Multifocal choroiditis with panuveitis (MFCwP), also called idiopathic multifocal choroiditis (IMFC), is an idiopathic inflammatory disease that presents with multiple inflammatory lesions at the level of the retinal pigment epithelium (RPE) and choriocapillaris. It recurs with inflammatory episodes and occurs bilaterally, simultaneously or sequentially.
In 1984, Deutsch and Tessler reported 28 cases as “pseudo-POHS.” In 1986, Morgan and Shatz described 11 cases as “recurrent multifocal choroiditis,” noting vitreous inflammation not seen in POHS patients. MCP and PIC (punctate inner choroidopathy) are both subtypes of white dot syndromes (WDS), belonging to a group of inflammatory diseases primarily affecting the outer retina, choriocapillaris, and choroid1). It has been suggested that both diseases may represent a spectrum of the same disease 1).
The Uveitis Clinical Practice Guidelines (Jpn J Ophthalmol 2019;123(6):635-696) list “multifocal choroiditis with panuveitis” as a differential diagnosis of PIC5), and the presence of vitritis is an important distinguishing feature from PIC.
QHow is POHS different from MCP?
A
The biggest difference is the presence or absence of vitritis. POHS is not accompanied by vitritis, but in MCP, vitritis is usually seen in one or both eyes. In addition, mild anterior chamber inflammation may also be observed in MCP. Furthermore, MCP is negative for histoplasma antibodies and can occur even in patients without a history of residence in histoplasma-endemic areas (such as the Ohio River Valley in the United States), which also serves as a clue for differentiation.
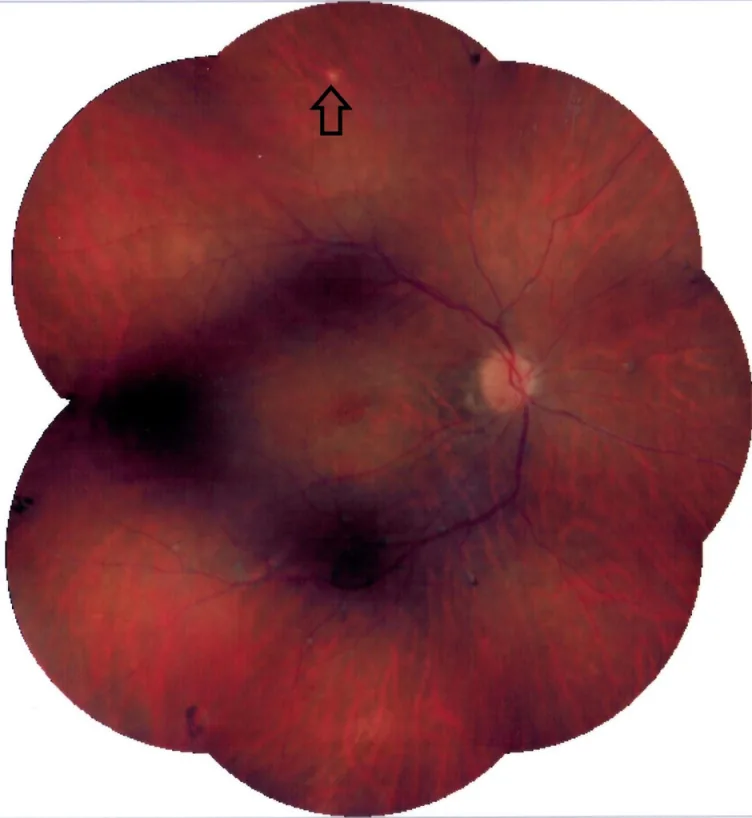
Soheilian M, et al. Presumed Tubercular Multifocal Choroiditis. J Ophthalmic Vis Res. 2024. Figure 1. PMCID: PMC11795012. License: CC BY.
Composite fundus photograph showing multiple black chorioretinal scars around the optic disc and near the inferior arcade. A pale yellowish-white lesion is also seen in the superior mid-periphery, indicating the coexistence of active lesions and scar lesions seen in multifocal choroiditis.
Floaters: Due to vitritis. One of the most common initial symptoms
Decreased vision/blurred vision: Due to macular edema, choroidal neovascularization, or extension of lesions to the fovea
Photopsia: Due to stimulation from active inflammatory lesions
Metamorphopsia: Distortion due to macular lesions or edema
Scotoma: Visual field defect corresponding to inflammatory lesions
Photophobia/ocular discomfort: Varies depending on the degree of anterior chamber inflammation
The presence of anterior chamber inflammation (mild) and vitreous inflammation is an important differentiating point from PIC5). In myopic patients, evaluation of vitritis can be difficult, and OCT-A or ICG findings are useful as auxiliary diagnostics 7).
