Age-related macular degeneration (AMD) is a disease that causes atrophic or exudative changes in the macula due to age-related changes. It is considered a multifactorial disease involving genetic predisposition and environmental factors such as aging, smoking, sunlight exposure, obesity, and high-fat diet.
Conventionally, AMD was defined as age-related macular abnormalities within a 6,000 μm diameter centered on the fovea in individuals aged 50 years or older. However, the 2024 Japanese clinical guidelines removed the age criterion from the diagnostic criteria and classify AMD into early AMD, intermediate AMD, late AMD, and end-stage AMD1). Late AMD includes neovascular AMD with MNV and atrophic AMD with GA. AMD is a major cause of visual impairment in Japan1).
Japanese epidemiological studies have shown that AMD and its precursor lesions increase with aging. Smoking is an important modifiable risk factor for AMD, and smoking cessation guidance is important from the perspective of prevention and progression control1)2).
There are racial differences, with higher prevalence in Caucasians and Asians, and lower in Hispanics and African Americans2). The prevalence of atrophic AMD is reported to be 0.66–1.34% in Western studies, and in those aged 85 years or older, it is reported to be four times more frequent than neovascular AMD. This is likely to become a major issue in Japan as the population ages. Worldwide, approximately 200 million people are affected by AMD, and this number is projected to increase to approximately 288 million by 20402). The prevalence of late AMD increases exponentially with age, from 0.1% in those aged 50–59 years to 4.3% in those aged 80 years or older2).
The latest Japanese clinical practice guidelines (2024) classify AMD into the following four stages based on the Beckman classification1).
Stage
Characteristics
Early AMD
One or more medium soft drusen (63 to <125 μm)
Intermediate AMD
Large drusen (≥125 μm), RPE abnormalities, subretinal drusenoid deposits
Late AMD
Presence of macular neovascularization (MNV) (including PNV) or geographic atrophy
End-stage AMD
Fibrotic scar or severe vision loss due to cystoid macular degeneration
Small (hard) drusen (<63 μm) are considered physiological aging changes and are not included in early AMD. However, if numerous (20 or more) hard drusen are present, the risk of developing AMD is high1). The 5-year progression rate for intermediate AMD is approximately 18%, but the risk increases markedly in the presence of reticular pseudodrusen (5-year risk 72% with pigmentary abnormalities + large drusen + reticular pseudodrusen)2).
Neovascular AMD
Macular neovascularization (MNV): New blood vessels originating from the choroid or retinal vessels develop in the macula, causing sudden vision loss.
Types: Classified into type 1 MNV (sub-RPE), type 2 MNV (supra-RPE), type 3 MNV (retinal angiomatous proliferation, RAP), and PCV (type 1 MNV with polypoidal lesions)1).
Characteristics in Japan: About half of neovascular AMD cases are pachychoroid neovasculopathy (PNV), and drusen are seen in only about 30% of cases1).
Atrophic AMD
Geographic atrophy (GA): Characterized by well-demarcated atrophy of the RPE, photoreceptors, and choriocapillaris.
Natural course: Begins around the fovea and expands in a horseshoe shape, then ring-shaped. Growth rate is 1.28–2.6 mm²/year3).
MNV during progression: MNV may develop during the course of geographic atrophy; if exudative changes appear, it should be evaluated and treated as neovascular AMD.
QDoes age-related macular degeneration affect both eyes?
A
This disease requires attention for bilaterality. If one eye has late-stage AMD, the fellow eye is at risk of developing MNV. The ARMS2 genotype has been reported as a predictor of fellow eye involvement1). Regular eye examinations and self-checking with an Amsler grid are recommended.
Early stages begin with metamorphopsia (distorted vision) and central scotoma. As it progresses, visual acuity may drop below 0.1. In cases of massive hemorrhage, sudden severe vision loss can occur.
Metamorphopsia: Straight lines appear wavy. Important as an early symptom of MNV onset2).
Central scotoma: Visual field defect in the central to paracentral area. In geographic atrophy, an absolute scotoma corresponding to the atrophic area occurs.
Vision loss: In the neovascular type, rapid decline. In the atrophic type, it progresses slowly, but when atrophy involves the fovea, vision drops to 0.1 or less.
Decreased contrast sensitivity: Occurs early even in the atrophic type with preserved fovea, and is a functional impairment not captured by visual acuity testing8).
Difficulty with dark adaptation: Takes time to adjust to dark environments. May appear before vision loss2).
Reading and distance vision impairment: Even extrafoveal geographic atrophy affects quality of life8). About half of patients with geographic atrophy experience rapid disease progression, which is said to have a significant negative impact on quality of life3).
Photopsia: Flashing lights. Although infrequent, it may be reported early in the onset of neovascularization2).
In cases of unilateral onset, it is often not noticed in daily life. The severity of symptoms varies depending on the location and size of MNV, and the extent of subretinal fluid, hemorrhage, and fibrous scarring. In the neovascular type, the time to legal blindness tends to be shorter than in the atrophic type, and prompt consultation is recommended when metamorphopsia appears.
