Floaters are symptoms caused by opacities in the vitreous (the transparent gel-like tissue filling the eyeball) projecting onto the retina. Against bright backgrounds such as white walls, bright skies, or windows, objects like mosquitoes, soot, or rings appear to drift with eye movements.
Floaters are one of the most common complaints in ophthalmology outpatient clinics 3). The underlying causes range from age-related physiological changes to urgent conditions such as retinal tears and retinal detachment. Therefore, it is important to carefully assess the nature of symptoms, onset, and accompanying symptoms to avoid missing pathological floaters.
Blue field entoptic phenomenon is a phenomenon in which small white dots appear to move randomly in the visual field when looking at a bright blue light such as a blue sky, and is distinguished from floaters. This is the perception of the movement of white blood cells within the retina and is not pathological.
Posterior vitreous detachment (PVD) is an age-related change that occurs frequently in people over 50 and is the most common cause of floaters. Reports indicate that about 14% of patients with acute symptoms of PVD are found to have retinal tears 1), and it is not uncommon for it to be asymptomatic. The combination of unilateral acute floaters and photopsia requires fundus examination3).
2. Types of Floaters (Physiological vs Pathological)
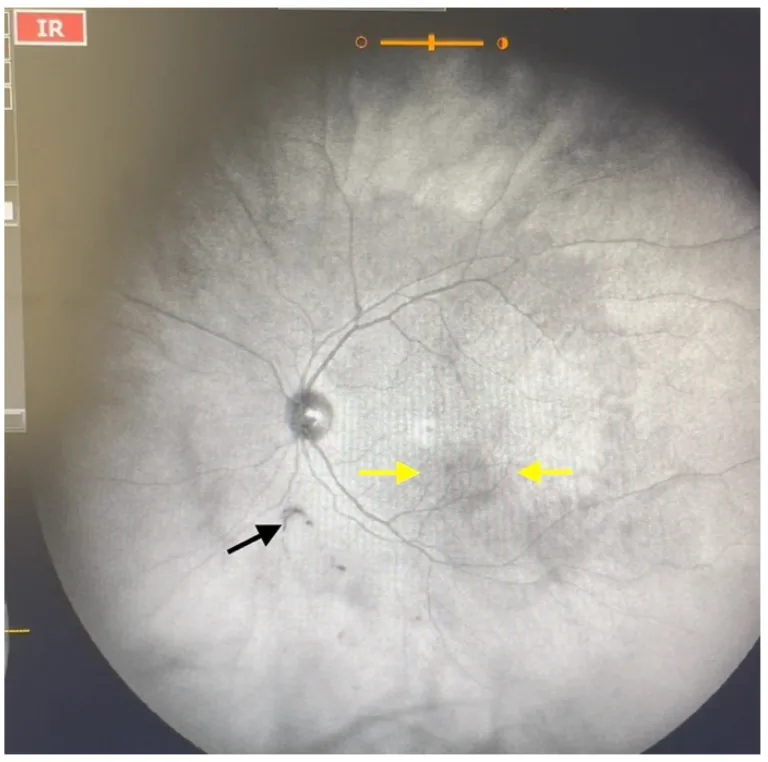
Garcia-Aguirre G, Henaine-Berra A, Salcedo-Villanueva G. Visualization and Grading of Vitreous Floaters Using Dynamic Ultra-Widefield Infrared Confocal Scanning Laser Ophthalmoscopy: A Pilot Study. J Clin Med. 2022;11(18):5502. Figure 3. PMCID: PMC9571201. License: CC BY 4.0.
Scattered shadows in the macula (yellow arrows) and a Weiss ring outside the macula (black arrow) are depicted on ultra-widefield IRcSLO. This corresponds to Weiss ring formation associated with posterior vitreous detachment, discussed in the section “2. Types of Floaters (Physiological vs Pathological)”.
Characteristics: Not a target for treatment. They are most noticeable immediately after PVD, but as vitreous liquefaction progresses, the prepapillary glial ring (Weiss ring) moves away from the retina, and symptoms gradually diminish.
Movement with gaze changes: Floaters move in conjunction with eye movements.
Note that vitreous opacities in asteroid hyalosis (calcium crystal deposits in the vitreous) are an exceptional disease that is often not perceived as floaters.
