Neovascular glaucoma (NVG) is a severe secondary glaucoma characterized by proliferation of fibrovascular tissue in the anterior chamber angle. Retinal ischemia is the main cause, leading to increased VEGF (vascular endothelial growth factor) and formation of new blood vessels on the iris and in the angle. The formation and contraction of fibrovascular tissue cause peripheral anterior synechiae (PAS), resulting in irreversible angle closure.
Iris rubeosis associated with retinal ischemia was reported from the first half of the 20th century, and the term “neovascular glaucoma” became established in the 1960s. Previously, various names such as hemorrhagic glaucoma, congestive glaucoma, and thrombotic glaucoma were used, but now NVG is the standard term.
The core of the pathology is the development of anterior segment neovascularization mediated by VEGF. Wakabayashi et al. performed intravitreal injection of bevacizumab in 41 consecutive cases of iris neovascularization and neovascular glaucoma secondary to ischemic retinal disease, and observed regression of iris neovascularization in almost all cases within 48 hours after administration 12). This rapid regression of neovascularization confirmed the major role of VEGF in anterior segment neovascularization.
QWhat kind of disease is neovascular glaucoma?
A
It is a refractory secondary glaucoma in which VEGF increases due to retinal ischemia, leading to the formation of new blood vessels in the iris and angle, resulting in elevated intraocular pressure. Diabetic retinopathy and retinal vein occlusion are the main causes. It is often resistant to drug therapy alone, and panretinal photocoagulation for retinal ischemia, combination with anti-VEGF drugs, and surgical intraocular pressure lowering are often required.
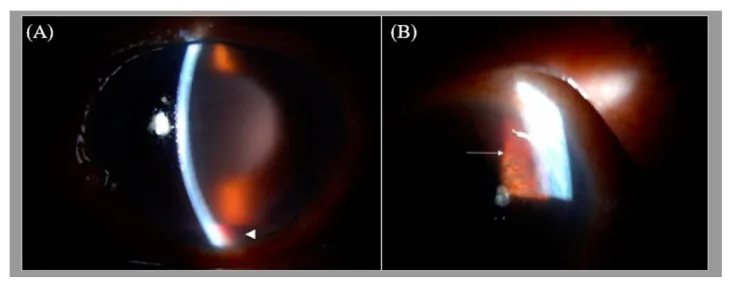
A shows severe anterior segment findings with corneal epithelial edema and hyphema, and B shows iris neovascularization. Typical findings that should not be missed in neovascular glaucoma can be easily grasped in a short time.
In the early stage with mild intraocular pressure elevation, there are no symptoms. As intraocular pressure rises, blurred vision, halos around lights, and eye pain occur. If the condition worsens rapidly, it may be accompanied by severe eye pain, headache, nausea, and vomiting, similar to an acute angle-closure glaucoma attack. On the other hand, if visual loss due to the underlying disease such as diabetic retinopathy or retinal vein occlusion precedes, the awareness of intraocular pressure elevation may be poor. When intraocular pressure becomes extremely high, bullous keratopathy may develop, and patients may visit the clinic complaining of foreign body sensation and eye pain.
For the staging of this disease, the four-stage classification by Shields is widely used. The clinical findings for each stage are as follows.
Pre-glaucoma stage to open-angle stage
Rubeosis iridis: Fine tufts of new blood vessels appear at the pupillary margin. Normal vessels run radially within the iris stroma, but new vessels show an irregular, tortuous pattern on the iris surface.
Angle neovascularization: Dendritic fine vessels are seen crossing the scleral spur and extending onto the trabecular meshwork. Intraocular pressure is normal to mildly elevated.
Fibrovascular membrane: Proliferates covering the trabecular meshwork, resulting in secondary open-angle glaucoma.
Angle-closure stage to absolute glaucoma stage
Uveal ectropion: The pigmented layer of the iris rolls forward onto the anterior surface due to contraction of the fibrovascular membrane. The iris surface becomes smooth.
Progression of peripheral anterior synechiae: The iris is pulled tent-like toward the trabecular meshwork, leading to synechial angle closure. Intraocular pressure rises markedly.
