Acute posterior multifocal placoid pigment epitheliopathy (APMPPE) is an acute inflammatory disease of both eyes first reported by Gass in 1968 10). It is characterized by multiple disc-shaped white spots at the level of the deep retina to the retinal pigment epithelium (RPE) in the posterior pole of both eyes.
According to the Uveitis Clinical Practice Guidelines (Journal of Japanese Ophthalmological Society 2019;123(6):635-696), it is classified as non-infectious posterior uveitis predominantly involving the fundus, with clinical features of bilateral involvement, acute onset, and transient course 1).
The pathogenesis is thought to be occlusive vasculitis due to a delayed-type hypersensitivity reaction (type IV allergy) occurring in the afferent arterioles of the choriocapillaris. Viral infections (influenza, mumps, etc.) are suspected triggers, but details remain unclear.
The peak age of onset is in the 20s to 30s (average 25 years), with no gender difference 1). Bilateral involvement is common. Preceding flu-like symptoms are reported in more than half of cases 1). Rare associations with systemic vasculitis, nephropathy, meningoencephalitis, and thyroiditis have been reported 1).
QDoes APMPPE only occur in young people?
A
The typical age of onset is young adults under 40 years; it is rare in the elderly and children. If similar lesions are found in patients over 40, differentiation from serpiginous choroiditis (geographic choroiditis) is important.
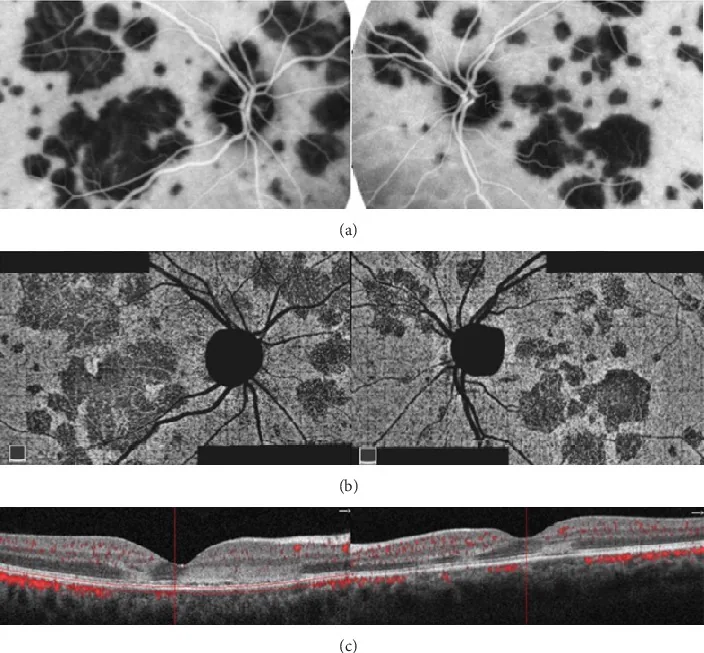
Oliveira MA, et al. Management of Acute Posterior Multifocal Placoid Pigment Epitheliopathy (APMPPE): Insights from Multimodal Imaging with OCTA. Case Rep Ophthalmol Med. 2020. Figure 5. PMCID: PMC7094199. License: CC BY.
Multiple geographic and patchy lesions are seen at the posterior pole of both eyes, appearing as hypofluorescent areas on ICGA and corresponding to areas of decreased choriocapillaris flow on OCTA. OCT shows hyperreflective changes from the outer plexiform layer to the RPE, representing typical findings of APMPPE.
Multiple gray-white (cream to white) disc-shaped spots appear in the deep retina to RPE level at the posterior pole of both eyes. The lesions are well-defined, about 1/4 to 1/2 disc diameter in size, nearly uniform, ranging from a few to many, and show little tendency to coalesce or enlarge. Mild optic dischyperemia and edema, and mild vitreous cells may be present 1). The spots are larger than those in multiple evanescent white dot syndrome (MEWDS), which is a distinguishing feature.
Acute Phase Findings
Fundus white spots: Multiple well-defined gray-white disc-shaped spots of 1/4 to 1/2 disc diameter at the posterior pole. They represent ischemic edema and opacity of the RPE and outer retina due to choriocapillaris occlusion.
Outer retinal damage: OCT shows hyperreflective disruption of the ellipsoid zone (IS/OS line) 1). Destruction of the ellipsoid zone causes subjective symptoms 2).
