Pars plana vitrectomy (PPV) is a surgery performed inside the eye for lesions in the retina and vitreous. It is also called vitrectomy. Generally, a vitreous cutter is inserted through the pars plana to remove the vitreous, and depending on the disease, membrane peeling, photocoagulation, gas tamponade, etc., are performed to treat retinal diseases.
Modern vitrectomy began in the 1970s with Machemer’s pars plana vitrectomy using an electric vitreous cutter. In Japan, Machemer’s disciples, Tano and Hida, actively promoted the spread of vitrectomy.
The origin dates back to 1969 when Kasner reported “open-sky vitrectomy.” In 1974, O’Malley established a 20-gauge (G) transconjunctival approach. Subsequently, instruments became smaller with 25G, 23G, and 27G, and minimally invasive vitrectomy surgery (MIVS) is now the mainstream 6).
The purposes of surgery are broadly divided into the following eight categories.
Removal of vitreous opacities: When opacities due to inflammation or hemorrhage impair visual function or hinder diagnosis and treatment.
Removal of vitreous traction: For VMT, retinal detachment, proliferative diabetic retinopathy, ROP, etc.
Removal of cytokines: When VEGF and inflammatory cytokines are present at high concentrations in proliferative diabetic retinopathy, neovascular glaucoma, RVO, and uveitis.
Removal of subretinal lesions: For age-related macular degeneration hemorrhage, ruptured microaneurysm hemorrhage, PVR subretinal bands, etc.
Control of intraocular pressure: For malignant glaucoma and elevated vitreous pressure in acute glaucoma attacks.
Removal of intraocular foreign bodies: Traumatic foreign bodies, dropped IOL.
Irrigation of infected focus: Removal of bacteria and endotoxins in endophthalmitis
Biopsy: Vitreous biopsy, cytology, and cytokine measurement for suspected malignant lymphoma
QWhat type of anesthesia is used for pars plana vitrectomy?
A
Currently, most vitrectomies can be performed under monitored anesthesia care (MAC) with local anesthesia (sub-Tenon’s or retrobulbar block).4, 7) 2% lidocaine 3–4 mL provides pain relief and akinesia. General anesthesia is selected for children, patients with psychiatric disorders, prolonged surgery, scleral buckling, or open globe injuries. In open globe injuries, general anesthesia is often chosen due to the risk of intraocular infiltration of local anesthetics.
The following subjective symptoms are common to diseases indicated for pars plana vitrectomy.
Decreased visual acuity: Occurs with progression of vitreous hemorrhage, macular lesions, or retinal detachment. In full-thickness macular holes, central vision is markedly reduced. 4)
Metamorphopsia (distortion): Caused by macular traction from epiretinal membrane or vitreomacular traction. Can be confirmed with an Amsler grid.
Visual field defect and photopsia: In retinal detachment, a visual field defect occurs corresponding to the affected area. Photopsia at the time of tear formation may be a prodromal symptom.
The following findings are confirmed by slit-lamp microscopy, fundus examination, and OCT.
Macular Diseases
Full-thickness macular hole (FTMH): OCT shows retinal elevation at the hole edge and vitreous traction. Evaluated by Gass classification stages 1–4. In stages 2–4, visual acuity may decrease to 20/200–20/400. 4)
Epiretinal membrane: A grayish-white semitransparent membrane is seen on the fundus. OCT reveals a hyperreflective linear structure on the retinal surface and inner layer traction.
Vitreomacular traction (VMT): OCT shows adhesion and traction between the posterior vitreous cortex and the fovea.
Retinal and Vitreous Diseases
Rhegmatogenous retinal detachment: A wavy, semitransparent detached retina is seen on fundus examination. The location of tears and lattice degeneration is confirmed.
Proliferative diabetic retinopathy: Hemorrhage and proliferative membrane formation from retinal neovascularization due to long-term poor glycemic control.
Full-thickness macular hole: Idiopathic tangential traction of the posterior vitreous cortex is the main cause. The incidence of full-thickness macular hole in the fellow eye is reported to be 10–15%. 4)
In eyes that have undergone pars plana vitrectomy with gas tamponade, the decrease in atmospheric pressure during air travel can cause gas expansion, leading to a rapid increase in intraocular pressure.
