Sarcoidosis is a systemic inflammatory disease of unknown cause that forms non-caseating epithelioid cell granulomas in various organs. Histopathologically, it is characterized by granulomatous lesions composed of epithelioid cells and giant cells without necrosis. Common sites include the lungs, mediastinal lymph nodes, eyes, and skin, but it can also affect the heart, brain, bones, kidneys, gastrointestinal tract, and other organs.
In 1878, Sir Jonathan Hutchinson first reported it as a skin disease. In 1909, Danish ophthalmologist Heerfordt reported cases with uveitis, parotitis, and fever, which became known as Heerfordt syndrome9).
Sarcoidosis is the leading cause of uveitis. In a 2002 epidemiological survey, it accounted for 13.3% of all uveitis cases, and in a 2009 survey, 10.7% (both ranked first)1). Ocular involvement occurs in 20–50% of sarcoidosis patients2), and ocular symptoms are the initial manifestation in 30–40%. More than 85% of cases are bilateral2).
Age of onset shows a peak in the 20s for men, and a bimodal distribution in women with peaks in the 20s and 50s–60s. It is more common in women (male-to-female ratio 1:1.8)1), and the proportion of women increases after age 50.
Childhood sarcoidosis differs from adult sarcoidosis in its pathology3). Early-onset sarcoidosis (EOS) occurring at age 5 or younger corresponds to Blau syndrome with NOD2 gene mutations (R334W, R334Q), characterized by the triad of arthritis, dermatitis, and uveitis. The adult-type form occurring at ages 8–15 is thought to result from an excessive immune response to environmental antigens3).
QWhy is sarcoid uveitis common in Japan?
A
Sarcoidosis is the leading cause of uveitis in Japan, while its proportion is lower in Europe, the United States, and Southeast Asia. Genetic background (HLA-DRB1 alleles) and differences in environmental factors are suspected to be involved, but the exact reason remains unknown1).
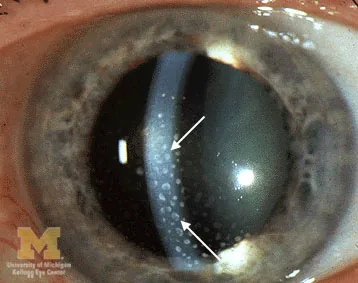
Trobe JT. Keratic precipitates. The Eyes Have It — Anterior Uveitis. University of Michigan Kellogg Eye Center. Via Wikimedia Commons (File:Keratic-precipitates.jpg). License: CC BY 3.0.
Large, yellowish-white, fatty granulomatous deposits are attached to the corneal endothelium, indicated by white arrows. These correspond to mutton-fat KPs discussed in section “2. Main symptoms and clinical findings.”
Ocular symptoms vary depending on the location and severity of inflammation. Blurred vision is the most common, followed by floaters (due to vitreous opacities), decreased vision, photophobia, redness, and eye pain. In chronic cases, the disease may progress asymptomatically, leading to delayed diagnosis 2). Ocular symptoms may precede systemic symptoms by several years.
:::caution Beware even when there are no subjective symptoms
In chronic cases, symptoms are often minimal. Active inflammation may only be detected through regular eye examinations.
:::
Lacrimal gland granulomas can cause lacrimal gland swelling leading to dry keratoconjunctivitis. Conjunctival nodules (often asymptomatic), scleritis (rare, non-necrotizing), and eyelid skin granulomas may also be observed. Cranial nerve palsies such as facial nerve palsy can occur.
The etiology is unknown. It is thought that an excessive immune response is triggered when genetically susceptible individuals are exposed to environmental antigens (inhaled antigens, infectious agents).
Involvement of Cutibacterium acnes (formerly Propionibacterium acnes) has been reported. Involvement of Mycobacterium tuberculosis DNA and various viruses has also been suggested2). As a genetic predisposition, association with HLA-DRB1 is known1), and the risk increases in familial cases2).
Risk Factor
Details
Race
More common in African Americans (about 10 times that of whites), also common in Northern Europeans
Sex
Slightly more common in women (male-to-female ratio 1:1.8)
Age
Men in their 20s; women in their 20s and 50s–60s
HLA
Association with HLA-DRB1 alleles1)
Family history
Increased risk if a first-degree relative has sarcoidosis2)
In early-onset sarcoidosis (EOS), NOD2 mutations (R334W, R334Q) cause excessive NF-κB signaling and emergence of pathogenic Th17 cells3).
