Multiple evanescent white dot syndrome (MEWDS) is an acute inflammatory disease first reported by Jampol et al. in 19847). It predominantly affects one eye in young myopic women, presenting with numerous faint gray-white spots at the level of the deep retina to RPE, from the posterior pole to the equator. The white spots almost disappear within a few weeks, and visual acuity improves, making it a self-limiting disease.
In the Uveitis Clinical Practice Guidelines (Jpn J Ophthalmol 2019;123(6):635-696), it is classified as non-infectious posterior uveitis primarily involving the fundus, characterized by unilateral, acute onset, and transient course1).
MEWDS is considered part of the AZOOR complex (MEWDS, AZOOR, AMN, PIC, MFC, AIBSE, AAOR), a spectrum of inflammatory diseases primarily affecting the outer retina, photoreceptors, and RPE2). Among white dot syndromes, MEWDS is one of the diseases whose pathophysiology has been most elucidated by multimodal imaging2).
Sex ratio: Female predominance with a ratio of 4:11)
Annual incidence: approximately 0.22 cases per 100,000 population10)
Predominantly occurs in myopic eyes, often unilateral
About half of cases have flu-like prodromal symptoms 1–2 weeks before onset1)
Precipitating factors include flu-like symptoms, oral contraceptive use, vaccination, and upper respiratory tract infection1)
Bilateral involvement is extremely rare, with only 6–7 cases reported in the literature2, 4). When bilateral, the course is always asymmetric
Atypical age cases have also been reported; the youngest is a 9-year-old girl13) and the oldest is a 75-year-old man10)
QDoes MEWDS recur?
A
Most cases resolve after a single episode, but recurrence occurs in about 10% of cases. Strong immune stimulation such as vaccination or infection can trigger recurrence11). Even in recurrent cases, visual prognosis is relatively good. Within the continuum concept of AZOOR complex, there are reports of patients with a history of MEWDS later developing AZOOR or PIC.
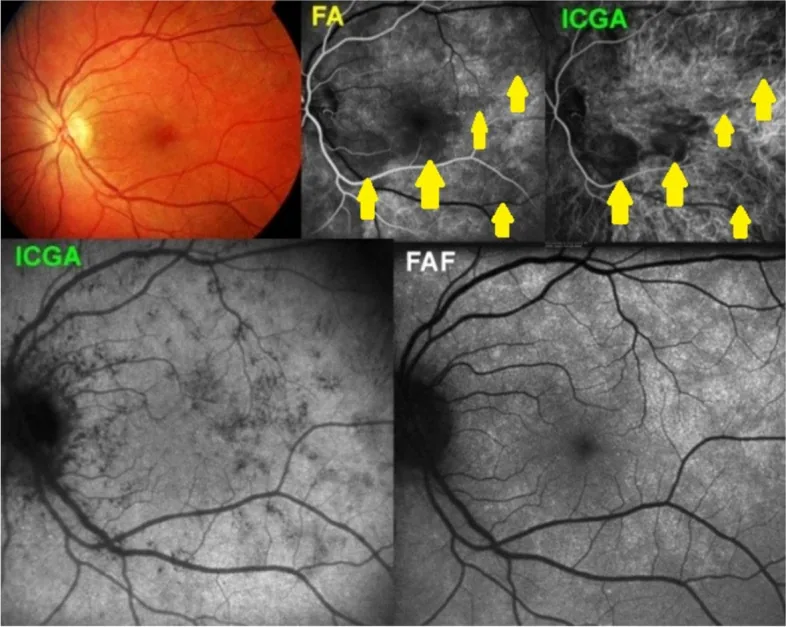
Papasavvas I, et al. Choroidal vasculitis as a biomarker of inflammation of the choroid. Indocyanine Green Angiography (ICGA) spearheading for diagnosis and follow-up, an imaging tutorial. J Ophthalmic Inflamm Infect. 2024. Figure 5. PMCID: PMC11618284. License: CC BY.