Foulsham et al. (2021) calculated and reported based on Boyle’s law that when a gas-filled eye with 50% C₃F₈ (perfluoropropane) is aboard an aircraft, intraocular pressure increases by 10.8 mmHg per 1000 feet of altitude, reaching a maximum of 42 mmHg. 1)
This intraocular pressure elevation can cause ischemia of the optic nerve and retinal vessels. Air travel is contraindicated until the gas has completely resolved. 1)
QWhy is a face-down position necessary after surgery?
A
After gas tamponade for macular hole, a face-down position is required because the gas floats and presses the macula from above, promoting hole closure. The duration of positioning varies depending on the surgical technique, type of gas, and hole size; follow your doctor’s instructions.
FA/OCTA: Evaluation of neovascularization in proliferative diabetic retinopathy, identification of retinal ischemic areas, assessment of vascular lesions and non-perfusion areas, and confirmation of postoperative complications.
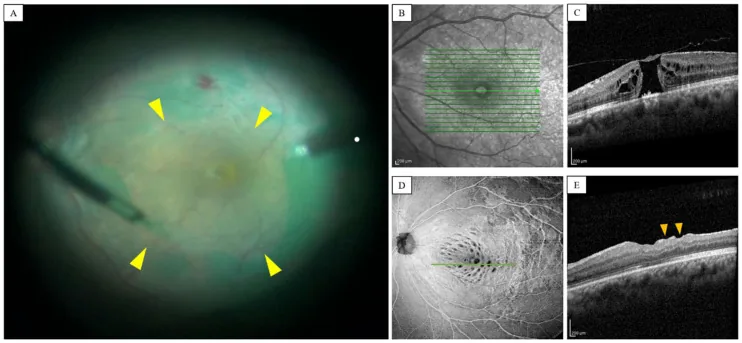
He S, Ye X, Qiu W, et al. Analysis of Retinal Microstructure in Eyes with Dissociated Optic Nerve Fiber Layer (DONFL) Appearance following Idiopathic Macular Hole Surgery. J Pers Med. 2023;13(2):255. Figure 1. PMCID: PMC9963747. License: CC BY 4.0.
Intraoperative fundus image (A) shows the internal limiting membrane (ILM) after ICG staining being grasped and peeled with forceps, with the yellow arrowhead indicating the peeling edge; preoperative OCT (C) shows marginal elevation of a full-thickness macular hole, and postoperative OCT (E) shows a small depression (dimple) in the inner retinal layer that occurred after ILM peeling. This corresponds to the internal limiting membrane peeling discussed in the section “5. Standard Treatment.”
In microincision vitrectomy surgery (MIVS), instruments are inserted via cannulas without conjunctival incision. Currently, almost all cases are performed with MIVS, and in many cases, surgery can be completed without sutures. 6) MIVS differs significantly from conventional 20G surgery in that instruments such as endoilluminators and vitreous cutters can be inserted through cannulas placed into the vitreous cavity from above the conjunctiva without incising the conjunctiva.
Gauge
Incision Size
Features
20G
Approx. 0.9 mm
Former standard. Requires scleral suture. Currently almost unused.
23G
Approx. 0.6 mm
MIVS popular type. Often sutureless.
25G
Approx. 0.5 mm
Introduced in 2002. Current mainstream. Minimally invasive.
27G
Approximately 0.4 mm
Smallest diameter. Becoming popular in recent years.
Trocar cannula insertion (3 ports): Inserted 3.5–4 mm from the limbus (4 mm for phakic eyes, 3.5 mm for aphakic/pseudophakic eyes). Inserting at a 30-degree angle from the sclera facilitates self-sealing of the scleral wound.
Vitrectomy: Create a posterior vitreous detachment (PVD) and resect up to the vitreous base. Using triamcinolone acetonide improves visualization of the vitreous.
Membrane peeling: Stain and peel the internal limiting membrane with indocyanine green (ICG) or brilliant blue G (BBG).
Hemostasis: Increase infusion pressure to 40 mmHg or higher, aspirate, and diathermy coagulate bleeding points.
Retinal reattachment (in cases of retinal detachment): Reattach the detached retina using fluid-air exchange.
Photocoagulation: Apply 2–3 rows around retinal tears (less than 200 mW, up to about 1,000 shots).
Tamponade: Choose from SF₆ gas (diluted to 20% or less), C₃F₈ gas (diluted to 12% or less), or silicone oil (for giant retinal tears or PVR).
Cannula removal and wound closure confirmation: Confirm self-sealing; suture with 8-0 absorbable suture if necessary.
