus 1.10 states that gonioscopy of both eyes is essential with 100% agreement 1). Even if the affected eye is difficult to observe due to corneal edema, findings in the fellow eye are useful for diagnosis 1)
Refraction test (both eyes): Hyperopic refraction is typical. In myopic refractive error, consider the possibility of secondary glaucoma.
When corneal edema makes gonioscopy difficult, anterior segment OCT and ultrasound biomicroscopy (UBM) are useful1). In particular, UBM can evaluate the morphology of the ciliary processes and the posterior surface of the iris, and is excellent for diagnosing plateau iris and lens subluxation2). Furthermore, B-mode ultrasound is useful for excluding posterior segment conditions such as choroidal hemorrhage, choroidal detachment, and vitreous hemorrhage, and is essential in atypical cases resistant to medical and laser therapy1). While the APGS 2025 recommends these imaging tests, it also clearly states that intraocular pressure reduction should not be delayed for the sake of testing1).
Conditions that may be confused with acute glaucoma attack include the following1).
Malignant glaucoma: Caused by anterior rotation of the ciliary body or forward displacement of the vitreous due to abnormal aqueous flow into the vitreous cavity. Differentiated by history of surgery and UBM findings.
Lens subluxation: Anterior subluxation can cause angle closure.
Posterior synechiae: Suspected from history of iritis or diabetes.
Vogt-Koyanagi-Harada disease: Secondary angle closure due to choroidal detachment or ciliary body edema. Laser treatment carries a risk of exacerbating inflammation and requires caution.
Intraocular tumor / choroidal hemorrhage: Causes secondary shallow anterior chamber due to choroidal swelling.
Neovascular glaucoma: Suspect if rubeosis (iris neovascularization) is present1).
Anterior lens subluxation: Suspect when the affected eye has shallow anterior chamber and high intraocular pressure, but the fellow eye has open angle and deep anterior chamber1).
In APGS 2025 Consensus 1.7, it was adopted with 94.11% agreement that secondary causes should be actively suspected when the fellow eye has open angle and deep anterior chamber, the cornea of the affected eye is relatively clear, or iris neovascularization is observed1). When these findings are present, it is necessary to exclude conditions such as lens subluxation and neovascular glaucoma, which may change the indication for invasive procedures.
QHow is acute glaucoma attack diagnosed?
A
Clinical diagnosis based on symptoms and signs is the principle 1). Diagnosis is relatively easy if marked intraocular pressure elevation of 40–80 mmHg, corneal edema, shallow anterior chamber, moderate mydriasis with fixed pupil, and extensive angle closure on gonioscopy are observed. Perform intraocular pressure measurement with Goldmann applanation tonometry, binocular gonioscopy, anterior chamber depth assessment with anterior segment OCT, corneal endothelial cell examination, axial length measurement, refraction test, and fundus examination1, 2). If gonioscopy is difficult due to corneal edema, supplement with UBM, anterior segment OCT, or B-mode ultrasound. However, APGS 2025 states with 100% consensus that “accurate diagnosis is important, but rapid intraocular pressure reduction should be prioritized” 1), and diagnostic tests should not delay treatment.
The treatment of acute glaucoma attack centers on rapid intraocular pressure reduction and relief of relative pupillary block in the acute phase. After the attack is resolved, long-term management for appropriate intraocular pressure control and recurrence prevention is important. The 5th edition of the Glaucoma Practice Guidelines presents lens reconstruction as an important treatment option for APAC2).
During an attack, administer the following drugs promptly and concurrently.
Drug
Dosage and Administration
Action and Precautions
20% Mannitol (hyperosmotic agent)
1.0–2.0 g/kg intravenously over 30–60 minutes 2)
Maximum IOP reduction occurs at 60–90 minutes, lasting 4–6 hours. Risk of acute renal failure in renal impairment, risk of pulmonary edema in heart failure/pulmonary congestion 2)
Glycerol (10% glycerol)
300–500 mL intravenously over 45–90 minutes 2)
Maximum IOP reduction occurs at 30–135 minutes, lasting about 5 hours. Metabolized to glucose; caution in diabetic patients 2)
1–2% Pilocarpine hydrochloride
Instill 2–3 times per hour 2)
Aims to relieve pupillary block by miosis. In cases of sphincter paralysis, miosis may not be achieved, and there is a risk of worsening pupillary block due to forward movement of the ciliary body2)
Acetazolamide
10 mg/kg orally or intravenously2)
Reduces intraocular pressure by suppressing aqueous humor production. Caution for metabolic acidosis and hypokalemia.