QCan floaters be cured?
A
Physiological floaters do not require treatment and often become less noticeable as vitreous liquefaction progresses. Pathological floaters may improve with treatment of the underlying cause. Typical treatments include laser photocoagulation for retinal tears, surgery for retinal detachment, and treatment of the cause of vitreous hemorrhage. Active treatment for physiological floaters (YAG laser vitreolysis, vitrectomy) is considered only in limited cases when quality of life is significantly impaired.
Maltsev DS, Kulikov AN, Burnasheva MA, et al. Involvement of Sclera in Lattice Retinal Degeneration: An Optical Coherence Tomography Study. Diagnostics (Basel). 2024;14(13):1295. Figure 5. PMCID: PMC11202986. License: CC BY 4.0.
A horseshoe retinal tear surrounded by laser photocoagulation scars is shown from multiple angles in OCT cross-sectional images (A and B) and a fundus color photograph (C). This corresponds to the retinal tear discussed in the section “3. Causes of floaters (differential diagnosis).”
Visual field defect, tobacco dust, photopsia combined, sudden increase in floaters with vision loss
Visit an ophthalmologist on the same day. A facility capable of emergency care is preferable.
Early visit (within a few days)
Sudden onset of floaters, clear increase in number of floaters, change in shape
Visit an ophthalmologist within 1 to 3 days.
Regular follow-up
Pre-existing floaters unchanged, only swaying against bright background
Continue regular eye examinations
Within 6 weeks after onset of PVD, the risk of retinal tear is highest 2), and if symptoms change during this period, prompt medical attention is required.
QI have had floaters before, but they have recently increased. Should I see a doctor?
A
A sudden increase in floaters or change in their characteristics (increase in number, change in shape, appearance of new black spots like tobacco dust) may indicate pathological floaters. Especially if photopsia occurs simultaneously, early ophthalmologic examination is necessary as a warning sign of retinal tear. If pre-existing floaters continue unchanged, they are likely physiological, but regular fundus examinations are recommended.
After visiting an ophthalmologist, the first step is to determine whether the floaters are physiological or pathological. A vitreous examination using a slit-lamp microscope and a non-contact biconvex lens is performed to check for the presence of a prepapillary glial ring (Weiss ring) as an indicator of PVD and to assess vitreous opacities.
In vitreous examination, it is important to narrow the slit beam width and maximize illumination intensity to dynamically observe the vitreous movement. If only PVD is present without obvious vitreous opacities other than the prepapillary glial ring, physiological floaters can be diagnosed. However, if tobacco dust, hemorrhage, or flare is observed, a detailed fundus examination is necessary.
After instilling mydriatic drops, the peripheral fundus is examined extensively to check for retinal tears, retinal detachment, and vitreous hemorrhage.
If hemorrhage does not resolve, consider vitrectomy
Uveitis
Inflammation control (steroids, etc.)
Workup and treatment of underlying disease required
QHow long does it take for the pupils to return to normal after a dilated eye exam?
A
When dilating drops (e.g., tropicamide) are used, the pupils usually return to normal within 4 to 6 hours. During this time, light appears bright and near vision is blurry, so driving a car or bicycle should be avoided. It is recommended to bring sunglasses. The effect of dilating drops varies among individuals, and recovery may take 6 to 8 hours.
The vitreous is a transparent gel-like tissue that fills the eye, composed mainly of collagen fibers and hyaluronic acid. With aging, collagen fibers aggregate and degenerate, leading to vitreous liquefaction (syneresis). The liquefied areas form lacunae, and the surrounding residual gel becomes opaque, scattering light. This opacity projects onto the retina and is perceived as floaters.
As vitreous liquefaction progresses, the adhesion between the vitreous and retina weakens, and eventually the posterior vitreous membrane separates from the retina (posterior vitreous detachment: PVD). Immediately after PVD occurs, the prepapillary glial ring (Weiss ring) is located just above the retina, causing strong perception of floaters. As vitreous liquefaction further progresses to complete PVD, the Weiss ring moves away from the retina, and symptoms tend to diminish.
During PVD, in areas where the vitreous and retina are locally strongly adherent (e.g., lattice degeneration), traction forces concentrate when the vitreous separates, potentially tearing the retina (retinal tear)2). This traction stimulates the retina and is perceived as photopsia. If fluid enters the subretinal space through the tear, it can progress to rhegmatogenous retinal detachment4).