Absolute glaucoma stage: Visual function recovery is extremely difficult. Ocular pain due to high intraocular pressure becomes the main symptom.
In a retrospective study of 129 eyes, at the time of neovascular glaucoma diagnosis, 25% had open angle, 30% had partial closure, and 45% had complete closure2). Eyes with complete closure had worse visual acuity (median 20/4375) and higher intraocular pressure (median 59 mmHg)2). Since clinical findings alone cannot accurately predict the angle status, gonioscopy is essential in all cases2).
Among retinal vein occlusions, ischemic CRVO tends to cause iris rubeosis in about 3 months and is often called “100-day glaucoma” (90-day glaucoma). In proliferative diabetic retinopathy, long-term accumulation of retinal non-perfusion areas promotes VEGF production, and anterior segment neovascularization tends to progress slowly. In ocular ischemic syndrome, since internal carotid artery occlusion or stenosis is the underlying cause, auxiliary diagnosis using carotid artery ultrasound and head MRA is necessary.
Temkar et al. (2023) reported a case of a 30-year-old man who developed NVG after traumatic carotid-cavernous fistula (CCF) with combined retinal arteriovenous occlusion4). Severe retinal ischemia due to venous stasis and arterial insufficiency was the mechanism of NVG onset.
Zakaria et al. (2023) reported a case of a patient with cilioretinal artery-sparing CRAO who developed NVG within 2 weeks3). Neovascularization occurs in 18.2% of CRAO cases, with an average onset of 8.5 weeks3).
Fliney et al. (2021) reported a case of a 20-year-old man with choroidal malignant melanoma presenting initially as NVG7). VEGF and FGF production from the tumor caused NVG. About 2% of choroidal melanomas present with elevated intraocular pressure, most of which are NVG7).
QDoes having diabetes mean I will get neovascular glaucoma?
A
Proliferative diabetic retinopathy is the most common cause of NVG, accounting for about 53% of all NVG cases2). However, not all diabetic patients develop NVG; blood glucose control and management of retinal ischemia with retinal photocoagulation are important for prevention. Performing panretinal photocoagulation before the non-perfusion area becomes extensive is key to suppressing the development of anterior segment neovascularization.
Early detection of iris rubeosis is key to diagnosis. Since mydriatic agents can constrict blood vessels and make neovascularization less visible, slit-lamp microscopy and gonioscopy in the undilated state are important10). It is essential to observe the pupillary margin at high magnification and not miss early iris rubeosis.
In gonioscopy, neovascular vessels extending over the scleral spur onto the trabecular meshwork are observed. Sometimes, due to circumferential peripheral anterior synechiae, neovascular vessels may not be directly visible in the angle, but if iris rubeosis is present, the diagnosis should be considered and treatment initiated. During follow-up of diabetic retinopathy or retinal vein occlusion, regular undilated observation of the pupillary margin is required to detect fine neovascularization.
It is necessary to differentiate from diseases that present with rubeosis iridis. In Fuchs heterochromic iridocyclitis, abnormal vessels may appear on the iris surface, but angle closure is often absent, and uveal ectropion due to contraction of fibrovascular membrane is usually not observed. ICE syndrome (iridocorneal endothelial syndrome) is typically unilateral, accompanied by corneal endothelial abnormalities, and presents characteristic findings such as iris stromal atrophy, iris hole formation, and pupillary deviation, allowing differentiation. For differentiation from inflammatory secondary glaucoma, the presence of cells in the anterior chamber and keratic precipitates is helpful.
The treatment strategy involves improving retinal ischemia and controlling intraocular pressure in parallel 10). Addressing only one aspect will not calm the disease; both must be combined according to the disease stage.
Pre-glaucoma stage: If there is no vitreous hemorrhage, perform transpupillary PRP up to the far peripheral retina10).
When vitreous hemorrhage is present: Perform vitrectomy and endophotocoagulation up to the far peripheral retina.
Angle-closure stage: PRP alone is insufficient to lower intraocular pressure. Combine with surgical intraocular pressure-lowering surgery.