Clinical findings (findings confirmed by physician examination)
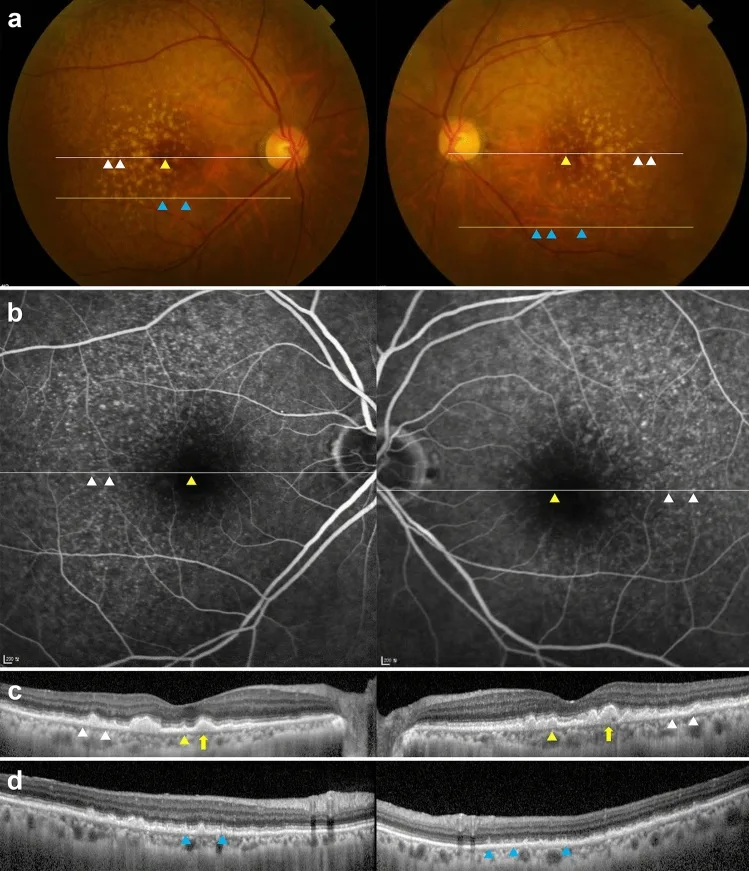
Yoon JM, Shin DH, Kong M, Ham DI. Age-related macular degeneration eyes presenting with cuticular drusen and reticular pseudodrusen. Sci Rep. 2022;12:5681. Figure 1. PMID: 35383241; PMCID: PMC8983695; DOI: 10.1038/s41598-022-09608-9. License: CC BY 4.0.
Fundus photography, fluorescein angiography, and OCT show cuticular drusen, soft drusen, large drusen, and subretinal drusenoid deposits. This is a case with coexisting cuticular drusen and RPD, not a typical example of overall AMD, but an image to understand the appearance of drusen-related lesions.
Yellow-white small round elevated lesions seen in the macula, consisting of polymorphous material (membranous debris, unesterified cholesterol, complement, etc.) accumulated between the RPE basement membrane and the inner collagenous layer of Bruch’s membrane. They are considered the origin of chronic inflammation, which is the core of AMD pathology.
Hard drusen: Less than 63 μm in longest diameter. Well-defined borders. Not included in early AMD alone, but if numerous, may increase the risk of developing AMD.
Soft drusen: 63 μm or more in longest diameter. Ill-defined borders. Closely associated with the development of AMD.
Subretinal drusenoid deposits (reticular pseudodrusen): Located above the RPE, closely associated with atrophic AMD and RAP (type 3 MNV)1).
Type 1 MNV: OCT shows a double layer sign (irregular elevation of the RPE with internal medium reflectivity). It is divided into low, flat lesions and fibrovascular PED with dome-shaped elevation of the RPE. The latter is particularly refractory to treatment1).
Type 2 MNV: Detected on OCT as a medium to high reflectivity structure above the RPE. It is often accompanied by fibrin deposition1).
Type 3 MNV (RAP): Common in patients with bilateral soft drusen. OCT shows cystoid macular edema and PED with a bump sign1).
PCV: Polypoidal lesions are associated with the edge of type 1 MNV. On ophthalmoscopy, they appear as orange-red elevated lesions, and diagnosis is confirmed by ICGA1).