Beta-blocker eye drops
Twice daily
Suppresses aqueous humor production
Alpha-2 agonist eye drops
2-3 times daily
Suppresses aqueous humor production and partially enhances outflow
The use of pilocarpine requires careful judgment. If the pupillary sphincter is ischemic due to high intraocular pressure, frequent administration does not achieve miosis, and the forward movement of the ciliary muscle may paradoxically worsen pupillary block2). At the time of initial administration, the presence or absence of a miotic effect should always be confirmed. Systemic absorption may also cause parasympathetic stimulation symptoms such as abdominal pain 2).
Systemic administration of hyperosmotic agents is particularly risky in elderly patients or those with comorbidities. A rapid increase in extracellular fluid volume places a burden on the circulatory system and may cause pulmonary edema in patients with heart failure or pulmonary congestion 2). Mannitol is excreted renally, so in cases of renal impairment, it can lead to increased plasma osmolality and circulating plasma volume, potentially causing acute renal failure 2). Additionally, during an attack, patients are often already dehydrated due to vomiting, and the diuretic effect of mannitol may further worsen dehydration 2). Glycerol produces glucose during metabolism and has an energy content of 637 kcal per liter, so caution is needed when administering it to diabetic patients 2). The APGS 2025 also notes that intravenous acetazolamide and mannitol can cause serious side effects ranging from paresthesia and confusion to fatal pulmonary edema and acute renal failure, so alternative treatments are desirable in elderly patients or those with comorbidities 1).
Once intraocular pressure is sufficiently lowered by medication and the cornea becomes clear, laser peripheral iridotomy (LPI) is performed. LPI is a definitive treatment to relieve relative pupillary block and is recommended as grade 1A in the 5th edition of the Glaucoma Clinical Practice Guidelines 2).
Perform after the cornea is sufficiently clear. Laser irradiation through an opaque cornea carries a high risk of developing bullous keratopathy2).
Laser selection: Argon laser alone requires a large total energy and poses a high risk of corneal endothelial damage, so Nd:YAG laser alone or combined argon + YAG is recommended.
Pre- and post-operative apraclonidine eye drops: To prevent transient intraocular pressure elevation after surgery.
Irradiation site: Attach an iridotomy contact lens (e.g., Abraham, Pollak) and irradiate the most peripheral part of the iris. A position hidden by the upper eyelid is desirable; the 12 o’clock position should be avoided because bubbles tend to collect there.
Standard laser settings include argon first-stage Stretch (200–400 μm, 200 mW, 0.2 seconds, 2–10 shots) to stretch the iris, second-stage Thinner (50 μm, 800–1000 mW, 0.02 seconds, until just before perforation, preferably fewer than 100 shots considering endothelial damage), and Nd:YAG third-stage (2.0–4.0 mJ, 1–2 shots) to complete perforation. Complications of LPI include hyphema, localized cataract, re-occlusion, and bullous keratopathy.
The 5th edition of the Glaucoma Clinical Practice Guidelines presents lens reconstruction as an important and effective treatment option for APAC2). APGS/AAPPO 2025 also supports considering early lens reconstruction after attack resolution when facilities, surgeon experience, corneal clarity/inflammation, lens/cataract status, anatomy, and patient factors are appropriate1).
A UK 5-year follow-up study reported better long-term outcomes with early lens reconstruction than with LPI alone. Interpretation and applicability depend on the study population, ocular findings, and surgical conditions1). APGS/AAPPO 2025 supports considering early lens reconstruction after attack resolution when conditions are appropriate1).
A UK 5-year follow-up study reported better long-term outcomes with early lens reconstruction than with LPI alone. Interpretation and applicability depend on the study population, ocular findings, and surgical conditions1). APGS/AAPPO 2025 supports considering early lens reconstruction after attack resolution when conditions are appropriate1).