Fundus photographs show faint white dot lesions in the posterior pole. FA and ICGA reveal scattered punctate lesions, and FAF also shows abnormal signals, providing a visual understanding of the clinical findings of MEWDS.
Multiple pale patchy lesions scattered in the deep retina to RPE from the posterior pole to the equator 1). The white spots range from 100 to 200 μm in size, vary in size, and may coalesce. Mild optic dischyperemia and mild vitreous cells may be present 1). Foveal granularity (orange to yellow granular appearance) is a diagnostic finding confirmed by near-infrared FAF, seen in 74–96% of cases, and may be the only finding after white spots disappear 2)5).
Optic disc edema: may be accompanied by peripapillary serous subretinal fluid
Retinal venous sheathing and retinal hemorrhage: rare findings
Acute Phase Findings
Fundus white spots: Numerous pale gray-white spots scattered from the posterior pole to the equator. Smaller and more widespread than the white spots of APMPPE1).
Foveal granularity: Diagnostic finding confirmed by near-infrared FAF and slit-lamp biomicroscopy as foveal granularity. Appears in the active phase and disappears with recovery 2)5).
FAF (fundus autofluorescence): Shows hyperautofluorescence in the acute phase, with a mixture of hypofluorescence and hyperfluorescence 1)2).
OCT: Marked disruption and loss of the ellipsoid zone, and focal thickening of the RPE. Disruption of the IS/OS line in the active phase is useful for diagnosis 2)3).
Remission Phase Findings
Resolution of white spots: White spots disappear within a few weeks, and visual acuity improves 1).
Recovery of the ellipsoid zone: The ellipsoid zone often recovers over time on OCT2)3). Correlates with visual acuity recovery.
Preservation of choriocapillaris: On OCT-A, choriocapillaris blood flow is generally preserved (some flow voids reported) 4), indicating a pathophysiological difference from APMPPE.
QWhat is the "sparkling" (photopsia) felt in MEWDS?
A
Photopsia is thought to be caused by damage to the outer retina and the ellipsoid zone (the junction between the inner and outer segments of photoreceptors). When photoreceptors do not function properly, abnormal light stimulation signals are generated, causing the perception of light that is not present. It usually disappears as the disease recovers.
The primary site of MEWDS is the outer retina and the ellipsoid zone (IS/OS), while the choriocapillaris is generally preserved 2). Although late-phase hypofluorescence is observed on ICGA, it has been suggested that this may be caused by abnormal pigment uptake due to RPE dysfunction rather than ischemia of the choriocapillaris2). Choriocapillaris impairment (ICGA findings) is also observed around the optic disc where no white spots are seen, and may be more extensive than the clinically visible lesions 1).
As a disease within the AZOOR complex, it is thought to develop due to genetic predisposition (e.g., IL-10 haplotype) combined with environmental factors (viruses, vaccines, drugs) 2)7)
Vaccination: Onset after hepatitis B, influenza, HPV, meningococcal, and COVID-19 vaccines has been reported 15, 11). The median time from vaccination to MEWDS onset is reported as 14 days (range 1–90 days).
COVID-19 infection: Multiple cases of MEWDS after SARS-CoV-2 infection have been reported, and the number of MEWDS reports significantly increased during the COVID-19 pandemic 14). The average time from infection to onset is 29.6 days (range 0–70 days).
As an immunological mechanism, it has been suggested that vaccine-derived mRNA induces type I interferon (IFN-I) via RIG-I, potentially causing barrier dysfunction in RPE cells 15). Molecular mimicry and adjuvant-mediated inflammation are also hypothesized. A preliminary report indicates that the frequency of the HLA-B51 haplotype is 3.5 times higher in MEWDS patients than in the normal group 12).
White spots show late hypofluorescence. More extensive hypofluorescent areas than clinical findings. Peripapillary hypofluorescent spots also appear1)2)
A key feature of MEWDS is that FA shows hyperfluorescence from the early phase, which is an important distinction from APMPPE. APMPPE shows a reversal phenomenon (early hypofluorescence → late hyperfluorescence), whereas MEWDS shows persistent hyperfluorescence from the early phase 2)6). In OCT, the ellipsoid zone (IS/OS line) becomes irregular during the active phase, and improvement of this irregularity correlates with visual recovery, which is an important finding for understanding the pathophysiology 3).