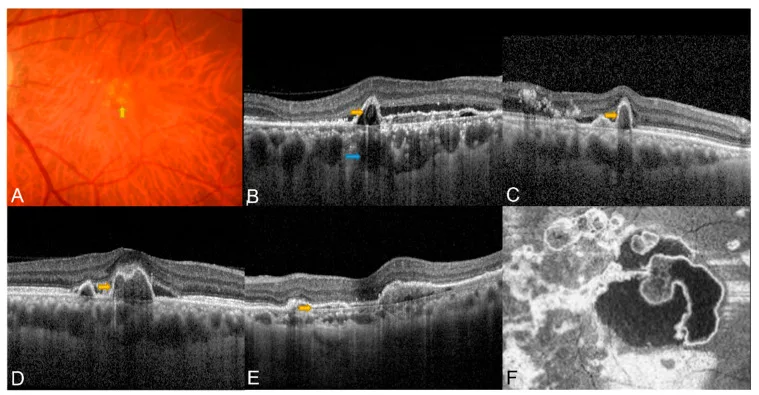
Zhao J, Chandrasekaran PR, Cheong KX, Wong M, Teo K. New Concepts for the Diagnosis of Polypoidal Choroidal Vasculopathy. Diagnostics (Basel). 2023;13(10):1680. Figure 1. PMID: 37238165; PMCID: PMC10216902; DOI: 10.3390/diagnostics13101680. License: CC BY 4.0.
PCV shows orange-red nodules, sub-RPE ring-like lesion, sharp-peaked or thumb-like PED, notched/multilobular PED, double-layer sign, and complex RPE elevation on en face OCT. Although OCT findings provide diagnostic clues for PCV, multimodal evaluation including ICGA is important for definitive diagnosis and treatment planning.
Geographic atrophy is a well-demarcated area of RPE atrophy through which choroidal vessels are visible. The lesion begins in the perifoveal area, expands in a horseshoe shape to a ring shape, and progresses to the fovea. The median time to foveal involvement is 2.5 years3). The growth rate is 1.28–2.6 mm²/year; in ranibizumab trial data, GA area increased from an average of 8.07 to 12.05 mm² over 2 years3). Multifocal GA has a faster growth rate than unifocal GA3).
Rapid atrophy progression may occur when a large drusenoid PED regresses. Hyperautofluorescence patterns at the border of the atrophic area on fundus autofluorescence are useful for predicting the rate of progression.
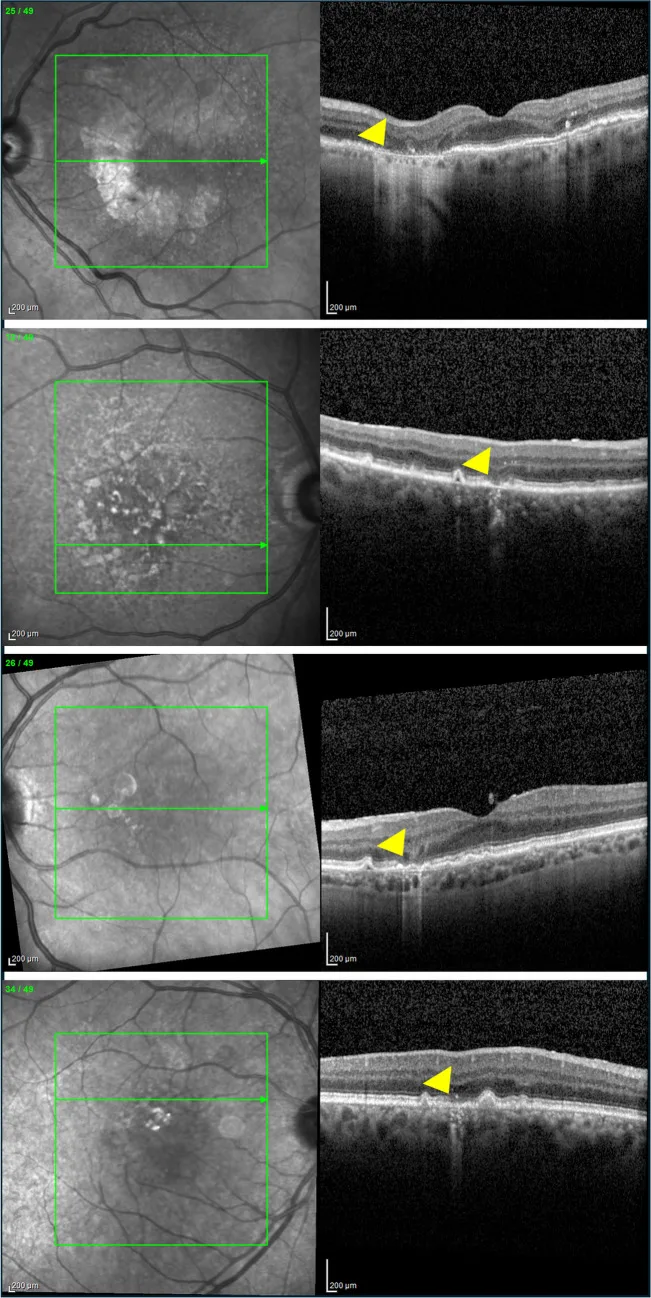
Vallino V, Berni A, Coletto A, Serafino S, Bandello F, Reibaldi M, Borrelli E. Structural OCT and OCT angiography biomarkers associated with the development and progression of geographic atrophy in AMD. Graefes Arch Clin Exp Ophthalmol. 2024;262(11):3421-3436. Figure 1. PMID: 38689123; PMCID: PMC11584504; DOI: 10.1007/s00417-024-06497-8. License: CC BY 4.0.