The EAGLE trial was a randomized controlled trial demonstrating the long-term outcomes of clear-lens extraction for primary angle closure disease. It followed patients with primary angle closure glaucoma or primary angle closure with intraocular pressure >30 mmHg for 36 months, and showed that the early lens extraction group was superior to conventional treatment in terms of intraocular pressure control, quality of life scores, and cost-effectiveness 6). A randomized controlled trial by Husain et al. compared primary phacoemulsification with laser peripheral iridotomy for acute primary angle closure eyes, and at 2-year follow-up, the phacoemulsification group showed better intraocular pressure control, greater reduction in peripheral anterior synechiae, and lower medication requirements 8). Furthermore, a prospective case series by Lai et al. reported that phacoemulsification for eyes with primary angle closure glaucoma and cataract significantly improved postoperative intraocular pressure, number of medications, and angle opening 11). Another randomized controlled trial by Tham et al. compared phacoemulsification with trabeculectomy in medically uncontrolled chronic primary angle closure glaucoma without cataract, and found that the phacoemulsification group had fewer postoperative complications and equivalent or better long-term intraocular pressure control 9).
The Japanese Glaucoma Treatment Guidelines, 5th edition, also specify lens extraction (recommendation level 1A) for primary angle closure glaucoma and primary angle closure based on these international evidence 2). The American Academy of Ophthalmology’s Primary Angle-Closure Disease Preferred Practice Pattern (2026 edition) also treats laser treatment and lens extraction as major treatment options for primary angle closure disease 3). The European Glaucoma Society (EGS) 6th edition guidelines (2025 edition) also update the standard framework for glaucoma management including angle closure disease 4).
APGS 2025 states that the traditional stepwise approach of “medication → laser peripheral iridotomy → trabeculectomy or phacoemulsification when necessary” is insufficient for late-onset or high intraocular pressure cases, and presents the following alternative treatments as early options 1).
Argon Laser Peripheral Iridoplasty (ALPI)
Mechanism: Circular laser burns of long duration, low power, and large spot size are applied to the peripheral iris, causing contraction of the iris stroma and mechanical widening of the angle.
Evidence: In a prospective randomized controlled trial by Lam et al., ALPI achieved faster intraocular pressure reduction than systemic medication; in the ALPI group, mean intraocular pressure decreased to 30.8 mmHg at 15 minutes and 24.1 mmHg at 30 minutes 5). Systemic medication resulted in significantly higher intraocular pressure at the same time points, and intraocular pressure control within 2 hours of treatment initiation was superior in the ALPI group 1, 5).
Indications: Particularly useful in cases where laser peripheral iridotomy cannot be effectively performed due to corneal edema.
APGS 2025 Consensus 2.5 was adopted with 94.12% agreement 1)
Laser Pupilloplasty (LPP)
Mechanism: A 532 nm frequency-doubled laser is used to cauterize the iris at the pupillary margin, causing it to contract outward and relieve pupillary block.
Advantages: Can be performed even with poor corneal clarity; easier to perform at the 3 and 9 o’clock positions, even in patients with pain or nausea.
Evidence: LPP alone or in combination with ALPI achieves significant intraocular pressure reduction within 2 hours of the attack.
APGS 2025 Consensus 2.6 was adopted with 88.23% agreement 1)
Anterior Chamber Paracentesis (ACP)
Mechanism: A 30G needle or stab knife is inserted at the 3 or 9 o’clock position to drain aqueous humor without aspiration. Due to the internal friction of the 30G needle, intraocular pressure naturally stabilizes at 12–15 mmHg 1)
Advantages: Immediate normalization of intraocular pressure. Can be performed even in facilities without argon laser equipment or trained personnel.
Evidence: In APACA eyes with initial IOP <60 mmHg, it was superior to mannitol infusion in visual improvement, and no major complications were observed 1)
APGS 2025 Consensus 2.7 was adopted with 94.12% agreement 1)
Corneal Indentation
Mechanism: A small-diameter 4-mirror gonioscopy lens (Posner, Sussman, etc.) or a smooth fingertip is used to compress the cornea through the eyelid, temporarily opening the angle and facilitating aqueous outflow.