:::tip Prevention and daily life
There is no established prevention method. For early detection, it is important to see an ophthalmologist if blurred vision or floaters persist.
:::
The principle of diagnosis is comprehensive assessment of clinical findings, laboratory findings, and histological findings.
:::caution Caution regarding systemic steroid administration before diagnosis
Systemic steroids can shrink lesions and cause false-negative biopsy results. Unless urgent, avoid systemic steroids until diagnosis is confirmed.
:::
QCan sarcoidosis be ruled out if blood ACE is normal?
A
No. Sensitivity is 73%, so about one-fourth show normal values. False negatives occur during steroid therapy or ACE inhibitor use. Comprehensive evaluation of clinical findings, imaging, and other tests is necessary 2).
QHow to differentiate sarcoidosis from malignant lymphoma?
A
Both can present with choroidal lesions and lymphadenopathy. Differential diagnosis proceeds using the IL-10/IL-6 ratio in aqueous humor or vitreous fluid (>1 suggests lymphoma) and FDG-PET accumulation patterns. Tissue biopsy is required for definitive diagnosis 5).
Indications for systemic administration 1): severe anterior uveitis resistant to local treatment, severe vitreous opacity, extensive retinochoroiditis, retinal vasculitis, macular edema, optic disc edema, granuloma
Prednisolone 0.5–1.0 mg/kg/day for 2–4 weeks, then taper by 5–10 mg/day every 4–8 weeks 1). Total treatment duration may be 6 months to over 1 year 1).
Example tapering schedule:
Dose
Duration
30 mg/day
2 weeks
20 mg/day
1 month
15 mg/day
1 month
10 mg/day
1 month
7.5 mg/day
1 month
5 mg/day
1 month
5 mg/day (every other day)
1 month
:::caution Precautions for long-term steroid use
Monitor for osteoporosis, diabetes, hypertension, and infection risk. In long-term use, consider concomitant use of gastric mucosal protectants and bisphosphonates.
:::
Adalimumab (Humira®): 40 mg every 2 weeks subcutaneously 2, 4). Anti-TNF-α antibody approved for non-infectious uveitis. The VISUAL I and VISUAL II trials confirmed its efficacy in suppressing recurrence 4).
Infliximab (Remicade®): 5 mg/kg intravenous infusion every 8 weeks 1). Approved for Behçet’s disease refractory retinal uveitis; off-label for sarcoidosis.
Etanercept has low efficacy 1). Screening for tuberculosis and hepatitis B is mandatory before initiating biologic therapy 4).
Cataract surgery: Performed during the quiescent phase. If complete quiescence is difficult, surgery is performed with oral steroids when inflammation is relatively controlled. If future filtering surgery may be needed, preserve the superior conjunctiva and choose a corneal incision.
Secondary glaucoma: Managed stepwise with topical hypotensive agents (PG analogs, beta-blockers, carbonic anhydrase inhibitors, alpha-2 agonists) → oral CAI → intravenous D-mannitol. Trabeculotomy is particularly effective for steroid-induced glaucoma. If insufficient, perform trabeculectomy.
Retinal photocoagulation: Performed for avascular areas due to occlusive vasculitis. Direct coagulation for retinal microaneurysms.
Mild anterior segment inflammation may be treated with eye drops alone. However, if posterior segment lesions (cystoid macular edema, extensive retinochoroiditis, optic neuropathy) are present, posterior sub-Tenon injection or systemic administration is required.
QCan sarcoid uveitis be completely cured?
A
Approximately two-thirds of cases follow a benign, self-limited course, and many have good visual prognosis without systemic steroids. Some cases become chronic and require long-term treatment. Inflammation centered on the anterior segment has a good prognosis, but repeated posterior segment involvement can lead to retinal degeneration and optic atrophy, resulting in severe visual impairment.
Histological features of granulomas: aggregates of non-caseating epithelioid cells and lymphocytes. Asteroid bodies and Schaumann bodies within multinucleated giant cells. Surrounding ring-shaped fibrosis 2).
Major intraocular pathologies: granuloma deposition in the trabecular meshwork → impaired aqueous outflow → secondary glaucoma6). Granulomatous infiltration of retinal vessel walls → periphlebitis → candle wax dripping exudates. Increased VEGF production in the inflammatory environment → choroidal neovascularization10).