Examples of cRORA, iRORA, cORA, and iORA as OCT atrophic findings based on the CAM classification. When assessing the presence and progression of GA, in addition to fundus photography and FAF, OCT should be used to confirm RPE and outer retinal atrophy and increased choroidal transmission.
Subretinal and sub-RPE hemorrhage: Bleeding from MNV. Large amounts can cause submacular hematoma and even vitreous hemorrhage.
Serous retinal detachment and serous PED: Due to fluid leakage from MNV.
Hard exudates: Deposited around the macula due to chronic exudation.
Fibrotic scar: A finding in end-stage AMD. Fibrovascular scar tissue forms in the macula1).
QCan age-related macular degeneration be noticed by oneself?
A
The Amsler grid (a self-check sheet with grid lines) can be used to self-detect metamorphopsia and scotomas. However, early stages are often asymptomatic, making regular eye exams essential. Especially when only one eye is affected, it is not uncommon for patients to be unaware in daily life.
AMD is a multifactorial disease, developing from a combination of genetic predisposition and environmental/behavioral factors.
Aging: The greatest risk factor. Prevalence increases sharply after age 752).
Smoking: The most important modifiable risk factor. There is a dose-response relationship, and secondhand smoke is also associated2). Smoking cessation guidance is important for prevention and progression control of AMD1).
Genetic predisposition: CFH and ARMS2/HTRA1 are known as major risk loci. Complement system genes such as C2/CFB, C3, and CFI, as well as lipid metabolism genes like APOE and CETP, are also involved1).
Pachychoroid: Dilatation of choroidal large vessels and increased vascular permeability are considered important as a background for the development of neovascular AMD. In Japanese individuals, drusen are less common (about 30%) than in Western populations, and pachychoroid plays a significant role in the onset1).
Cardiovascular disease, hypertension, obesity: Associated with the risk of developing AMD2).
Diet: High-fat intake increases risk, while intake of long-chain omega-3 fatty acids and green-yellow vegetables reduces risk1). Adherence to a Mediterranean diet reduces the risk of advanced AMD by 41%2).
Sunlight exposure: Ultraviolet and visible light exposure are also pointed out as risk factors2).
Sex: Tends to be more common in men. However, it also occurs in elderly women1).
Family history: Having a first-degree relative with AMD increases the risk of developing the disease2).
AREDS2 supplements (lutein, zeaxanthin, vitamins C and E, zinc, copper) reduce the risk of progression from intermediate to late AMD by about 25% 2). However, their effectiveness for early AMD or primary prevention has not been established. Beta-carotene increases the risk of lung cancer in smokers, so smokers should choose products containing lutein/zeaxanthin 1).
The diagnostic criteria for neovascular AMD are as follows 1).
MNV present in the macula (within 6,000 μm of the fovea) associated with drusen, pachychoroid, or RPE abnormalities
Confirmation of MNV is desirable for a definitive diagnosis, but diagnosis is possible if the presence of MNV can be inferred with sufficient certainty from hemorrhagic changes or fibrous scarring
Exclusion: lesions due to high myopia, angioid streaks, inflammatory diseases, trauma, etc.
The diagnostic criteria for atrophic AMD (geographic atrophy) are considered to be all of the following 1).
OCT (Optical Coherence Tomography): Central examination for AMD diagnosis and follow-up. Detects double layer sign in type 1 MNV, subretinal hyperreflective material in type 2 MNV, bump sign in type 3 MNV, and outer retinal atrophy in geographic atrophy1).
OCTA (Optical Coherence Tomography Angiography): Meta-analysis for MNV detection shows sensitivity 0.87 and specificity 0.97 2). Non-invasive and may have higher detection power for type 1 MNV than FA1).
ICGA (Indocyanine Green Angiography): Useful for confirming PCV diagnosis. Depicts polypoidal lesions around type 1 MNV as nodular hyperfluorescence 1). Due to anaphylaxis risk, consider omitting if diagnosis is possible with other tests.
Fundus Autofluorescence (FAF): Detects geographic atrophy as well-demarcated areas of decreased autofluorescence. Hyperautofluorescence at the border is useful for predicting progression.
Amsler Grid: Screening for metamorphopsia and scotomas. Regular self-checking is recommended 2).
Microperimetry: Quantifies retinal sensitivity. Measures absolute scotoma and sensitivity loss due to geographic atrophy, assessing functional impairment not captured by BCVA 8).
OCT simultaneously evaluates disease stage, MNV type, exudative activity, and the extent of GA atrophy. In AMD-related atrophy, OCT is positioned as the foundational imaging for diagnosis and staging, with fundus photography and FAF used complementarily 11).
When exudative changes from MNV (IRF, SRF, sub-RPE fluid, fibrin, hemorrhage, etc.) are observed, it is judged as “active”1). Noninvasive evaluation with OCT has become mainstream. Since the site of high disease activity in MNV is not necessarily at the fovea, scanning the entire macula for evaluation is recommended1).