Indications: Initial management in areas with limited access to ophthalmic equipment.
APGS 2025 Consensus 4.4 was adopted with 88.23% agreement 1)
On the other hand, emergency trabeculectomy and emergency phacoemulsification for APACA eyes that cannot be controlled with medication are to be avoided according to APGS 20251). The success rate of trabeculectomy alone for medically uncontrolled APACA eyes is limited, with reports of qualified success at 56.2% and complete success at only 9.4%1). Furthermore, performing phacoemulsification in a “hot and angry” eye carries significant risks of serious complications such as poor visibility due to corneal edema, shallow anterior chamber, small and deformed pupil, risk of iris prolapse due to atonic iris, and intraoperative inflammation1).
The fellow eye is at high risk after APACA in one eye. Evaluate angle configuration, lens/cataract status, ocular and systemic factors, then consider prophylactic LPI as a basic option and lens extraction when indicated2). APGS 2025 Consensus 2.3 adopted with 100% agreement starting pilocarpine eye drops in the fellow eye while the affected eye is being treated until LPI can be performed1).
Intravenous infusion of 20% mannitol 1.0–2.0 g/kg over 30–60 minutes (caution for renal impairment)
Start frequent instillation of 1–2% pilocarpine (confirm miotic effect)
Administer acetazolamide, beta-blocker eye drops, and betamethasone eye drops concomitantly
Start pilocarpine eye drops in the fellow eye
Perform LPI after corneal clearing (instill apraclonidine hydrochloride before and immediately after surgery)
Postoperative prescription example: 0.1% betamethasone eye drops 4 times daily + glaucoma eye drops and carbonic anhydrase inhibitors as needed based on intraocular pressure
The next day, evaluate angle opening with anterior segment OCT; if PAS remains or high intraocular pressure persists, promptly refer to a facility capable of lens reconstruction
Plan lens reconstruction 1–3 months after resolution of the attack
Evaluate the fellow eye angle, lens/cataract status, and systemic condition; consider prophylactic LPI as the basic option and lens extraction when indicated
For facilities where emergency surgery cannot be performed on the same day, a realistic approach is to first relieve the attack with medication and LPI, and then perform lens reconstruction surgery within 1 to 3 months after the attack 1, 2).
QIs cataract surgery necessary after the attack subsides?
A
Lens reconstruction after attack resolution is an important option, and APGS/AAPPO 2025 supports considering early surgery when conditions are appropriate1). It should not be applied mechanically to every case; corneal clarity, inflammation, cataract/lens factors, peripheral anterior synechiae, and surgeon experience should guide the decision. The fellow eye is also high risk, so evaluate the angle and lens/cataract status, consider prophylactic LPI as the basic option, and add lens extraction when indicated2).
6. Pathophysiology and Detailed Mechanism of Onset
The posterior surface of the iris and the anterior surface of the lens are in physiological contact at the pupillary margin, and aqueous humor flows from the posterior chamber to the anterior chamber through the pupil. With aging, the lens thickens and moves forward, increasing the iris-lens contact at the pupillary margin and raising resistance to aqueous outflow. This is called relative pupillary block. When posterior chamber pressure exceeds anterior chamber pressure, the iris bulges forward convexly, covering the trabecular meshwork almost completely, leading to a rapid rise in intraocular pressure1).
In hyperopic eyes, the axial length is short and the anterior chamber is shallow, making the effect of lens thickening more pronounced. Once pupillary block occurs, increased posterior chamber pressure causes further forward bulging of the iris, and at the same time, iris stromal edema due to elevated intraocular pressure further enhances the pupillary block, creating a vicious cycle. Thus, intraocular pressure reaches 40–80 mmHg within a few hours.
Pupillary block is maximal at moderate mydriasis. In this position, both the sphincter and dilator muscles are co-activated, and the iris is most relaxed, making broad contact with the anterior lens surface 1). Therefore, pharmacological dilation with anticholinergics or sympathomimetics, dark environments, and natural dilation due to strong stress can trigger an attack. In contrast, complete mydriasis or complete miosis results in relatively less pupillary block.