Wide-angle observation systems (non-contact lenses) and contact lenses are used depending on the application. Wide-angle observation is advantageous for treating the peripheral retina, but there may be optical blind spots. 3)
After photocoagulation or cryocoagulation of the tear, tamponade is performed to reattach the retina. In surgery for epiretinal membrane, simultaneous removal of the ILM (internal limiting membrane) reduces the recurrence rate of epiretinal membrane. Approximately 80% of epiretinal membranes contain residual glial elements, and ILM removal helps eliminate these. 5)
Gas expands when diluted inside the eye. At high altitudes, it expands according to Boyle’s law, causing increased intraocular pressure; therefore, air travel is contraindicated before the gas is absorbed. 1)
QWhy is silicone oil removed later?
A
Silicone oil left in place for a long time can cause complications such as cataract, secondary glaucoma, and corneal opacity. Therefore, removal surgery is generally performed after the retina has reattached and stabilized. In cases with a high risk of refractory retinal detachment or phthisis bulbi, the oil may be left in place.
QWhat should be noted during subsequent surgery if gas is present in the eye?
A
If nitrous oxide (laughing gas) is used while intraocular gas (SF₆, C₃F₈, etc.) remains, the gas bubble expands, causing a rapid rise in intraocular pressure, which can lead to blindness in the worst case. 4) When undergoing surgery in another department, it is essential to inform the attending ophthalmologist and anesthesiologist of the residual intraocular gas and to avoid the use of nitrous oxide. Wearing a warning wristband is recommended. 4, 8)
Most vitrectomy procedures can be performed under monitored anesthesia care (MAC) plus local anesthesia. 4, 7) Typically, retrobulbar or sub-Tenon anesthesia is chosen, using 3–4 mL of 2% lidocaine to achieve pain relief and akinesia.
Sub-Tenon Anesthesia
Technique: An incision is made in the inferonasal conjunctiva, and anesthetic is injected into the sub-Tenon space using a 27G blunt needle.
Dosage: 3–4 mL for vitrectomy.
Features: Provides equivalent analgesia to retrobulbar anesthesia, with fewer serious complications such as globe perforation, and is easier to perform. 8)
Agents: A 1:1 mixture of 2% lidocaine and 0.5% bupivacaine (Marcaine) or 0.75% ropivacaine (Naropin). Ropivacaine has low toxicity, is preservative-free, and has a lower risk of allergy. 8)
Retrobulbar Anesthesia
Technique: 4–6 mL of anesthetic is injected into the intraconal space, anesthetizing the oculomotor, trochlear, abducens, optic, trigeminal, and ciliary ganglia.
Features: Provides superior akinesia compared to sub-Tenon anesthesia.
Complications: Retrobulbar hemorrhage (0.1–3%), globe perforation (0.9/10,000), optic nerve injury. Risk is increased in high myopia, long axial length, and previous scleral buckle. 7)
Peribulbar Anesthesia
Technique: 5–10 mL is administered outside the muscle cone. Slower onset than retrobulbar block but similar effect.
Efficacy: No significant difference in pain scores or akinesia compared to retrobulbar anesthesia. 7)
Complications: Perforation rate 1/16,000 (lower than retrobulbar). Conjunctival edema is more common with peribulbar, while eyelid hematoma is more common with retrobulbar. 7)
Other local anesthesia techniques:
Topical anesthesia: 4% lidocaine eye drops, onset about 16 seconds, duration about 14 minutes. It only suppresses pain sensation in the cornea, conjunctiva, and sclera, with no effect on the iris, ciliary body, or eye movement.
Intracameral anesthesia: 0.5 mL of 1% preservative-free lidocaine injected into the anterior chamber. Duration of action is about 10 minutes. Combined with topical anesthesia, it improves pain control. 7)
Subconjunctival anesthesia: Infiltration anesthesia acting on the conjunctiva and sclera. It may be effective for simple small-incision surgery.
Needle block complications: 7)
Posterior staphyloma, history of scleral buckle surgery, and long axial length (>26 mm) increase the risk of perforation. Other serious complications include strabismus, intravascular injection, subarachnoid injection, and macular infarction. Local anesthetic toxicity progresses from initial excitatory symptoms and hypertension to generalized convulsions in the advanced stage, and finally to hypotension and cardiac arrest in the terminal stage. Early recognition and management are important.