OCTA has high accuracy for MNV detection with sensitivity 0.87 and specificity 0.972), and is increasingly used as a non-invasive test. It may be superior to fluorescein angiography especially for detecting type 1 MNV1). However, ICGA remains essential for PCV diagnosis, and OCTA is not a complete replacement.
There is no evidence-based treatment for early AMD2). For intermediate AMD or higher, in addition to smoking cessation and dietary improvement, supplementation based on the AREDS2 formulation is recommended1).
Supplement formulation used in AREDS21):
Vitamin C 500 mg
Vitamin E 400 IU
Lutein/Zeaxanthin 10 mg/2 mg
Zinc oxide 25 mg
Cupric oxide 2 mg
Beta-carotene was replaced with lutein/zeaxanthin because it increases lung cancer risk in smokers1). The AREDS2 formulation reduces the risk of progression from intermediate to late AMD by approximately 25%.
The first-line treatment for neovascular AMD is intravitreal injection of anti-VEGF agents 1). For subfoveal MNV, anti-VEGF monotherapy is recommended as initial treatment.
Maintenance phase: Pro re nata (PRN) dosing. In the MARINA study, visual acuity improved by 6.6 letters compared to a 14.9-letter decline in the sham group 1).
Maintenance phase: Fixed dosing every 2 months or treat-and-extend regimen. If no exudative recurrence, the interval is extended by 2 weeks (up to 3 months); if recurrence occurs, the interval is shortened by 2 weeks 1).
PCV: Polyp regression rate of 40–50%, superior to ranibizumab (20–30%).
Brolucizumab / Faricimab
Brolucizumab: 6 mg injection. Dosing every 8–12 weeks is possible. Caution is needed for intraocular inflammation including retinal vasculitis and vascular occlusion 1).
Faricimab: VEGF-A + Ang-2 bispecific antibody. Administered every 8 to 16 weeks. In the TENAYA/LUCERNE studies, it was non-inferior to aflibercept1)10).
Fixed dosing: Administration continues at regular intervals.
Pro re nata (PRN): Monthly monitoring is performed, and treatment is given if disease activity is observed. The CATT and HARBOR studies reported that the PRN group had worse visual acuity at 2 years compared to the monthly dosing group1).
Treat-and-extend (TAE): The dosing interval is adjusted based on disease activity. The TREX-AMD study showed visual improvement equivalent to monthly dosing. The ALTAIR study (Japanese subjects) confirmed efficacy over 96 weeks with 2-week/4-week adjustment TAE1). Meta-analyses also showed that TAE achieved 2-year visual outcomes equivalent to fixed dosing and significantly better than PRN1).
Laser Photocoagulation for MNV Not Involving the Fovea
For type 2 MNV or PCV lesions that do not involve the fovea, laser photocoagulation of the entire MNV is an option. Irradiation parameters are determined professionally based on lesion size, location, and equipment used. However, laser photocoagulation irreversibly damages the RPE and is not suitable for MNV near the fovea1).
Treatment of PCV (Polypoidal Choroidal Vasculopathy)
Anti-VEGF combined with photodynamic therapy (PDT): The EVEREST II study showed that ranibizumab plus PDT achieved significantly higher polyp regression rates than ranibizumab alone. Combination with anti-VEGF is recommended for safety.
Anti-VEGF monotherapy: Since aflibercept has a favorable polyp regression rate of 40–50%, monotherapy has become more common in recent years.
PDT uses verteporfin, with laser irradiation tailored to the lesion area. After treatment, patients are instructed to avoid photosensitivity reactions for a certain period.
Long-term PDT may worsen macular atrophy, and it is advisable to avoid it in cases with thin choroid or pre-existing macular atrophy. PDT is not recommended for type 3 MNV1).
When the response to anti-VEGF therapy is poor (treatment-resistant cases) or diminishes over time (acquired resistance), switching to another agent may be effective 1). Drug changes may also be considered based on treatment burden (frequency of visits and injections). In end-stage AMD with inactive fibrotic scarring or atrophic changes, aggressive treatment is not indicated, and observation is considered 1).
Treatment of RAP (retinal angiomatous proliferation)
Massive submacular hemorrhage causes acute vision loss. If treated early, pneumatic displacement may improve vision.
Conservative treatment: For small hemorrhages with relatively good vision. If exudation is present, consider anti-VEGF therapy.
Intravitreal gas injection: Injection of 0.3–0.5 mL of sulfur hexafluoride (SF₆) or perfluoropropane (C₃F₈) followed by prone positioning to displace the hemorrhage. tPA may be used concurrently 1).
Vitrectomy: Subretinal tPA injection or displacement of hemorrhage using perfluorocarbon liquid.