Anti-VEGF Agents
Open-angle stage: Perform PRP after regressing neovascularization by intravitreal injection of VEGF inhibitors
Rapid regression: In 41 consecutive cases by Wakabayashi et al., iris neovascularization regressed within 48 hours after IVB administration12)
Preoperative administration: Combining anti-VEGF drugs before surgery can reduce intraoperative and postoperative complications10)14) (evidence level 2B)
Intravitreal injection of anti-VEGF drugs (intravitreal bevacizumab: IVB) is the core of pharmacological treatment for neovascular glaucoma. A randomized controlled trial of intravitreal bevacizumab reported that IVB monotherapy for NVG significantly promoted intraocular pressure reduction and neovascular regression compared to the control group13). The duration of neovascular suppression is generally 3 to 6 weeks, and it is desirable to complete PRP within this period. In Japan, intravitreal injection of bevacizumab is off-label use, so it is essential to obtain approval from the ethics committee of each medical facility.
Pharmacological treatment is performed according to primary open-angle glaucoma10). Beta-blockers and carbonic anhydrase inhibitors, which suppress aqueous humor production, are theoretically highly effective. Prostaglandin analogs and alpha-2 adrenergic receptor agonists are also used in combination. Oral carbonic anhydrase inhibitors should be administered after confirming the absence of renal dysfunction. Intravenous infusion of hyperosmotic agents aims for temporary intraocular pressure reduction, but the effect is short-lived, and caution is required because of the risk of acute renal failure in patients with reduced renal function. Atropine sulfate eye drops and corticosteroid eye drops may be effective for reducing inflammation and pain10).
Pilocarpine (miotic agent), a parasympathomimetic, is often ineffective and may worsen the condition due to disruption of the blood-aqueous barrier, so it is not recommended10)11).
Trabeculectomy (with mitomycin C): This is the first choice for surgical intraocular pressure lowering treatment10). Concomitant use of the antimetabolite mitomycin C during surgery helps maintain long-term function of the filtering bleb. Performing IVB 1 to 7 days before surgery reduces intraoperative and postoperative hyphema and vitreous hemorrhage, and lowers the risk of filtering failure10). In Japan, mitomycin C is used off-label for this indication.
Tube shunt surgery: This became available in Japan in 2012. It is typically selected for cases where intraocular pressure cannot be lowered even with trabeculectomy, or for cases with active neovascularization, inflammation, or hyphema9). For neovascular glaucoma, anterior chamber insertion of the Ahmed glaucoma valve has a 1-year survival rate of 63.2%, 3-year 43.2%, and 5-year 25.2%, which decreases markedly over time. However, pars plana insertion after vitrectomy has been reported to have relatively good outcomes with 2- to 3-year survival rates of over 80%. A systematic review by Hwang et al. showed that adjunctive IVB combined with Ahmed glaucoma valve implantation improves intraoperative and postoperative hyphema and early intraocular pressure reduction outcomes 14).
Cyclophotocoagulation (transscleral or endoscopic): This is indicated for eyes with poor visual prognosis or when intraocular pressure control cannot be achieved with filtration surgery or tube shunt surgery 1)10). It aims to suppress aqueous humor production, but excessive coagulation can lead to extreme reduction in aqueous production, risking phthisis bulbi.
Laser trabeculoplasty: This is not only ineffective but also harmful for neovascular glaucoma 10).
Outflow reconstruction surgery (trabeculotomy): Its effectiveness for neovascular glaucoma has not been confirmed 10).
The following is a guide for treatment selection according to disease stage.
Stage I: Pre-glaucoma stage: If there is no vitreous hemorrhage, perform transpupillary PRP up to the far peripheral retina. If vitreous hemorrhage prevents clear fundus view, perform vitrectomy + endophotocoagulation.
Stage II: Open-angle stage: After regressing neovascularization with IVB, complete PRP. If sufficient laser treatment to the far peripheral retina is not possible, perform lens extraction and vitrectomy, and administer adequate endophotocoagulation. If intraocular pressure reduction is not achieved, consider trabeculectomy or tube shunt surgery.