Indications for general anesthesia: General anesthesia is selected for infants, children, patients with mental illness, dementia, involuntary movements, claustrophobia, long surgeries, scleral buckle surgery, and cases of globe rupture. Combining general anesthesia with a local anesthetic block can prevent the oculocardiac reflex (OCR) and stabilize hemodynamics.
Sedation (MAC): Options include propofol, opioids, and benzodiazepines. Intravenous sedation has been shown in meta-analyses to significantly reduce pain. 7) For patients with high anxiety, consider preoperative intramuscular injection of hydroxyzine plus pentazocine. Excessive sedation can cause disinhibition and be counterproductive (the principle of “Local is Vocal”).
Intraoperative visual experience: Perception of light, color, and movement is accompanied by discomfort in 3–18% of cases. Preoperative explanation is recommended to reduce patient anxiety. 7)
There are no significant differences in visual acuity, visual function, complications, or patient satisfaction among anesthesia methods; the choice is based on the surgeon’s experience and patient conditions. 7)
QWhich is more suitable: sub-Tenon's anesthesia or retrobulbar anesthesia?
A
There are no significant differences in analgesic effect, visual acuity, complications, or patient satisfaction between anesthesia methods, and no absolute superiority. 7) Generally, sub-Tenon’s anesthesia is easier to perform and has a lower risk of perforation. Retrobulbar anesthesia provides better control of eye movement and may be advantageous for complex, long-duration surgeries. In eyes with long axial length, posterior staphyloma, or a history of scleral buckle, be cautious of the perforation risk with retrobulbar anesthesia.
QCan pain be felt during surgery under local anesthesia?
A
Local anesthesia alone can suppress somatic pain in the cornea, conjunctiva, and sclera, but may not completely suppress visceral pain originating from the iris and ciliary body. 7) If you feel pain, inform the surgeon, who can administer additional anesthesia or sedatives. Additionally, 3–18% of patients experience unpleasant visual sensations of light, color, or movement, but preoperative explanation can reduce anxiety.
Removal of vitreous opacities: Physically removes cloudy vitreous containing inflammatory exudates, blood, and infectious microorganisms, restoring the optical pathway.
Release of mechanical traction: Removing tangential traction from epiretinal membranes or proliferative membranes improves structural deformation of the macula. ILM peeling prevents recurrence of epiretinal membranes and provides the effect of internal limiting membrane peeling for macular edema. 5)
Removal of cytokines and growth factors: In endophthalmitis and diabetic retinopathy, VEGF and inflammatory cytokines accumulate in the vitreous cavity. Pars plana vitrectomy removes these humoral factors, suppressing neovascular proliferation and edema.
Physical support of tamponade: Gas and silicone oil support the retina and macula through buoyancy, assisting in reattachment of detached retina and closure of holes.
The relationship between intraocular gas volume and pressure follows Boyle’s law (P × V = constant). When atmospheric pressure decreases, volume increases, and in a closed eye, this manifests as elevated intraocular pressure. 1)
Foulsham et al. (2021) estimated that in eyes with 50% C₃F₈ fill, intraocular pressure increases by 10.8 mmHg per 1000 feet of altitude, reaching up to 42 mmHg at typical aircraft cruising altitude. 1) This pressure can exceed the ischemic threshold of the optic nerve and retinal vessels.
Gas Tamponade and High-Altitude/Low-Altitude Travel
High-altitude travel (including aircraft) causes gas expansion due to decreased atmospheric pressure, posing risks of increased intraocular pressure, arterial occlusion, and wound dehiscence. 1) Conversely, low-altitude travel can also cause intraocular pressure fluctuations, leading to risks of hypotony and retinal detachment. 1) Until the gas is completely absorbed, caution is needed for pressure changes in either direction.
The oculocardiac reflex is a reflex that causes a decrease in heart rate (≥20%) via the trigeminal nerve (afferent) and vagus nerve (efferent). It is triggered by manipulation or traction of the extraocular muscles and is common in strabismus surgery and scleral buckling procedures. Sub-Tenon’s anesthesia can prevent OCR by blocking the afferent pathway. Administration of atropine sulfate can also suppress its occurrence, but complete prevention is not possible.