The goal of treatment for geographic atrophy is to slow the enlargement of atrophy, not to restore lost vision or eliminate atrophic lesions. Previously, management focused on lifestyle modification, AREDS2, anti-VEGF therapy for incident MNV, and low-vision care. However, on September 19, 2025, avacincaptad pegol sodium (Izaybe intravitreal injection 20 mg/mL) was approved in Japan for the indication of “slowing the progression of geographic atrophy in atrophic age-related macular degeneration” 13).
This drug is administered as 2 mg/0.1 mL avacincaptad pegol sodium intravitreally once monthly for the first 12 months, then every 2 months thereafter. Indication decisions should individually assess lesion location, enlargement rate, fellow eye status, risk of MNV development, injection-related complications, and visit burden 13). If MNV develops during follow-up, anti-VEGF therapy for neovascular AMD should be considered 1).
For patients with progressive vision loss, low-vision care including visual aids such as tinted glasses and magnifiers, as well as support for daily activities, is important 1).
QHow often are anti-VEGF injections needed?
A
The induction phase typically involves three injections at one-month intervals. During the subsequent maintenance phase, the treat-and-extend method (gradually extending intervals) is recommended. The ALTAIR study (Japanese subjects) confirmed efficacy over 96 weeks 1). With faricimab, some cases can maintain intervals of up to 16 weeks 10).
QIs there an effective treatment for atrophic (geographic atrophy) AMD?
A
For geographic atrophy, treatments aimed at slowing lesion enlargement have emerged. In Japan, avacincaptad pegol sodium was approved on September 19, 2025 13). However, it is not a treatment that restores vision; indications are determined after evaluating foveal involvement, MNV complications, injection risks, and visit burden. AREDS2 supplements reduce the risk of progression to late AMD but have not been shown to suppress the progression of geographic atrophy itself. When vision loss progresses, low vision care becomes important.
The pathology of AMD begins with damage to RPE cells. Drusen accumulate between the RPE basement membrane and the inner collagenous layer of Bruch’s membrane. Drusen components include membranous debris, unesterified cholesterol, and complement, serving as a source of chronic inflammation. Oxidative stress, lipid metabolism abnormalities, and activation of the innate immune system are complexly involved, leading to disruption of the homeostasis of the RPE-Bruch’s membrane-choriocapillaris complex. Subsequently, the pathway diverges into two.
Atrophic pathway: Inflammation and oxidative stress cause progressive RPE degeneration and atrophy, resulting in geographic atrophy of the photoreceptor-RPE-choriocapillaris complex. First, the outer retinal layers (RPE and ellipsoid zone) are lost, and in advanced cases, the choriocapillaris also atrophies 3).
Exudative pathway: New blood vessels (MNV) form beneath the retina or RPE, leading to hemorrhage and exudation. In intraocular fluid, IL-6, IL-8, MCP-1, and VEGF are elevated 5).
Aged RPE cells exhibit a senescence-associated secretory phenotype (SASP), with increased expression of SA-β-gal, p53, p21, and p16 7). This senescent RPE phenotype is consistent with findings in patients with atrophic AMD, and selective elimination by senolytics is attracting attention as a therapeutic target.
Genetic polymorphisms in CFH, C3, and ARMS2 are associated with susceptibility to AMD 2). Dysregulation of complement pathways (classical, alternative, and lectin pathways) drives the expansion of geographic atrophy3). Inhibiting complement C3 is expected to suppress the entire terminal pathway downstream of C5, while inhibiting C5 is expected to prevent the formation of the membrane attack complex (MAC).
Anegondi et al. (2025) analyzed data from the lampalizumab trial and showed that faster growth rates of geographic atrophy lead to faster BCVA decline, with approximately 75% losing 5 or more letters, approximately 50% losing 10 or more letters, and approximately 25% losing 15 or more letters over 2 years 3).
Pachychoroid is a condition characterized by dilation of large choroidal vessels (pachyvessels) and increased choroidal vascular permeability 1). Central serous chorioretinopathy (CSC) is a representative pachychoroid disease, and MNV arising from CSC or pachychoroid pigment epitheliopathy (PPE) is called pachychoroid neovasculopathy (PNV). The CFH gene has also been reported to be involved in the development of pachychoroid and CSC1).
Ribatti et al. (2024) reported that tryptase secreted by choroidal mast cells induces Bruch’s membrane degradation, leading to RPE death, and the release of VEGF-A, FGF-2, IL-8, and NGF promotes angiogenesis 5).
Non-exudative MNV is biologically active even when asymptomatic, with persistent area enlargement 4).
Wang et al. (2023) reported in an SS-OCTA study of 45 eyes that growing MNV (area increase ≥50%) had a significantly shorter time to exudative conversion than non-growing MNV (13.60 months vs. 31.11 months, HR 12.51), and smoking history was significantly correlated with MNV area increase (P=0.021) 4).
Geographic atrophy often begins around the fovea, and the fovea shows relative resistance to atrophy 3). This results in horseshoe-shaped or ring-shaped GA. The median time to foveal involvement is 2.5 years, during which high-contrast visual acuity is preserved, but daily visual functions such as dark-adapted sensitivity and reading speed are impaired early 8).