MEWDS tends to be unilateral, transient, and fully recoverable, whereas PIC is often bilateral, leaves atrophic scars, and has a high rate (40–76%) of choroidal neovascularization (CNV). On FA, MEWDS shows hyperfluorescence from the early phase, while PIC shows leakage in the late phase. On OCT-A, the choriocapillaris is generally preserved in MEWDS, but PIC may show more severe changes1).
Since spontaneous recovery can be expected without specific treatment, observation is the basic approach for mild cases1). The white spots disappear spontaneously within a few weeks, and the visual prognosis is good. Over time, the ERG subsides and normalizes1).
Only consider the following when visual acuity loss is significant or when optic disc edema is present.
Oral prednisolone: Taper from 30 mg/day. Short-term use is indicated for cases with marked visual loss or optic disc edema.
Calnacrin tablets: Sometimes used in combination to improve microcirculation.
Since this disease has a strong tendency for spontaneous remission, treatment is unnecessary in most cases1).
Over time, the ERG normalizes and visual recovery is expected1).
In a review of 7 cases of COVID-19-associated MEWDS, 5 cases (71%) received some form of treatment, suggesting that COVID-19-associated cases may be slightly more severe than viral MEWDS in general14). Incomplete visual recovery has also been reported, so careful follow-up is required for COVID-19-associated cases.
When choroidal neovascularization is present, consider intravitreal anti-VEGF injections (bevacizumab, ranibizumab, aflibercept)1). Although CNV is rare, it can lead to poor visual prognosis, so caution is needed. OCT-A is useful for assessing CNV activity and helps in treatment decisions and efficacy evaluation of anti-VEGF therapy8).
QDoes steroid treatment lead to faster recovery?
A
Basically, this disease has a strong tendency for spontaneous remission, so treatment is unnecessary in most cases. The Uveitis Clinical Practice Guidelines also state that “spontaneous recovery without special treatment” is the basic policy1). Only in severe cases with significant visual loss or optic disc edema, oral steroids may be used to speed up recovery.
The main site of damage in MEWDS is the outer retina and ellipsoid zone (IS/OS junction), while the choriocapillaris is generally spared 2). This is an important pathophysiological difference from APMPPE.
OCT findings show that the ellipsoid zone (photoreceptor inner segment/outer segment junction) becomes irregular or absent during the active phase. It has been reported that visual acuity recovers as this disruption improves, indicating that the transient and reversible nature of outer retinal damage is the essence of MEWDS 3). Recent en face swept-source OCT has also visualized the extent of lesions that were difficult to recognize with conventional tomographic imaging 3).
Late-phase hypofluorescence on ICGA is observed, but it has been suggested that this may result from abnormal pigment uptake due to RPE dysfunction rather than ischemia of the choriocapillaris2). On OCT-A, blood flow in the choriocapillaris is generally preserved, with transient flow voids reported only in some cases 4)8). Studies using swept-source OCT-A have confirmed sparing of the choriocapillaris in MEWDS 4).
Foveal granularity observed on near-infrared FAF is a characteristic finding reflecting damage to the foveal photoreceptor layer 2)5). It can also be detected with multicolor imaging (near-infrared reflectance and blue reflectance) and is considered useful for diagnosis in the active phase.
The concept of the AZOOR complex has been proposed, integrating MEWDS, AZOOR, PIC, MFC, and others. It is thought that genetic predisposition (e.g., IL-10 haplotypes) combined with various environmental factors (viral infection, vaccines, drugs) leads to onset 2)7). Jampol and Becker (2003) proposed the hypothesis that these diseases share a common genetic autoimmune/inflammatory mechanism 7).