Although rare, attacks due to the plateau iris mechanism also exist. In this mechanism, the iris root is bent forward, and during mydriasis, the ciliary body mechanically pushes the iris root from behind, directly occluding the angle. In plateau iris, the central anterior chamber depth is relatively preserved, but the peripheral angle is acutely narrow. On UBM, the central iris is flat, the root is thick and bent forward, with anterior displacement of the ciliary processes and obliteration of the ciliary sulcus being characteristic. If high intraocular pressure persists after laser iridotomy, involvement of the plateau iris mechanism should be suspected, and additional laser gonioplasty (LGP) or lens extraction should be considered 2).
Imaging studies suggest that choroidal expansion may increase posterior chamber pressure, pushing the iris-lens diaphragm forward and narrowing the anterior chamber angle 1). However, APGS 2025 Consensus 1.5 “Choroidal expansion is an initiating factor for APACA” achieved only 41.17% agreement and was not established 1). Quantification of causality and contribution requires future large-scale imaging studies.
A rapid rise in intraocular pressure causes ischemia of the pupillary sphincter, leading to loss of the light reflex. The lens epithelium also undergoes ischemic necrosis, leaving white opacities in the pupillary area. These are called glaucomflecken and are important findings suggesting a history of past attacks 1).
Optic neuropathy can progress due to mechanical and ischemic damage from high intraocular pressure during the attack, as well as ischemia-reperfusion injury after normalization of intraocular pressure1). APGS 2025 states that retinal ganglion cell loss may continue even after intraocular pressure is controlled 1). Therefore, it is not enough to say “the pressure is down, so we are safe”; long-term follow-up of the optic nerve and visual field is necessary.
APACA eyes exhibit marked anterior chamber inflammation. Protein leakage from iris capillaries due to high intraocular pressure, ischemic necrosis of the pupillary sphincter and dilator muscles, and increased aqueous humor protein due to endothelial cell damage are observed as inflammatory cells and fibrin in the anterior chamber. APGS 2025 Consensus 2.2, that APACA eyes present with severe inflammation and therefore topical and, when necessary, systemic anti-inflammatory therapy should be used, was adopted with 100% agreement 1). Quiescence of inflammation is important for preventing bullous keratopathy after LPI, preventing pupillary synechiae, and preparing for early lens reconstruction surgery.
Various complications may persist after an acute attack. Typical examples include paralytic mydriasis with loss of the light reflex, glaucomflecken, pigment release from the iris stroma, localized cataract, formation of peripheral anterior synechiae (PAS), and decreased corneal endothelial cell count. It is known that bullous keratopathy after LPI is more common in cases with cornea guttata, diabetes, a history of acute attack, or already reduced corneal endothelial cells 2). Therefore, preoperative corneal endothelial cell examination is essential, and in cases with low endothelial cell count, surgical peripheral iridectomy should be considered 2).
The treatment paradigm for acute glaucoma attacks is changing significantly toward the late 2020s. In addition to the conventional “medical treatment → LPI,” the APGS Guidelines 2025 present the following new treatment strategies 1).
Early alternative treatments: Actively selecting ALPI, LPP, or ACP in the early stage can lower intraocular pressure to a safe range within 30 minutes while avoiding systemic drug side effects 1, 5)
Early lens reconstruction: Given the high conversion rate to CACG of up to 58% after LPI alone, lens reconstruction at 1–3 months after attack resolution should be more actively considered 1)
Combined goniosynechialysis (GSL): When there is a CACG component with extensive PAS, the option of combining GSL or goniotomy with lens reconstruction is also being considered 1)
Subconjunctival dexamethasone: A randomized controlled trial has reported that adding subconjunctival dexamethasone to conventional treatment improves intraocular pressure reduction and treatment success rate 1). Optimization of administration route and dosage remains a future challenge
Management in resource-limited settings: Corneal indentation has been proposed as a viable option in areas where argon laser is not available 1)
On the other hand, many unresolved issues remain. The optimal timing of lens reconstruction, the role of MIGS (minimally invasive glaucoma surgery) in angle-closure glaucoma, new drug combination therapies, and image-based prediction models for onset require validation through large-scale prospective studies 1).