7. Latest treatments, research, and future perspectives
In geographic atrophy, drugs targeting the complement pathway have been clinically implemented to slow lesion progression. Pegcetacoplan in the OAKS/DERBY trials and avacincaptad pegol in the GATHER2 trial have been reported to suppress the enlargement of GA lesions9)12). In Japan, avacincaptad pegol sodium was approved in 202513).
Pegcetacoplan (SYFOVRE): C3 inhibitor. 15 mg/0.1 mL intravitreal injection every 25–60 days. In the OAKS trial (637 patients) and DERBY trial (621 patients), it reduced the growth rate of geographic atrophy by up to 21%9).
Avacincaptad pegol (Izervay): C5 inhibitor. In the GATHER2 trial (n=448), it reduced GA growth rate by 14% compared to sham at 12 months 12). In Japan, it is approved as a formulation administered intravitreally at 2 mg/0.1 mL once monthly from the first dose through 12 months, then every 2 months thereafter 13).
However, neither drug showed a significant difference in trials where visual acuity improvement was a prespecified endpoint, leaving the “structure-function dissociation” as a remaining challenge3)8). The European Medicines Agency (EMA) required demonstration of functional benefit and did not approve pegcetacoplan8).
On the other hand, not all complement system and visual cycle targeted drugs have shown efficacy, and careful evaluation from both structural and functional perspectives continues for the pharmacological treatment of geographic atrophy8).
In a review by Dinah et al. (2026), BCVA was found to insufficiently capture the functional impact of geographic atrophy, and microperimetry, low-luminance visual acuity (LLVA), and reading speed were recommended as alternative measures8). Establishing a comprehensive, multimodal functional assessment will be key for future clinical trials.
Novel anti-VEGF drugs and sustained-release devices
High-dose aflibercept (8 mg): The PULSAR trial demonstrated that administration every 16 weeks is possible2). This is expected to reduce the treatment burden.
Ranibizumab sustained-release implant (port delivery system): The Archway trial reported that refill exchange every 24 weeks achieved efficacy equivalent to monthly injections2).
Biosimilars: Multiple biosimilars of ranibizumab and aflibercept have been approved2).
Ji et al. (2025) reported a case of dry AMD treated with photobiomodulation therapy (red to near-infrared light 650–1,300 nm)6). Over 8 months, the drusen area in the right eye decreased by 58% and completely disappeared in the left eye. Visual acuity improved from 20/30 to 20/20 in the left eye and remained 20/25 in the right eye. However, this is a case report, and further validation is needed to establish it as a standard treatment.
Chung & Kim (2022) reported that the MDM2 inhibitor Nutlin-3a is a promising novel approach for selectively eliminating senescent RPE cells7). The development of mitochondria-specific senolytics remains a future challenge.
Stem cell therapy using RPE cell transplantation is in the research stage, with multiple trials ongoing. Gene therapy targeting complement factors is also being investigated.
QShould I undergo genetic testing for age-related macular degeneration?
A
Genetic polymorphisms in CFH, ARMS2, and C3 are associated with the risk of developing AMD. Genetic testing may enable prediction of prognosis, such as the development of AMD in the fellow eye1). However, at present, treatment strategies based on genetic testing are not standardized2), and routine testing is not recommended.
Atrophic AMD progresses slowly, but when geographic atrophy reaches the fovea, visual acuity drops to 0.1 or less. The median time to legal blindness (visual acuity 20/200 or worse) has been reported as 6.2 years3). Analysis of lampalizumab trial data showed that mean BCVA decreased from 66 to 57 letters (approximately 20/50 to 20/80 equivalent) over 2 years3).
Faster growth of geographic atrophy is associated with more rapid BCVA decline; in eyes with a single subfoveal lesion, the fastest-growing group showed a loss of approximately 4 lines (17.75 letters) over 2 years3). In contrast, the slowest-growing group lost only 1.69 letters over 2 years. Even when the fovea is preserved, scotopic sensitivity, contrast sensitivity, and reading speed are impaired early, so visual acuity alone underestimates functional impact8).
Additionally, there is a certain probability of developing MNV and transitioning to neovascular AMD, leading to more severe vision loss.
Control of MNV with anti-VEGF drugs has significantly improved visual prognosis. In the 5-year follow-up of the CATT study, 50% of eyes achieved visual acuity of 20/40 or better15). However, if left untreated, severe vision loss occurs, leaving fibrotic or atrophic scars in the macula. In cases with massive hemorrhage from MNV, extensive visual field defects and more severe visual impairment, including complete blindness, can occur.
Complete cure of MNV is impossible, and without appropriate treatment and long-term management, it can easily lead to irreversible vision loss 1). Even if MNV activity temporarily subsides, it may recur over the long term, and repeated exudation can lead to atrophic changes or fibrous scarring. Considering that MNV also occurs at a high rate in the fellow eye, continued treatment and regular monitoring are essential 1). Active low-vision care is recommended for patients with severe visual impairment.