Excess vitamin D production (increased 1,25(OH)₂D₃ synthesis by macrophages) can lead to hypercalciuria and hypercalcemia 2).
In early-onset pediatric cases (NOD2 mutation), excessive NF-κB signaling and emergence of pathogenic Th17 cells promote granuloma formation 3).
:::danger Information on research stage
The treatments and research results described in this section include some that are still in the research stage. In actual clinical practice, decisions should be made in consultation with a specialist.
:::
Application of faricimab to refractory cystoid macular edema12): A dual inhibitor of VEGF and Ang-2. In a 2025 report by Lin, an 82-year-old woman with steroid-resistant CME showed improvement in BCVA in both eyes after two injections (right 20/200→20/50, left 20/400→20/63), and foveal retinal thickness also markedly improved (right 562→371 μm, left 717→286 μm). This is the world’s first report of its application to ocular sarcoidosis12).
Association with immune checkpoint inhibitors11): In Read 2025, a patient with a history of severe ocular sarcoidosis received pembrolizumab for over 2 years without ocular recurrence. This case report suggests the possibility of safe use under careful monitoring.
Association between sarcoidosis and malignant tumors (sarcoid-lymphoma syndrome)5): Disruption of immune regulation may predispose to lymphoma development, and attention should be paid to tumor development during long-term follow-up.
Advances in multimodal imaging2): EDI-OCT depicts choroidal granulomas as homogeneous, hyporeflective, well-defined lesions. OCTA (optical coherence tomography angiography) enables detection of choriocapillaris flow deficits. ICGA (indocyanine green angiography) is useful for detecting occult choroidal granulomas and assessing treatment response.
Long-term prognosis of childhood sarcoidosis3): In 52 cases of childhood-onset adult-type sarcoidosis (median follow-up 11.5 years), 50% maintained active disease into adulthood. Among patients who achieved remission in childhood, 19% relapsed in adulthood. Lifelong follow-up is recommended.
Berkowitz ST, Brock AL, Reichstein DA. Chorioretinal biopsy-proven ocular sarcoidosis in a patient with a history of B-cell lymphoma. Case Rep Ophthalmol. 2021;12(2):438-445. doi:10.1159/000512694. PMID:34054498; PMCID:PMC8136327.
Sarcoidosis and inflammatory glaucoma. Oman J Ophthalmol. 2011;4(1):5.
Oyeniran E, Katz D, Kodati S.. Isolated Optic Disc Granuloma as a Presenting Sign of Sarcoidosis. Ocul Immunol Inflamm. 2024;32(2):175-177. doi:10.1080/09273948.2022.2127783. PMID:36223603; PMCID:PMC10090223.
Riccardi M, Contento R, Christensen C, Brady A, Swan RL, Swan RT. A Case of Sarcoid Uveitis Diagnosed With Mammography Two Months After Normal Chest Imaging. Case reports in ophthalmological medicine. 2025;2025:8871004. doi:10.1155/crop/8871004. PMID:39975857; PMCID:PMC11839256.
Nakamura M, Suzuki K, Yoshida E, Watanabe K, Sasage H, Dohi K, Suzuki S.. A Case of Incomplete Heerfordt Syndrome Diagnosed Following Fever Onset. Cureus. 2025;17(10):e94234. doi:10.7759/cureus.94234. PMID:41210040; PMCID:PMC12596090.
Zong Y, Wang K, Zhang T, Xu G.. Pediatric peripapillary choroidal neovascularization secondary to ocular sarcoidosis: a long-term follow-up case. BMC Ophthalmol. 2025;25(1):422. doi:10.1186/s12886-025-04266-7. PMID:40702433; PMCID:PMC12285086.
Read C, Bhatia S, Totonchy M.. Programmed cell death 1 blockade in the setting of severe ocular sarcoidosis: Cancer immunotherapy in a patient with autoimmunity. JAAD Case Rep. 2025;62:43-45. doi:10.1016/j.jdcr.2025.04.017. PMID:40661112; PMCID:PMC12256288.
Lin TH, Lin HY, Chuang YH, Tseng PC.. Faricimab as Treatment for Sarcoid Uveitis With Refractory Cystoid Macular Edema. J Vitreoretin Dis. 2025:24741264251358628. doi:10.1177/24741264251358628. PMID:40765984; PMCID:PMC12318965.
Copy the article text and paste it into your preferred AI assistant.
Article copied to clipboard
Open an AI assistant below and paste the copied text into the chat box.