Chan PP, Zhang X, Aung T, et al. Controversies, consensuses, and guidelines for acute primary angle closure attack (APACA) by the Asia-Pacific Glaucoma Society (APGS) and the Academy of Asia-Pacific Professors of Ophthalmology (AAPPO). Asia Pac J Ophthalmol (Phila). 2025;14(6):100223. PMID: 40615047. doi:10.1016/j.apjo.2025.100223.
Gedde SJ, Chopra V, Vinod K, Bowden EC, Kolomeyer NN, Challa P, et al.; American Academy of Ophthalmology Preferred Practice Pattern Glaucoma Committee. Primary Angle-Closure Disease Preferred Practice Pattern. Ophthalmology. 2026;133(4):P153-P201. PMID: 41665581. doi:10.1016/j.ophtha.2025.12.030.
Pazos M, Traverso CE, Viswanathan A; European Glaucoma Society. European Glaucoma Society - Terminology and guidelines for glaucoma, 6th Edition. Br J Ophthalmol. 2025;109(Suppl 1):1-212. doi:10.1136/bjophthalmol-2025-egsguidelines. PMID:41026937.
Lam DS, Lai JS, Tham CC, Chua JK, Poon AS. Argon laser peripheral iridoplasty versus conventional systemic medical therapy in treatment of acute primary angle-closure glaucoma : a prospective, randomized, controlled trial. Ophthalmology. 2002;109(9):1591-6. doi:10.1016/s0161-6420(02)01158-2. PMID:12208703.
Azuara-Blanco A, Burr J, Ramsay C, et al. Effectiveness of early lens extraction for the treatment of primary angle-closure glaucoma (EAGLE): a randomised controlled trial. Lancet. 2016;388(10052):1389-1397.
Aung T, Friedman DS, Chew PT, Ang LP, Gazzard G, Lai YF, et al. Long-term outcomes in asians after acute primary angle closure. Ophthalmology. 2004;111(8):1464-9. doi:10.1016/j.ophtha.2003.12.061. PMID:15288972.
Husain R, Gazzard G, Aung T, Chen Y, Padmanabhan V, Oen FT, et al. Initial management of acute primary angle closure: a randomized trial comparing phacoemulsification with laser peripheral iridotomy. Ophthalmology. 2012;119(11):2274-81. doi:10.1016/j.ophtha.2012.06.015. PMID:22885123.
Tham CC, Kwong YY, Baig N, Leung DY, Li FC, Lam DS. Phacoemulsification versus trabeculectomy in medically uncontrolled chronic angle-closure glaucoma without cataract. Ophthalmology. 2013;120(1):62-7. doi:10.1016/j.ophtha.2012.07.021. PMID:22986111.
Quigley HA, Broman AT. The number of people with glaucoma worldwide in 2010 and 2020. Br J Ophthalmol. 2006;90(3):262-7.
Lai JS, Tham CC, Chan JC. The clinical outcomes of cataract extraction by phacoemulsification in eyes with primary angle-closure glaucoma (PACG) and co-existing cataract: a prospective case series. Journal of glaucoma. 2006;15(1):47-52. doi:10.1097/01.ijg.0000196619.34368.0a. PMID:16378018.
Wang B, Sakata LM, Friedman DS, et al. Quantitative iris parameters and association with narrow angles. Ophthalmology. 2010;117(1):11-17.
Aung T, Ang LP, Chan SP, Chew PT. Acute primary angle-closure: long-term intraocular pressure outcome in Asian eyes. American journal of ophthalmology. 2001;131(1):7-12. doi:10.1016/s0002-9394(00)00621-8. PMID:11162972.
Day AC, Baio G, Gazzard G, Bunce C, Azuara-Blanco A, Munoz B, et al. The prevalence of primary angle closure glaucoma in European derived populations: a systematic review. The British journal of ophthalmology. 2012;96(9):1162-7. doi:10.1136/bjophthalmol-2011-301189. PMID:22653314.
Copy the article text and paste it into your preferred AI assistant.
Article copied to clipboard
Open an AI assistant below and paste the copied text into the chat box.