Stage III: Angle-closure stage: In the angle-closure stage with uveal ectropion, even after IVB, intraocular pressure reduction is not achieved in about 90% of cases. Therefore, after thorough vitrectomy and endophotocoagulation, perform surgical intraocular pressure reduction such as trabeculectomy or tube shunt surgery.
Stage IV: Absolute glaucoma stage: Visual function recovery is extremely difficult. If ocular pain due to high intraocular pressure is present, perform drug therapy for intraocular pressure reduction or cyclophotocoagulation.
Before IVB was used, trabeculectomy was often accompanied by massive hyphema during and after surgery, frequently leading to filtration failure. Preoperative IVB reduces perioperative hyphema, and the rate of intraocular pressure control to 21 mmHg or lower is reported to be about 60%. Poor prognostic factors include age under 50 years and a history of vitrectomy. Particularly in young patients with angle-closure stage where peripheral anterior synechiae progress rapidly, postoperative outcomes are often poor. The recent widespread adoption of minimally invasive vitreous surgery has reduced conjunctival scarring, also contributing to improved outcomes of trabeculectomy.
QWhat surgical methods are available for neovascular glaucoma?
A
Mitomycin C-augmented trabeculectomy is the first choice, and it is desirable to perform it when neovascularization has subsided 10). For cases where intraocular pressure cannot be lowered even with trabeculectomy or where active neovascularization remains, tube shunt surgery (especially Ahmed glaucoma valve insertion into the pars plana) is selected 9). For eyes with poor visual prognosis, cyclophotocoagulation is performed. In any case, preoperative panretinal photocoagulation and anti-VEGF drug administration reduce perioperative complications 10)14).
When oxygen supply is insufficient due to retinal ischemia, retinal cells release angiogenic factors such as VEGF and IL-6. Normally, VEGF levels are balanced with the anti-angiogenic factor pigment epithelium-derived factor (PEDF). When this balance shifts toward VEGF dominance, endothelial cell activation, proliferation, and migration are promoted, leading to anterior segment neovascularization. It is known that VEGF concentration in aqueous humor is several tens of times higher in NVG eyes compared to healthy eyes, directly related to the development of anterior segment neovascularization.
Formation and Contraction of Fibrovascular Membrane
Neovascular vessels in neovascular glaucoma have thin walls, lack a muscular layer, and have deficient tight junctions, resulting in increased permeability. These new vessels are accompanied by a fibrovascular membrane consisting of proliferating myofibroblasts. Initially, the fibrovascular membrane spreads over the trabecular meshwork, increasing aqueous outflow resistance, presenting as secondary open-angle glaucoma. Subsequently, contraction of the membrane leads to flattening of the iris surface, uveal ectropion, and formation of peripheral anterior synechiae, eventually resulting in irreversible angle closure 1).
Initially, the fibrovascular membrane covers the trabecular meshwork, resulting in secondary open-angle glaucoma1)11). Subsequently, contraction of the membrane leads to peripheral anterior synechiae, transitioning to synechial angle-closure glaucoma. In phakic eyes, angle closure tends to progress more readily 2), and once this stage is reached, long-term intraocular pressure control becomes difficult with conventional filtration surgery alone. As long as the underlying retinal ischemia persists, neovascularization and contraction of the fibrovascular membrane continue to progress; therefore, suppression of the ischemic condition through PRP or anti-VEGF therapy is fundamental to treatment.
Wang et al. (2024) investigated predictors of angle status at diagnosis in 129 eyes with NVG 2). Eyes with complete closure had more severe visual acuity and intraocular pressure, but angle status could not be accurately predicted based on clinical features alone. Cases presenting to the emergency department had a higher frequency of complete closure, and eyes with a history of PRP or vitrectomy also tended to have more angle closure 2).
Soman et al. (2022) reported a case of rapid-onset NVG due to COVID-19-associated retinopathy 5). A 50-year-old man developed bilateral retinal vascular lesions three weeks after contracting COVID-19, and the right eye progressed to NVG within two weeks. Retinal vascular damage associated with a prothrombotic state was considered the mechanism. Complete regression of neovascularization and normalization of intraocular pressure were achieved with antiglaucoma medications and PRP5).