Interaction Between Intraocular Gas and Nitrous Oxide
Nitrous oxide (laughing gas) can diffuse into intraocular gas bubbles, causing them to expand and rapidly increase intraocular pressure. This can lead to central retinal artery occlusion and blindness. It is essential to discontinue nitrous oxide at least 20 minutes before fluid-air exchange. 4) Intraocular gas is an important factor that limits the use of certain anesthetics, and strict prohibition of nitrous oxide use during other medical consultations is required.
Coughing or bucking under light general anesthesia can cause a sudden rise in intraocular pressure, leading to suprachoroidal hemorrhage (expulsive hemorrhage). To prevent this, maintaining deep anesthesia, combining local anesthesia, and suturing the scleral incision are recommended.
Somatic pain: Originating from the cornea, conjunctiva, and sclera. Can be managed with topical anesthesia or local infiltration.
Visceral pain: Originating from the iris and ciliary body. Cannot be suppressed with topical anesthesia alone; requires block anesthesia or general anesthesia.
QWhat is the oculocardiac reflex?
A
It is a reflex in which manipulation or traction of the extraocular muscles causes a decrease in heart rate of 20% or more via the trigeminal nerve (afferent) and vagus nerve (efferent). It is common in strabismus surgery and scleral buckling procedures. It can be prevented by sub-Tenon’s anesthesia (blocking the afferent pathway) or administration of atropine sulfate, but complete prevention is not possible, so intraoperative ECG monitoring is essential. 7)
7. Latest Research and Future Perspectives (Research Stage Reports)
The 2023 guideline of the Royal College of Ophthalmologists (RCOphth) positions the transition from 20G surgery to 27G MIVS as a historical turning point. 6)
According to the RCOphth FTMH Guideline (2023), the incidence of postoperative endophthalmitis is significantly lower with MIVS (23G/25G/27G) at 0.005% compared to 0.021% with 20G surgery. 6) The reintervention rate on the first postoperative day was reported as 4.7%.
This reduction in infection risk has promoted the adoption of MIVS and has been a major factor enabling outpatient surgery and local anesthesia. 6)
Quantitative Assessment of Air Travel and Intraocular Pressure Elevation
Foulsham et al. (2021) quantitatively evaluated the previously only qualitatively known risk of gas-filled eyes and air travel, and systematically reported for the first time the intraocular pressure rise (10.8 mmHg per 1000 feet) with 50% C₃F₈ fill. 1) This finding provides an important basis for preoperative informed consent.
Barth et al. (2023) reported that after PPV with silicone oil tamponade for fovea-sparing rhegmatogenous retinal detachment, 11 out of 22 cases experienced unexplained visual acuity loss of 3 or more lines. 2)Silicone oil is useful in difficult cases, but its necessity should be carefully assessed, and early removal should be considered when possible.
Itoh et al. (2023) reported a case of intraocular eyelash migration via the trocar after 25G MIVS. 3) The cause was oversight in the blind spot of the wide-angle viewing system, highlighting the importance of careful intraoperative observation and preoperative eyelash management.
Foulsham W, Bhatt U, Pasquale LR, et al. Intraocular pressure changes with gas-filled eyes during air travel: a prospective study. Retin Cases Brief Rep. 2021;15(5):564-567.
Barth T, Helbig H, Maerker D, Gamulescu MA, Radeck V. Unexplained visual loss after primary pars-plana-vitrectomy with silicone oil tamponade in fovea-sparing retinal detachment. BMC Ophthalmol. 2023;23:82. doi:10.1186/s12886-023-02823-6. PMID:36829157; PMCID:PMC9951486.
Itoh K. Intraocular eyelash after 25-gauge microincision vitrectomy surgery through a trocar: a case report. Case Rep Ophthalmol. 2023;14:1-6.
American Academy of Ophthalmology. Idiopathic Macular Hole Preferred Practice Pattern 2019. San Francisco: AAO; 2019.
American Academy of Ophthalmology. Epiretinal Membrane and Vitreomacular Traction Preferred Practice Pattern 2019. San Francisco: AAO; 2019.
Royal College of Ophthalmologists. Full-thickness Macular Hole Surgery Guideline. London: RCOphth; 2023.
American Academy of Ophthalmology. Cataract in the adult eye Preferred Practice Pattern. Ophthalmology. 2022;129(4):P1-P126.
European Society of Cataract and Refractive Surgeons (ESCRS). ESCRS clinical guideline for cataract surgery. 2024.
Copy the article text and paste it into your preferred AI assistant.
Article copied to clipboard
Open an AI assistant below and paste the copied text into the chat box.