In long-term cohorts, CNV is the main cause of vision loss, and cystoid macular edema and epiretinal membrane are also associated with vision loss 9). For assessment of vision loss risk, pay attention to CNV, atrophic scars involving the fovea, and dense macular lesions.
The etiology of MCP is unknown. There is a hypothesis that a preceding infection stimulates an immune response, but no specific pathogen has been identified.
Epidemiological features:
More common in white women
Mean age at onset 30 years (range: 6–69 years)
Most patients are myopic
Affects healthy individuals without known systemic or ocular diseases
Genetic predisposition:
MCP is associated with haplotypes of IL-10 and tumor necrosis factor (TNF). A hypothesis of genetic predisposition plus environmental factors as a disease within the AZOOR complex has been proposed.
Pathophysiological hypothesis:
Inflammatory lesions begin at the level of the retinal pigment epithelium and choriocapillaris. Antigen sensitization may occur in the retinal photoreceptors and retinal pigment epithelium by an exogenous antigen, potentially compromising the integrity of Bruch’s membrane. This creates space for choroidal neovascular membranes to develop, and choroidal neovascularization can occur in up to 60% of patients.
MCP is a clinical diagnosis and a diagnosis of exclusion. It is essential to exclude infectious, malignant, and systemic diseases. The uveitis clinical practice guidelines also state “no established diagnostic criteria, characteristic findings and exclusion diagnosis” 5).
Diagnostic requirements for MCP:
Multiple small white spots predominantly in the posterior pole of both eyes
Presence of anterior chamber inflammation or vitritis (essential for differentiation from PIC)
Exclusion of infectious and systemic diseases (syphilis, tuberculosis, sarcoidosis, etc.)
Exclusion of malignant diseases (lymphoma, metastasis)
Imaging differentiation between MCP and PIC:
In differentiating MCP/IMFC from PIC, it is important to organize findings characteristic of myopic CNV and PIC. MCP lesions are larger (45–350 μm) and tend to show extensive hypofluorescence on ICG. PIC lesions are smaller (125–250 μm), confined to the posterior pole, and not associated with vitritis7).
In tuberculosis-endemic areas (e.g., India), up to 40% of multifocal choroiditis may be associated with ocular tuberculosis3), and may be observed as sub-RPE inflammatory lesions on OCT3).
QHow is multifocal choroiditis differentiated from tuberculosis?
A
Multimodal imaging is useful for differentiation. In tuberculous multifocal choroiditis, OCT may show disruption of the external limiting membrane and focal loss of the ellipsoid zone overlying sub-RPE inflammatory lesions3). Evaluation should combine QuantiFERON-TB Gold testing and imaging. In tuberculosis-endemic areas or with a history or exposure to tuberculosis, active exclusion testing should be performed.
Treatment is selected based on the degree of inflammation, active lesions, complications, and visual acuity loss. Cystoid macular edema, dense vitritis, or choroidal neovascular membrane formation are indications for treatment.
Oral steroids: First-line treatment. For active lesions with vitritis and anterior chamber inflammation, systemic steroids are administered, primarily prednisolone 0.5–1 mg/kg/day, tapered according to inflammation resolution 5).
Local steroids:
Triamcinolone acetonide (Kenacort-A): Sub-Tenon or intravitreal injection. Duration of action 2–3 months.
For refractory, recurrent, or steroid-dependent cases, immunomodulatory agents are considered. Maintenance therapy with cyclosporine, azathioprine, or mycophenolate mofetil (MMF) is used, and anti-TNFα agents (adalimumab) are considered for refractory cases 5).
In a survey by an international research group (n=221 uveitis specialists), the first-choice conventional immunomodulatory agent for multifocal choroiditis-PIC spectrum disease was methotrexate (39.4%), and the first-choice biologic was adalimumab (95.5%) 4).
From the perspective of long-term visual prognosis, inflammation control and CNV management are important. In the Johns Hopkins MFCPU cohort, posterior pole complications such as CNV, cystoid macular edema, and epiretinal membrane were associated with visual acuity loss 9). A comparative study by Kedhar et al. also showed that MFCPU has more inflammatory complications such as cataracts, cystoid macular edema, and epiretinal membrane than PIC8).
