The vitreous body is a transparent tissue without blood vessels, so bleeding from adjacent tissues spreads into the vitreous gel, causing vitreous hemorrhage. Vitreous hemorrhage is a condition in which bleeding into the vitreous cavity enters the gel through a tear in the vitreous membrane. It also includes the spread of preretinal hemorrhage (between the internal limiting membrane and the nerve fiber layer, or between the internal limiting membrane and the posterior vitreous membrane) into the vitreous cavity.
The incidence of spontaneous vitreous hemorrhage is reported to be approximately 7 per 100,000 population per year, and 4.8 per 10,000 in Taiwan, varying by population characteristics, geography, and other factors. It often presents with rapid, painless, significant vision loss, making it a common condition encountered not only by ophthalmologists but also in emergency departments. The most common cause is proliferative diabetic retinopathy, followed by posterior vitreous detachment and ocular trauma. 12)
ICD-10 code: H43.1
QHow often does vitreous hemorrhage occur?
A
It is estimated to occur in about 7 per 100,000 population per year, and is a relatively common cause of sudden vision loss in ophthalmology. The incidence varies depending on the underlying cause and patient background.
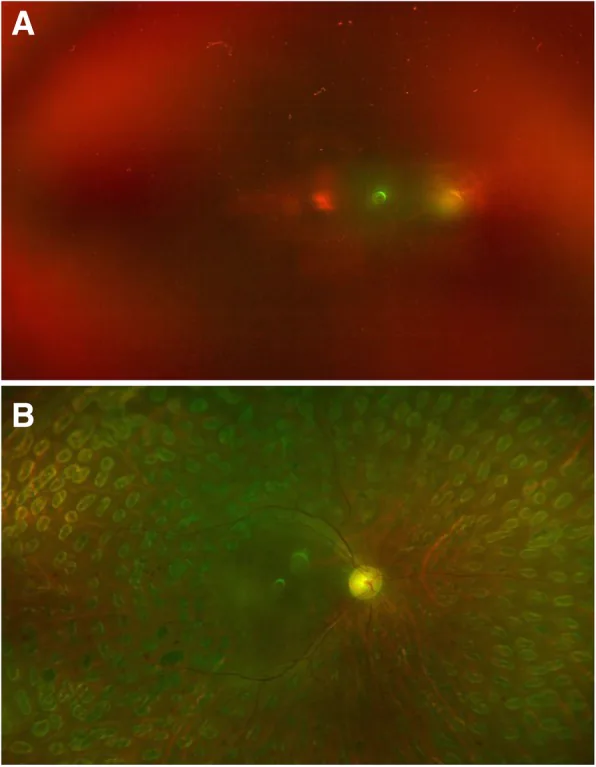
Hu X, et al. Reoperation following vitrectomy for diabetic vitreous hemorrhage with versus without preoperative intravitreal bevacizumab. BMC Ophthalmol. 2019. Figure 4. PMCID: PMC6743107. License: CC BY.
a Right eye of a woman with type 2 diabetes, showing vitreous hemorrhage without tractional retinal detachment and hand motion vision; b She received intravitreal bevacizumab preoperatively, followed by vitrectomy and gas tamponade one week later, improving to 20/50 at six months. This corresponds to vitreous hemorrhage discussed in section “2. Main Symptoms and Clinical Findings.”
Sudden painless vision loss and blurred vision are the main complaints.
Sudden vision loss/blurred vision: Ranges from mild to severe depending on the amount, location, and extent of bleeding. Presents as sudden blurred vision or vision loss.
Floaters/“cobweb” appearance: Newly appearing floaters, shadows, or a “cobweb”-like appearance may be described.
Red vision: Some patients report erythropsia, where the visual field appears reddish.
Worsening in the morning: Symptoms may be worse in the morning due to blood settling over the macula overnight.
Slit-lamp examination identifies red blood cells in the anterior vitreous, the presence of pigment epithelial cells, and inflammatory cells in the anterior chamber or vitreous. Over time, as hemolysis progresses, the remaining cells become whitish. If the hemorrhage is small, the red color may not be prominent, and differentiation from uveitis may be necessary.
Vitreous hemorrhage becomes white over months (organization), so white does not necessarily indicate inflammation. Also, the distribution is often uneven, with dense sedimentation inferiorly and thinner superiorly where the retina may be visible.
Fresh hemorrhage: Appears red with clumped or feathery reflections. Over time, it changes from yellowish-white to grayish-white, sometimes making differentiation from old hemorrhage or vitreous opacity difficult.
Old hemorrhage: Changes to yellowish-white or grayish-white over time. The color can help estimate the time elapsed since the hemorrhage.