Choriocapillaris function assessment using OCT-A: Transient detection of flow voids in the choriocapillaris using swept-source OCT-A has been reported, and re-evaluation of the involvement of the choriocapillaris is ongoing 4)8). In some cases, decreased blood flow in the choriocapillaris is also observed, suggesting diversity in the pathology 8).
En face swept-source OCT: Reports are increasing as a new diagnostic method that three-dimensionally visualizes the shape, distribution, and inner layer boundaries of white dot lesions 3).
Progress in the AZOOR complex concept: Research is advancing to understand MEWDS, AZOOR, PIC, AMN, AIBSE, and AASR as a single spectrum 2)9). Zicarelli et al. (2020) proposed a new interpretation of the pathology of MEWDS 9).
Multicolor imaging: Development of clinical diagnostic support tools using near-infrared reflectance and blue reflectance. Non-invasive assessment of foveal granularity is now possible 5).
MEWDS after COVID-19 infection or vaccination: Cases of onset after infection or mRNA vaccination are increasingly reported worldwide, drawing attention to its role as an immune trigger.
Recurrence rate and long-term prognosis data: Accumulation of large-scale long-term follow-up studies is awaited.
Chen et al. (2024) reviewed 7 cases of MEWDS that developed after COVID-19 infection, reporting a mean age of 38.4 years, 5 females, and a mean interval from infection to onset of 29.6 days 14). Two cases (29%) were bilateral, and 5 (71%) received treatment, suggesting that COVID-19-associated cases may have a higher likelihood of incomplete visual recovery and need for treatment intervention than typical cases.
Regarding COVID-19 vaccine-associated MEWDS, a systematic review of 27 cases reported a median age of 34.1 years, female predominance, and a median interval from vaccination to onset of 14.7 days 14). The mRNA vaccine (Pfizer-BioNTech) was the most common.
Ramirez Marquez et al. (2022) reported a 17-year-old female who developed MEWDS after simultaneous HPV and meningococcal vaccination, and subsequently experienced two recurrences in the contralateral eye following COVID-19 infection and BNT162b2 vaccination 11).
Yasuda et al. (2022) reported a 67-year-old Japanese woman who developed MEWDS the day after the second dose of BNT162b2 mRNA vaccine 15). She had moderate vitritis, and visual acuity decreased to 0.2, but recovered to 0.8 without treatment.
Wiley et al. (2022) reported a case of a 17-year-old female who developed bilateral optic disc edema and MEWDS-like white dot lesions two days after SARS-CoV-2 vaccination, and cerebrospinal fluid examination revealed uveomeningeal syndrome with an opening pressure of 55 cmH2O and white blood cell count of 48 cells/μL 16). This was the first report of uveomeningeal syndrome associated with MEWDS.
Testi I, Modugno RL, Pavesio C. Multimodal imaging supporting the pathophysiology of white dot syndromes. Journal of ophthalmic inflammation and infection. 2021;11(1):32. doi:10.1186/s12348-021-00261-3. PMID:34529201; PMCID:PMC8446150.
Pichi F, Srvivastava SK, Chexal S, Lembo A, Lima LH, Neri P, et al. EN FACE OPTICAL COHERENCE TOMOGRAPHY AND OPTICAL COHERENCE TOMOGRAPHY ANGIOGRAPHY OF MULTIPLE EVANESCENT WHITE DOT SYNDROME: New Insights Into Pathogenesis. Retina. 2016;36(Supplement 1):S178-S188. doi:10.1097/IAE.0000000000001255. PMID:28005676.
Yannuzzi NA, Swaminathan SS, Zheng F, Miller A, Gregori G, Davis JL, Rosenfeld PJ.. Swept-Source OCT Angiography Shows Sparing of the Choriocapillaris in Multiple Evanescent White Dot Syndrome. Ophthalmic Surg Lasers Imaging Retina. 2017;48(1):69-74. doi:10.3928/23258160-20161219-10. PMID:28060397.