Intravitreal anti-VEGF therapy is used for active choroidal neovascularization and macular edema. Anti-VEGF alone often insufficiently controls CNV with an inflammatory background, and combination with steroid therapy and immunomodulatory therapy is recommended.
Inflammatory lesions begin at the level of the retinal pigment epithelium and choriocapillaris, and it is hypothesized that antigen sensitization occurs in the retinal pigment epithelium by exogenous antigens.
Both MCP and PIC involve the outer retina, choriocapillaris, and choroid, and may represent a spectrum of the same disease 1). MCP is a chronic, bilateral, recurrent inflammatory disease characterized by posterior lesions with anterior uveitis and vitritis, whereas PIC differs by the absence of vitritis and anterior chamber inflammation 1). In a redefinition using multimodal imaging by Spaide et al., MCP and PIC are unified as “primary inflammatory diseases of the choriocapillaris plate,” with the presence or absence of vitritis as the main distinguishing feature 6).
On OCT angiography (OCT-A), distinct areas of decreased blood flow at the choriocapillaris level correspond to active inflammatory lesions 1), supporting the possibility that outer retinal changes are secondary to primary choroidal involvement. OCT-A is increasingly useful both for monitoring active inflammation and detecting CNV.
Inflammation disrupts the integrity of Bruch’s membrane, which serves as a foothold for the development of choroidal neovascular membranes. In MCP, up to 60% of patients may develop choroidal neovascularization. CNV, as inflammatory CNV, responds to anti-VEGF therapy, but control of the underlying inflammation is essential.
Genetic factors such as associations with haplotypes of IL-10 and tumor necrosis factor have been reported, but the exact mechanism remains unclear.
OCT angiography shows clear decreased blood flow in the choriocapillaris of MCP lesions, corresponding to active inflammatory lesions 1). It is also applied for monitoring choroidal vascular changes after treatment, and may allow non-invasive assessment of disease activity without fluorescein angiography.
OCT angiography has been shown to delineate areas of decreased choriocapillaris blood flow corresponding to retinal pigment epithelial elevations on optical coherence tomography and hypofluorescent spots on indocyanine green angiography, deepening pathophysiological understanding 1).
Redefinition of Disease Spectrum and Personalized Treatment
Spaide et al. redefined MFCwP and PIC using multimodal imaging, suggesting they may be on the same spectrum 6). More precise disease classification and development of personalized treatment are progressing. Criteria for multimodal imaging to differentiate myopic CNV from MCP/PICCNV have also been proposed 7), and appropriate application of anti-VEGF therapy is expected.
Testi I, Modugno RL, Pavesio C. Multimodal imaging supporting the pathophysiology of white dot syndromes. Journal of ophthalmic inflammation and infection. 2021;11(1):32. doi:10.1186/s12348-021-00261-3. PMID:34529201; PMCID:PMC8446150.
Kaza H, Gala JM, Rani PK. Subfoveal retinal pigment epithelium inflammatory lesion presenting as a sign of reactivation of tubercular multifocal choroiditis. BMJ case reports. 2021;14(5). doi:10.1136/bcr-2020-240280. PMID:34031072; PMCID:PMC8149327.
Branford JA, et al. Practice patterns of systemic immunomodulatory drug treatment for non-infectious uveitis: an international study. Br J Ophthalmol. 2025;109:482-489.
Spaide RF, Goldberg N, Freund KB. Redefining multifocal choroiditis and panuveitis and punctate inner choroidopathy through multimodal imaging. Retina (Philadelphia, Pa.). 2013;33(7):1315-24. doi:10.1097/IAE.0b013e318286cc77. PMID:23584703.
Kedhar SR, Thorne JE, Wittenberg S, Dunn JP, Jabs DA. Multifocal choroiditis with panuveitis and punctate inner choroidopathy: comparison of clinical characteristics at presentation. Retina. 2007;27(9):1174-1179. doi:10.1097/IAE.0b013e318068de72.
Thorne JE, Wittenberg S, Jabs DA, Peters GB, Reed TL, Kedhar SR, Dunn JP. Multifocal choroiditis with panuveitis: incidence of ocular complications and of loss of visual acuity. Ophthalmology. 2006;113(12):2310-2316. doi:10.1016/j.ophtha.2006.05.067.
Copy the article text and paste it into your preferred AI assistant.
Article copied to clipboard
Open an AI assistant below and paste the copied text into the chat box.