Preretinal hemorrhage: Characteristically forms a horizontal level (niveau) on fundus examination. Hemorrhage in the subhyaloid space (scaphoid hemorrhage) presents a characteristic boat-shaped appearance.
Rubeosis iridis: Seen in severe cases with neovascularization.
QIs vitreous hemorrhage painful?
A
Usually, vitreous hemorrhage itself is painless. Sudden painless vision loss or floaters are typical symptoms. If caused by trauma, pain from the injury may be present.
The three most common causes account for 59–88.5% of all cases.
Proliferative Diabetic Retinopathy
Rupture of neovascularization: Retinal ischemia leads to production of angiogenic factors such as VEGF, causing proliferation of fragile new blood vessels. Normal eye movements, acute posterior vitreous detachment, and fibrovascular contraction trigger bleeding.
Frequency: The most common of the three major causes. Poorly controlled diabetes is a high risk factor.
Closed and open globe injuries: Blunt trauma compresses the globe and causes retinal vessel rupture. In open globe injuries, bleeding can occur through the full thickness of the eye.
Age characteristics: Vitreous hemorrhage in individuals under 40 years of age is often associated with a history of trauma.
Terson syndrome: Vitreous hemorrhage associated with subarachnoid hemorrhage. It occurs when elevated intracranial pressure compresses and ruptures retinal venules. Incidence is 3–20% of subarachnoid hemorrhage cases.
Idiopathic intracranial hypertension (IIH): A rare but important cause. Associated with papilledema, acute elevation of intracranial pressure leads to venous compression and rupture.
Blood disorders/coagulopathy: Leukemia, thrombocytopenia, etc. In diseases such as leukemia and uveitis, wait for absorption of vitreous hemorrhage while providing medical treatment.
Age under 40: Trauma is more likely to be the main cause.
Anticoagulants/antiplatelet drugs: Aspirin does not slow the progression of diabetic retinopathy, and there is no clear evidence that it increases the risk of vitreous hemorrhage. If anticoagulation therapy is medically necessary, discontinuation for the purpose of resolving vitreous hemorrhage is not recommended. 5)
Vitreous hemorrhage is a clinical finding, so identifying the underlying cause is important. If the bleeding is mild and the fundus can be observed, identifying the cause is relatively easy.
Diabetes, hypertension, sickle cell disease, trauma, and past retinal diseases or ophthalmic surgeries are important clues for diagnosis. The presence of systemic diseases such as hypertension or diabetes, and the condition of the fellow eye, may help infer the cause of bleeding.
Dilated fundus examination: Assess the pattern and distribution of hemorrhage in the vitreous cavity, and search for retinal tears and retinal detachment. If associated with acute posterior vitreous detachment, use scleral depression to examine the peripheral retina.
Ultra-widefield scanning laser ophthalmoscopy (SLO): For mild to moderate hemorrhage, ultra-widefield fundus imaging allows extensive observation of peripheral retinal tears, neovascularization, and ischemic areas.
Examination of the fellow eye: Often provides clues to the underlying disease.
When the fundus is completely obscured by vitreous hemorrhage, B-mode ultrasonography is essential. Use B-mode to assess the extent and severity of hemorrhage and to check for posterior vitreous detachment. In vitreous hemorrhage due to age-related macular degeneration, subretinal hemorrhage may be present, so pay attention to the retinal reflection near the macula.
Fresh vitreous hemorrhage shows clumped or feathery echoes with mobility. Posterior vitreous detachment is seen as a membrane echo. Continuity with the optic disc is a key point for differentiating from retinal detachment. When hemorrhage aggregates on the posterior vitreous membrane, it may be difficult to distinguish from detached retina.
The sensitivity of B-mode ultrasonography for detecting retinal tears in fundus-obscuring vitreous hemorrhage associated with PVD is reported to be 44–100%. 10) Since false negatives can occur with ultrasound alone, detailed fundus examination after resolution of hemorrhage is important.
The main conditions requiring differentiation from vitreous hemorrhage are listed below.
Uveitis: Vitreous opacities (inflammatory cells, fibrin) may resemble hemorrhage. Slit-lamp examination for cell identification, presence of keratic precipitates, and systemic symptoms are important for differentiation.
Endophthalmitis: Presents with rapid vision loss, eye pain, and anterior chamber inflammation. History of infection risk is essential.
Vitreous amyloidosis: White to gray-white opacities in the vitreous. Differentiated by color, morphology, and history.
Intraocular tumors: Retinoblastoma (children), choroidal melanoma, etc., may cause vitreous hemorrhage. B-mode ultrasound and MRI are important for tumor identification.