FAF (fundus autofluorescence): In the acute phase, lesions appear as hypoautofluorescent or hyperautofluorescent areas. OCT and autofluorescence findings correspond closely 9).
Remission Phase Findings
Resolution of white spots: The white spots regress from the center over 7 to 12 days, disappearing with mild depigmentation changes.
OCT recovery: The ellipsoid zone may recover over several months, but thinning of the photoreceptor layer may persist 1).
Chorioretinal atrophy: In some cases, mild chorioretinal atrophic spots may remain1).
QDo the white spots in APMPPE disappear?
A
In many cases, the white spots regress 7–12 days after onset and disappear leaving depigmentation. Visual prognosis is usually good and recurrence is rare. However, progression may be seen in cases that transition to serpiginous choroiditis, so regular follow-up is necessary.
The underlying mechanism is thought to be occlusive vasculitis due to a delayed-type hypersensitivity reaction (type IV allergy) in the afferent arterioles of the choriocapillaris. OCT angiography (OCT-A) shows flow voids at the choriocapillaris level in acute lesions, supporting choriocapillaris ischemia as a core component of the pathology3). Klufas et al. reported that OCT-A detected choriocapillaris flow voids with high agreement with FA and ICGA in three placoid chorioretinitis diseases (APMPPE, PPM, and RPC)4).
Some cases develop after preceding flu-like symptoms (influenza, mumps, etc.), upper respiratory tract infection, or vaccination.
Associations with systemic vasculitis (cerebral vasculitis), nephropathy, polyarteritis nodosa, and thyroiditis have been reported1).
QDoes APMPPE increase the risk of stroke?
A
Although rare, cases of APMPPE complicated by central nervous system vasculitis have been reported. If neurological symptoms (severe headache, altered consciousness, paralysis) appear, emergency brain MRI/MRA should be performed, and coordination with a neurologist is necessary.
The diagnosis of APMPPE is based on characteristic fundus findings and fluorescein angiography (FA/ICGA) findings. Multimodal imaging allows a multifaceted evaluation of the pathology 2).
The “fluorescence reversal phenomenon” seen on FA—early hypofluorescence followed by late hyperfluorescence—is the most characteristic finding of APMPPE. It is interpreted as early blockage of dye inflow into the choriocapillaris (due to occlusive vasculitis) and late leakage from surrounding areas causing hyperfluorescence 1). On ICGA, hypofluorescence persists from early to late phases, more directly reflecting choriocapillaris ischemia 5).
OCT-A is a non-invasive imaging modality that can evaluate blood flow impairment in the choriocapillaris in APMPPE. Furino et al. reported that OCT-A can detect choriocapillaris flow voids in acute APMPPE lesions with high concordance with FA and ICGA8). In the convalescent phase, reduction of flow voids along with improvement in visual function has been observed, making it useful as a biomarker for activity monitoring.
Persistent placoid maculopathy (PPM) / relentless placoid chorioretinitis (RPC): Similar to APMPPE, there is debate on reclassification within the “placoid chorioretinitis spectrum” 4)7)
QHow do you differentiate APMPPE from MEWDS?
A
Three key points for differentiation are lesion size, FA findings, and bilaterality. APMPPE white spots are larger than MEWDS (1/4 to 1/2 disc diameter), often bilateral, and show the reversal phenomenon (early hypofluorescence to late hyperfluorescence) on FA. MEWDS is often unilateral, with smaller and more widespread white spots, and shows early hyperfluorescence on FA1).
There is a strong tendency for spontaneous resolution, and many cases recover naturally without specific treatment 1). In mild cases, observation is the basic approach. Jones (1995) long-term follow-up report also showed that many cases ultimately recovered good visual acuity10).
The following treatments are considered when visual acuity loss is significant, papillitis is present, or there are lesions near the macula.
Prednisolone tablets (5 mg): Start at 30 mg/day and taper over 2 weeks to 1 month
Calnacrin tablets (kallidinogenase 25–50 units): 3 tablets in 3 divided doses (used as a choroidal microcirculation improver)
In cases that progress to serpiginous choroidopathy or are complicated by central nervous system vasculitis, consider steroid pulse therapy (high-dose intravenous methylprednisolone) or immunosuppressive drugs 1). If choroidal neovascularization (CNV) occurs, consider intravitreal anti-VEGF injection, but this is a rare complication. In cases that progress to persistent placoid maculopathy (PPM), long-term management may be required, as Kolomeyer and Brucker pointed out in their systematic review 7).