ALKhamees et al. (2023) reported an 11-year-old girl with Pierson syndrome (LAMB2 mutation) who developed spontaneous hyphema, vitreous hemorrhage, and neovascular glaucoma 8). Iris and angle neovascularization secondary to retinal ischemia was observed, and although cyclophotocoagulation was ultimately required, the eye progressed to phthisis bulbi8).
Pazos M, Traverso CE, Viswanathan A; European Glaucoma Society. European Glaucoma Society - Terminology and guidelines for glaucoma, 6th Edition. Br J Ophthalmol. 2025;109(Suppl 1):1-212. doi:10.1136/bjophthalmol-2025-egsguidelines. PMID:41026937.
Wang J, Kanter J, Qiu M. Predictors of anterior chamber angle status at the time of neovascular glaucoma diagnosis. American journal of ophthalmology case reports. 2024;36:102096. doi:10.1016/j.ajoc.2024.102096. PMID:39822766; PMCID:PMC11738042.
Zakaria NA, et al. Neovascular Glaucoma Complicating Central Retinal Artery Occlusion Despite Cilioretinal Artery Sparing. Cureus. 2023;15(8):e44339. doi:10.7759/cureus.43303.
Temkar S, Jayaseelan J, Deb AK, Kaliaperumal S. Neovascular glaucoma with combined retinal vascular occlusion in carotid cavernous fistula. BMJ case reports. 2023;16(4). doi:10.1136/bcr-2022-253197. PMID:37076195; PMCID:PMC10124193.
Soman M, Indurkar A, George T, Sheth JU, Nair U. Rapid Onset Neovascular Glaucoma due to COVID-19-related Retinopathy. Journal of current glaucoma practice. 2022;16(2):136-140. doi:10.5005/jp-journals-10078-1356. PMID:36128075; PMCID:PMC9452705.
Fliney G, Ahmed O, Young B, Teng C, Pointdujour-Lim R. Metastatic Choroidal Melanoma Presenting as Neovascular Glaucoma. Case reports in ophthalmology. 2021;12(3):791-796. doi:10.1159/000518804. PMID:34720979; PMCID:PMC8525261.
ALKhamees A, ALShemmari M. Case of Pierson syndrome presented with hyphema, vitreous haemorrhage and subsequent neovascular glaucoma. BMC Ophthalmol. 2023;23:82.
Gedde SJ, Vinod K, Wright MM, et al. Primary Open-Angle Glaucoma Preferred Practice Pattern. Ophthalmology. 2021 Jan;128(1):P71-P150. doi:10.1016/j.ophtha.2020.10.022. PMID:34933745.
European Glaucoma Society. European Glaucoma Society Terminology and Guidelines for Glaucoma, 5th Edition. Br J Ophthalmol. 2021 Jun;105(Suppl 1):1-169. doi:10.1136/bjophthalmol-2021-egsguidelines. PMID:34675001.
Wakabayashi T, Oshima Y, Sakaguchi H, Ikuno Y, Miki A, Gomi F, et al. Intravitreal bevacizumab to treat iris neovascularization and neovascular glaucoma secondary to ischemic retinal diseases in 41 consecutive cases. Ophthalmology. 2008;115(9):1571-1580.e3. PMID:18440643. doi:10.1016/j.ophtha.2008.02.026.
Yazdani S, Hendi K, Pakravan M, Mahdavi M, Yaseri M. Intravitreal bevacizumab for neovascular glaucoma: a randomized controlled trial. J Glaucoma. 2009;18(8):632-637. PMID:19826393. doi:10.1097/IJG.0b013e3181997211.
Hwang HB, Han JW, Yim HB, Lee NY. Beneficial effects of adjuvant intravitreal bevacizumab injection on outcomes of Ahmed glaucoma valve implantation in patients with neovascular glaucoma: systematic literature review. J Ocul Pharmacol Ther. 2015;31(4):198-203. doi:10.1089/jop.2014.0108.
Copy the article text and paste it into your preferred AI assistant.
Article copied to clipboard
Open an AI assistant below and paste the copied text into the chat box.