Asteroid hyalosis: White asteroid bodies scattered throughout the vitreous. Usually asymptomatic, differentiation from hemorrhage is relatively easy.
ERG (electroretinogram): Performed to assess retinal function when needed, especially when the cause is unknown or retinal disease is suspected.
Orbital CT scan: Used when open globe injury is suspected, and to rule out intraocular foreign bodies.
Blood pressure measurement and clinical laboratory tests (blood tests): Performed to evaluate diabetes, sickle cell disease, leukemia, thrombocytopenia, and other hematological abnormalities.
QHow is it diagnosed when the fundus is not visible?
A
B-mode ultrasonography is essential. It helps differentiate from retinal detachment by assessing vitreous echoes due to hemorrhage, presence of posterior vitreous detachment, and continuity with the optic disc. Even if the fundus is completely opaque, indirect ophthalmoscopy with scleral depression may allow visualization of the peripheral retina.
If the hemorrhage is mild, observation is continued while waiting for spontaneous absorption. Blood clears at a rate of approximately 1% per day.
Rest and head positioning: Instruct the patient to keep the head elevated during sleep. This allows blood to settle, improving vision and enabling a more complete fundus examination. Advise avoiding strenuous activities.
Management of underlying disease: Patients with systemic diseases such as diabetes or hypertension should receive close ophthalmologic follow-up along with systemic management by an internist or endocrinologist. For conditions like leukemia or uveitis, medical treatment is given while waiting for vitreous hemorrhage absorption.
If neovascularization (e.g., proliferative diabetic retinopathy, retinal vein occlusion) is the cause and the view is adequate, PRP is performed to regress new vessels and reduce the risk of further bleeding. Randomized controlled trials have shown that panretinal photocoagulation reduces the risk of severe vision loss in proliferative diabetic retinopathy by more than 50%. 8)
When the view for PRP is inadequate, anti-VEGF injections are used to regress neovascularization in proliferative retinopathy. For vitreous hemorrhage due to age-related macular degeneration, intravitreal anti-VEGF injection is usually indicated.
In a randomized controlled trial for vitreous hemorrhage associated with proliferative diabetic retinopathy, comparing intravitreal ranibizumab with saline injection, no difference in vitrectomy rates at 16 weeks was observed. Data from DRCR.net Protocol S comparing PRP and intravitreal ranibizumab for proliferative diabetic retinopathy showed similar rates of vitreous hemorrhage at 5 years (approximately 50%). 5)
Because delayed treatment can lead to permanent retinal damage or neovascular glaucoma due to ischemia, it is necessary to carefully consider whether to continue conservative observation or perform surgical treatment. If retinal detachment is present on B-scan, early surgery should be performed to achieve retinal reattachment.
Vitrectomy is indicated in the following cases: 5)
In proliferative retinopathy associated with diabetes, if new vitreous hemorrhage does not resolve within one month, many surgeons perform vitrectomy. However, in known patients with proliferative diabetic retinopathy and a history of PRP, a longer observation period (3–6 months) may be reasonable. Intraoperative endolaser (endophotocoagulation) or preoperative anti-VEGF agents may be considered.
Initial results from DRCR.net Protocol AB compared an initial aflibercept treatment group (100 patients) with an initial vitrectomy plus laser treatment group (105 patients) in patients with vitreous hemorrhage due to proliferative diabetic retinopathy. At 24 weeks, there was no statistical difference in mean visual acuity scores, but the surgery group had faster visual recovery, and about one-third of the aflibercept group required vitrectomy during follow-up (8% in the surgery group). 5)
QHow long does it take for vitreous hemorrhage to resolve spontaneously?
A
Red blood cells disappear at a rate of about 1% per day, and complete absorption may take several months. For mild cases, natural absorption is awaited with observation, but if absorption does not occur or if retinal detachment is present, vitrectomy is indicated.
QWhen should surgery for vitreous hemorrhage be performed?
A
It depends on the underlying disease and the extent of hemorrhage. If retinal detachment is present, early surgery is performed. In proliferative diabetic retinopathy, vitrectomy is considered if new vitreous hemorrhage does not resolve within one month. In patients with a history of PRP, an observation period of 3 to 6 months may be appropriate. For severe vitreous hemorrhage in type 1 diabetes, earlier vitrectomy is advantageous for visual recovery. 9)Vitrectomy is also indicated for vitreous hemorrhage where panretinal photocoagulation cannot be completed. 6)
The vitreous is a transparent tissue without blood vessels, so bleeding from adjacent tissues into the vitreous gel causes vitreous hemorrhage. Leakage of blood into the vitreous cavity is caused by two main mechanisms.