QIs steroid treatment always necessary?
A
In mild cases, natural recovery occurs with observation alone. Steroid therapy is considered when visual acuity loss is significant, inflammation near the optic disc is severe, or central nervous system symptoms are present. The Uveitis Clinical Practice Guidelines also state that “natural recovery without specific treatment” is the basic policy 1).
The pathology of APMPPE is understood as ischemic changes centered on occlusion of the choriocapillaris.
It is presumed that the underlying cause is occlusive vasculitis due to a delayed-type hypersensitivity reaction (type IV allergy) occurring in the afferent arterioles of the choriocapillaris. Occlusion → ischemic changes (edema, opacification) of the RPE and outer retina → formation of disc-shaped white lesions. Mrejen et al. showed that choroidal lesions extend to deeper layers, suggesting possible involvement not only of the choriocapillaris but also of medium and large vessels 3).
On OCT-A, flow voids at the inner choroid level are observed, and choriocapillaris ischemia is consistently recognized as the pathological basis of the disease group known as the “placoid disorder spectrum” (including persistent placoid maculopathy and relentless placoid chorioretinitis), similar to APMPPE 4). Klufas et al. reported that choriocapillaris flow voids on OCT-A show a common pattern among the three diseases, supporting the concept of the placoid chorioretinitis spectrum.
Mechanism of fluorescence reversal: In the early phase of angiography, dye inflow into the choriocapillaris is impaired, resulting in hypofluorescence; in the late phase, dye leaks from surrounding normal tissue, turning into hyperfluorescence. The fact that ICGA consistently shows hypofluorescence also reflects occlusive changes in the choriocapillaris5). FAF can noninvasively assess the distribution of RPE damage and shows a high correlation with OCT findings 9).
APMPPE after COVID-19 infection/vaccination: Cases of acute APMPPE-like lesions appearing after infection have been reported, drawing attention to the relationship with virus-induced immune responses.
Complication with cerebral vasculitis: Recommendations for brain MRI/MRA in cases with neurological symptoms are increasing. Multiple cases of APMPPE complicated by stroke or cerebral vasculitis have been reported, emphasizing the importance of systemic monitoring beyond ocular symptoms 6).
Advances in multimodal imaging: Monitoring of choriocapillaris flow voids by OCT-A may serve as a biomarker for activity assessment 8). Being noninvasive and repeatable, it is becoming an important modality complementing FA and ICGA.
Reclassification of disease types: An integrated understanding as the “placoid chorioretinitis spectrum” including persistent placoid maculopathy and relentless placoid chorioretinitis is progressing 4). Mirza and Jampol (2012) organized the characteristics of relentless placoid chorioretinitis as an independent disease concept and discussed its continuity with APMPPE 6).
Testi I, Modugno RL, Pavesio C. Multimodal imaging supporting the pathophysiology of white dot syndromes. Journal of ophthalmic inflammation and infection. 2021;11(1):32. doi:10.1186/s12348-021-00261-3. PMID:34529201; PMCID:PMC8446150.
Claudio Furino, Zaid Shalchi, Maria Oliva Grassi, Joao N. Cardoso, Pearse A. Keane, Alfredo Niro, Maria Vittoria Cicinelli, Michele Reibaldi, et al. OCT Angiography in Acute Posterior Multifocal Placoid Pigment Epitheliopathy. Ophthalmic Surg Lasers Imaging Retina. 2019;50(7):428-436. doi:10.3928/23258160-20190703-04.
Souka AA, Hillenkamp J, Gora F, Gabel VP, Framme C.. Correlation between optical coherence tomography and autofluorescence in acute posterior multifocal placoid pigment epitheliopathy. Graefes Arch Clin Exp Ophthalmol. 2006;244(10):1219-1223. doi:10.1007/s00417-006-0343-1. PMID:16639621.
N P Jones. Acute posterior multifocal placoid pigment epitheliopathy. British Journal of Ophthalmology. 1995;79(4):384-389. doi:10.1136/bjo.79.4.384.
Copy the article text and paste it into your preferred AI assistant.
Article copied to clipboard
Open an AI assistant below and paste the copied text into the chat box.