In high myopia, the eyeball volume increases due to axial elongation, so vitreous liquefaction progresses from a young age 6). In addition, lattice degeneration and retinal tears in the peripheral retina are more frequent, and the onset of floaters tends to occur at a relatively younger age.
Even when floaters do not cause vision loss, they can have a significant impact on patients’ mental burden and quality of life. In a study by Wagle et al. (2011), the utility value associated with floaters averaged 0.98, but patients with more severe symptoms showed significantly lower QOL scores 9). It is important not to treat floaters as a minor symptom and to listen carefully to patients’ complaints.
In an RCT by Shah et al. (2017), YAG laser vitreolysis for symptomatic vitreous opacities resulted in significant symptom improvement compared to sham control (53.3% vs 8.7%, p=0.02) 7). However, the procedure is highly dependent on the operator’s skill, and there are risks of complications (increased intraocular pressure, lens damage, retinal damage), so careful selection of facilities and indications is important.
A treatment method involving intravitreal injection of an enzyme (ocriplasmin) to chemically release vitreous traction is being studied. In an RCT by Stalmans et al. (2012), the efficacy of ocriplasmin for vitreomacular traction and macular hole was demonstrated 10). Its application to floaters themselves is still at the research stage.
Byer et al. (1994) showed in a natural history study after PVD onset that the risk of retinal tears is highest immediately after the onset of posterior vitreous detachment2). Subsequent studies have indicated that follow-up observation within 6 weeks after the onset of acute symptomatic PVD is a key strategy to prevent tears and detachment, and standardization of follow-up timing is being promoted 3).
Hollands H, Johnson D, Brox AC, et al. Acute-onset floaters and flashes: is this patient at risk for retinal detachment? JAMA. 2009;302(20):2243-2249.
Byer NE. Natural history of posterior vitreous detachment with early management as the premier line of defense against retinal detachment. Ophthalmology. 1994;101(9):1503-1514. doi:10.1016/s0161-6420(94)31141-9.
Kahawita S, Simon S, Engelbrecht T. Acute symptomatic posterior vitreous detachment and the prevalence of associated retinal tears: a systematic review. Eye (Lond). 2024;38(5):825-833.
Feltgen N, Walter P. Rhegmatogenous retinal detachment—an ophthalmologic emergency. Deutsches Arzteblatt international. 2014;111(1-2):12-21; quiz 22. doi:10.3238/arztebl.2014.0012. PMID:24565273; PMCID:PMC3948016.
Ohno-Matsui K, Lai TY, Lai CC, Cheung CMG. Updates of pathologic myopia. Prog Retin Eye Res. 2016;52:156-187. PMID:26769165. doi:10.1016/j.preteyeres.2015.12.001.
Shah CP, Heier JS. YAG Laser Vitreolysis vs Sham YAG Vitreolysis for Symptomatic Vitreous Floaters: A Randomized Clinical Trial. JAMA ophthalmology. 2017;135(9):918-923. doi:10.1001/jamaophthalmol.2017.2388. PMID:28727887; PMCID:PMC5710539.
de Nie KF, Crama N, Tilanus MA, Klevering BJ, Boon CJ. Pars plana vitrectomy for disturbing primary vitreous floaters: clinical outcome and patient satisfaction. Graefe’s archive for clinical and experimental ophthalmology = Albrecht von Graefes Archiv fur klinische und experimentelle Ophthalmologie. 2013;251(5):1373-82. doi:10.1007/s00417-012-2205-3. PMID:23250478.
Wagle AM, Lim WY, Yap TP, Neelam K, Au Eong KG. Utility values associated with vitreous floaters. American journal of ophthalmology. 2011;152(1):60-65.e1. doi:10.1016/j.ajo.2011.01.026. PMID:21570045.
Stalmans P, Benz MS, Gandorfer A, et al. Enzymatic vitreolysis with ocriplasmin for vitreomacular traction and macular holes. N Engl J Med. 2012;367(7):606-615. PMID:22894573. doi:10.1056/NEJMoa1110823.
Copy the article text and paste it into your preferred AI assistant.
Article copied to clipboard
Open an AI assistant below and paste the copied text into the chat box.