1. Rupture of Normal Blood Vessels Due to Mechanical Force
Acute posterior vitreous detachment (PVD): As a complication of age-related posterior vitreous detachment, vitreous hemorrhage occurs in about 8% of patients. It occurs when retinal blood vessels rupture during vitreous detachment from the retina. 70-95% of vitreous hemorrhages associated with acute posterior vitreous detachment are accompanied by retinal tears or breaks. There is a direct correlation between the amount of hemorrhage and the likelihood of retinal tears. 4)
Blunt trauma (closed globe injury): Compression of the eye in the anteroposterior direction causes the equator to bulge in the coronal plane, creating inward traction from the vitreous to the retina. Especially in young patients, the adhesion between the vitreous and retina is strong, and this traction can cause retinal dialysis, retinal vascular rupture, and vitreous hemorrhage.
Open globe injury: A full-thickness defect in the eye wall occurs, and hemorrhage can occur in all layers of the eye, including vitreous hemorrhage.
Terson syndrome: Increased intracranial pressure raises pressure in the retinal venules, causing them to rupture. Sub-ILM hemorrhage is observed.
Valsalva retinopathy: Sudden increases in intrathoracic or intra-abdominal pressure (e.g., coughing, straining, vomiting) cause acute rupture of retinal blood vessels, leading to sub-ILM hemorrhage that may extend into the vitreous cavity.
Retinal microaneurysms: Localized weakening of the arterial wall leads to aneurysm formation; rupture can cause multilayered hemorrhage including subretinal, preretinal, and vitreous hemorrhage.
When intracranial pressure rises rapidly due to idiopathic intracranial hypertension (IIH) or subarachnoid hemorrhage, the CSF pressure within the optic nerve sheath compresses the central retinal vein and choroidal-retinal anastomotic vessels. This leads to venous stasis, and blood cannot drain through the anastomotic channels, causing rupture and severe hemorrhage that breaks through the internal limiting membrane into the vitreous.
Vosoughi & Micieli (2022) reported a case of idiopathic intracranial hypertension in a 32-year-old obese woman (BMI 54.9 kg/m²) who presented with flashes and floaters without headache, pulsatile tinnitus, or transient visual disturbances, and exhibited vitreous hemorrhage and papilledema. Lumbar puncture opening pressure was 34 cmH₂O. Treatment with acetazolamide 500 mg twice daily led to improvement of papilledema at 3 months and complete resolution of vitreous hemorrhage and visual recovery at 6 months. 3)
Hanai et al. (2022) reported a case of a 12-year-old boy with unilateral dilated petrous apex cyst (PAC) and contralateral vitreous hemorrhage secondary to elevated intracranial pressure. Lumbar puncture opening pressure was 250 mmH₂O. Administration of acetazolamide 250 mg twice daily resulted in gradual resolution of vitreous hemorrhage and papilledema. 1)
Blood released into the vitreous cavity rapidly forms a clot and clears at a rate of approximately 1% per day. Red blood cells are eliminated through the trabecular meshwork, undergo hemolysis and phagocytosis, or remain in the vitreous for several months. The immune response within the vitreous is unique, resembling a low-turnover granuloma, with no initial polymorphonuclear cell reaction. This suppressed inflammatory response reduces damage to ocular tissues and helps maintain transparency of the visual axis.
7. Latest research and future perspectives (investigational reports)
The Diabetic RetinopathyVitrectomy Study (DRVS) was a landmark trial that first demonstrated the efficacy of early vitrectomy for severe vitreous hemorrhage in type 1 diabetes. At the 2-year analysis, the early vitrectomy group showed significantly better visual recovery compared to the observation group. 9) This study, along with advances in small-incision vitrectomy techniques, formed the basis for current vitrectomy indications.
Early surgery for vitreous hemorrhage associated with retinal tears
Tan et al. (2010) conducted a randomized controlled trial comparing early vitrectomy and observation for vitreous hemorrhage associated with retinal tears. Although there was no significant difference in final visual acuity, the incidence of retinal detachment was significantly lower in the early surgery group compared to the observation group. 11) This evidence supports early active intervention in vitreous hemorrhage suspected to be due to retinal tears.