Vemulakonda GA, Bailey ST, Kim SJ, Kovach JL, Lim JI, Ying GS, et al; American Academy of Ophthalmology Preferred Practice Pattern Retina/Vitreous Committee. Age-Related Macular Degeneration Preferred Practice Pattern®. Ophthalmology. 2025;132(4):P1-P74. doi:10.1016/j.ophtha.2024.12.018. PMID:39918524.
Anegondi N, Steffen V, Sadda SR, Schmitz-Valckenberg S, Tufail A, Csaky K, et al. Visual Loss in Geographic Atrophy: Learnings from the Lampalizumab Trials. Ophthalmology. 2025;132(4):420-430. doi:10.1016/j.ophtha.2024.11.017. PMID:39581330.
Wang Y, Sun J, Wu J, Jia H, Feng J, Chen J, et al. Growth of nonexudative macular neovascularization in age-related macular degeneration: an indicator of biological lesion activity. Eye (London, England). 2023;37(10):2048-2054. doi:10.1038/s41433-022-02282-1. PMID:36434285; PMCID:PMC10333345.
Ribatti D, Dammacco R. Mast cells in human choroid and their role in age-related macular degeneration (AMD). Clin Exp Med. 2024;24(1):98. doi:10.1007/s10238-024-01361-9. PMID:38727918; PMCID:PMC11087330.
Ji PX, Pickel L, Berger AR, Sivachandran N. Improvement in Dry Age-Related Macular Degeneration with Photobiomodulation. Case reports in ophthalmology. 2025;16(1):155-162. doi:10.1159/000543971. PMID:40241926; PMCID:PMC11879149.
Chung H, Kim C. Nutlin-3a for age-related macular degeneration. Aging. 2022;14(14):5614-5616. doi:10.18632/aging.204187. PMID:35849498; PMCID:PMC9365563.
Dinah C, Esmaeelpour M, Rachitskaya AV, De Salvo G, Munk MR. Functional endpoints in patients with geographic atrophy: What to consider when designing a clinical trial. Prog Retin Eye Res. 2026;110:101421. doi:10.1016/j.preteyeres.2025.101421. PMID:41352581.
Heier JS, Lad EM, Holz FG, et al. Pegcetacoplan for the treatment of geographic atrophy secondary to age-related macular degeneration (OAKS and DERBY): two multicentre, randomised, double-masked, sham-controlled, phase 3 trials. Lancet. 2023;402:1434-1448. doi:10.1016/S0140-6736(23)01520-9. PMID:37865470.
Khanani AM, Kotecha A, Chang A, Chen SJ, Chen Y, Guymer R, et al; TENAYA and LUCERNE Investigators. TENAYA and LUCERNE: Two-Year Results from the Phase 3 Neovascular Age-Related Macular Degeneration Trials of Faricimab with Treat-and-Extend Dosing in Year 2. Ophthalmology. 2024;131(8):914-926. doi:10.1016/j.ophtha.2024.02.014. PMID:38382813.
Sadda SR, Guymer R, Holz FG, Schmitz-Valckenberg S, Curcio CA, Bird AC, et al. Consensus Definition for Atrophy Associated with Age-Related Macular Degeneration on OCT: Classification of Atrophy Report 3. Ophthalmology. 2018;125(4):537-548. doi:10.1016/j.ophtha.2017.09.028. PMID:29103793; PMCID:PMC11366072.
Khanani AM, Patel SS, Staurenghi G, Tadayoni R, Danzig CJ, Eichenbaum DA, et al; GATHER2 trial investigators. Efficacy and safety of avacincaptad pegol in patients with geographic atrophy (GATHER2): 12-month results from a randomised, double-masked, phase 3 trial. Lancet. 2023;402(10411):1449-1458. doi:10.1016/S0140-6736(23)01583-0. PMID:37696275.
Zhao J, Chandrasekaran PR, Cheong KX, Wong M, Teo K. New Concepts for the Diagnosis of Polypoidal Choroidal Vasculopathy. Diagnostics (Basel). 2023;13(10):1680. doi:10.3390/diagnostics13101680. PMID:37238165; PMCID:PMC10216902.
Comparison of Age-related Macular Degeneration Treatments Trials (CATT) Research Group, Maguire MG, Martin DF, Ying GS, Jaffe GJ, Daniel E, Grunwald JE, et al. Five-Year Outcomes with Anti-Vascular Endothelial Growth Factor Treatment of Neovascular Age-Related Macular Degeneration: The Comparison of Age-Related Macular Degeneration Treatments Trials. Ophthalmology. 2016;123(8):1751-1761. doi:10.1016/j.ophtha.2016.03.045. PMID:27156698; PMCID:PMC4958614.
Copy the article text and paste it into your preferred AI assistant.
Article copied to clipboard
Open an AI assistant below and paste the copied text into the chat box.