Mantovani A, Invernizzi A, Staurenghi G, Herbort CP Jr. Multiple Evanescent White Dot Syndrome: A Multimodal Imaging Study of Foveal Granularity. Ocular immunology and inflammation. 2019;27(1):141-147. doi:10.1080/09273948.2017.1353104. PMID:28981397.
R dell’Omo, R Wong, M Marino, K Konstantopoulou, C Pavesio. Relationship between different fluorescein and indocyanine green angiography features in multiple evanescent white dot syndrome. British Journal of Ophthalmology. 2009;94(1):59-63. doi:10.1136/bjo.2009.163550.
Jampol LM, Becker KG. White spot syndromes of the retina: a hypothesis based on the common genetic hypothesis of autoimmune/inflammatory disease. American journal of ophthalmology. 2003;135(3):376-9. doi:10.1016/s0002-9394(02)02088-3. PMID:12614757.
Khochtali S, Dridi T, Abroug N, Ksiaa I, Lupidi M, Khairallah M. Swept-Source Optical Coherence Tomography Angiography Shows Choriocapillaris Flow Reduction in Multiple Evanescent White Dot Syndrome. Journal of current ophthalmology. 2020;32(2):211-215. doi:10.4103/JOCO.JOCO_107_20. PMID:32671309; PMCID:PMC7337020.
Zicarelli F, Mantovani A, Preziosa C, Staurenghi G. Multiple evanescent white dot syndrome: a new interpretation. Ocul Immunol Inflamm. 2020;28(6):862-870.
Wang L, Lankry P, Rabinovitch D, Gallo R, Laiginhas R, Iyer P, Shulman S, Trivizki O.. An Elderly Man with Atypical Multiple Evanescent White Dot Syndrome. Case Rep Ophthalmol. 2022;13(3):892-896. doi:10.1159/000526583. PMID:36466057; PMCID:PMC9710463.
Ramirez Marquez E, Ayala Rodríguez SC, Rivera L, Pappaterra-Rodriguez MC, Requejo-Figueroa GA, Rios R, Rivera-Grana E, Rodríguez-García EJ, Oliver AL.. Contralateral Recurrences of Post-vaccination Multiple Evanescent White Dot Syndrome. Cureus. 2022;14(12):e32300. doi:10.7759/cureus.32300. PMID:36628035; PMCID:PMC9822784.
Smeller L, Toth-Molnar E, Sohar N.. White Dot Syndrome Report in a SARS-CoV-2 Patient. Case Rep Ophthalmol. 2022;13(3):744-750. doi:10.1159/000526090. PMID:36845457; PMCID:PMC9944209.
Shepherd EA, Herst BS, Parlitsis GJ, Shapiro MJ, Goldstein DA, Merrill PT.. Multiple Evanescent White-Dot Syndrome in a 9-Year-Old Girl. J Vitreoretin Dis. 2022;6(6):470-473. doi:10.1177/24741264211044222. PMID:37009534; PMCID:PMC9954785.
Chen N, Mandell M, Arjmand P. Multimodal imaging findings of multiple evanescent white dot syndrome in COVID-19 patients. IDCases. 2024;38:e02110. doi:10.1016/j.idcr.2024.e02110. PMID:39582747; PMCID:PMC11585666.
Yasuda E, Matsumiya W, Maeda Y, Kusuhara S, Nguyen QD, Nakamura M, Hara R.. Multiple evanescent white dot syndrome following BNT162b2 mRNA COVID-19 vaccination. Am J Ophthalmol Case Rep. 2022;26:101532. doi:10.1016/j.ajoc.2022.101532. PMID:35434421; PMCID:PMC8994682.
Wiley ZC, Pakravan M, Charoenkijkajorn C, et al. Uveomeningeal syndrome presenting with bilateral optic disc edema and multiple evanescent white dots syndrome (MEWDS). Am J Ophthalmol Case Rep. 2022;26:101538. doi:10.1016/j.ajoc.2022.101538. PMID:35514800; PMCID:PMC9062123.
Copy the article text and paste it into your preferred AI assistant.
Article copied to clipboard
Open an AI assistant below and paste the copied text into the chat box.