Vitreous hemorrhage after COVID-19 mRNA vaccination
Matsuo & Noda (2022) reported a case of a 60-year-old ophthalmologist with no abnormalities on annual checkups who experienced recurrent vitreous hemorrhage approximately 2.5 months after the second and third doses of the COVID-19 mRNA vaccine (BNT162b2, Pfizer-BioNTech). After each vaccination, a tendency for diastolic blood pressure to increase by 10–20 mmHg over a period of 2–3 months was observed, which was temporally associated with the recurrence of vitreous hemorrhage. Although this is a single case report and insufficient to prove causation, checking vaccination history is recommended in patients with recurrent vitreous hemorrhage and elevated blood pressure after COVID-19 vaccination. 2)
DRCR.net Protocol AB is a randomized controlled trial comparing anti-VEGF monotherapy versus vitrectomy plus laser therapy for vitreous hemorrhage due to proliferative diabetic retinopathy. Data on long-term visual prognosis and conversion rate to surgery are expected to accumulate in the future.
Since vitreous hemorrhage involves various underlying diseases, the prognosis depends on the cause. In general, if macular function is preserved, the visual prognosis is good.
In cases complicated by retinal detachment, whether preoperatively or postoperatively, there is a risk of progression to proliferative vitreoretinopathy and poor prognosis. Caution is required, especially when tractional changes become chronic or when surgery is delayed, as the risk of proliferative vitreoretinopathy increases.
If the underlying disease is appropriately managed, the risk of rebleeding can be reduced. In diabetic retinopathy, regression of neovascularization through panretinal photocoagulation and anti-VEGF therapy is important for preventing rebleeding.
Hanai K, Hashimoto M, Nakamura H.. Unilateral expanding petrous apex cephalocele and contralateral vitreous hemorrhage in a young patient with intracranial hypertension. Am J Ophthalmol Case Rep. 2022;25:101368. doi:10.1016/j.ajoc.2022.101368. PMID:35146212; PMCID:PMC8818526.
Matsuo T, Noda H. Temporal association of vitreous hemorrhage and hypertension after COVID-19 mRNA vaccines. Clin Case Rep. 2022;10:e06657.
Vosoughi AR, Micieli JA.. Vitreous Hemorrhage as the Presenting Sign of Idiopathic Intracranial Hypertension. Case Rep Ophthalmol. 2022;13(3):905-909. doi:10.1159/000526631. PMID:36466053; PMCID:PMC9710450.
Flaxel CJ, Adelman RA, Bailey ST, Fawzi A, Lim JI, Vemulakonda GA, et al. Posterior Vitreous Detachment, Retinal Breaks, and Lattice Degeneration Preferred Practice Pattern®. Ophthalmology. 2020;127(1):P146-P181. doi:10.1016/j.ophtha.2019.09.027. PMID:31757500.
Lim JI, Kim SJ, Bailey ST, et al. Diabetic Retinopathy Preferred Practice Pattern. Ophthalmology. 2025 Apr;132(4):P75-P162. doi:10.1016/j.ophtha.2024.12.020. PMID:39918521.
Kim SJ, Bailey ST, Kovach JL, Lim JI, Vemulakonda GA, Ying GS, et al. Posterior Vitreous Detachment, Retinal Breaks, and Lattice Degeneration Preferred Practice Pattern®. Ophthalmology. 2025;132(4):P163-P196. doi:10.1016/j.ophtha.2024.12.023. PMID:39918519.
Diabetic Retinopathy Study Research Group. Photocoagulation treatment of proliferative diabetic retinopathy: clinical application of Diabetic Retinopathy Study (DRS) findings, DRS report number 8. Ophthalmology. 1981;88:583-600.
Early vitrectomy for severe vitreous hemorrhage in diabetic retinopathy. Two-year results of a randomized trial. Diabetic RetinopathyVitrectomy Study report 2. The Diabetic RetinopathyVitrectomy Study Research Group. Archives of ophthalmology (Chicago, Ill. : 1960). 1985;103(11):1644-52. PMID:2865943.
Sarrafizadeh R, Hassan TS, Ruby AJ, Williams GA, Garretson BR, Capone A Jr, et al. Incidence of retinal detachment and visual outcome in eyes presenting with posterior vitreous separation and dense fundus-obscuring vitreous hemorrhage. Ophthalmology. 2001;108(12):2273-8. doi:10.1016/s0161-6420(01)00822-3. PMID:11733270.
Tan HS, Mura M, Bijl HM. Early vitrectomy for vitreous hemorrhage associated with retinal tears. American journal of ophthalmology. 2010;150(4):529-33. doi:10.1016/j.ajo.2010.04.005. PMID:20579632.
Christoph W. Spraul, Hans E. Grossniklaus. Vitreous hemorrhage. Survey of Ophthalmology. 1997;42(1):3-39. doi:10.1016/s0039-6257(97)84041-6.
Copy the article text and paste it into your preferred AI assistant.
Article copied to clipboard
Open an AI assistant below and paste the copied text into the chat box.