A glaucoma drainage device (GDD), also called an aqueous shunt or tube shunt, is an implant composed of a silicone tube and a plate. The tube is inserted into the eye, and the plate is fixed onto the sclera near the equator of the globe. Aqueous humor is directed through the tube to the plate outside the eye, where it is absorbed by surrounding tissues through a fibrous capsule that forms around the plate 4 to 6 weeks after surgery1).
It is considered a treatment option for glaucoma cases where conventional filtering surgery (trabeculectomy) fails to control intraocular pressure. The tube can be inserted into the anterior chamber or the vitreous cavity, and the choice depends on the presence of the vitreous and the target intraocular pressure.
In Japan, two types of devices are available under insurance coverage (since 2012): Baerveldt® glaucoma implant and Ahmed® glaucoma valve. The Ex-PRESS® glaucoma filtration device, which has no plate, is also approved12).
Cases where other filtering surgeries are technically difficult to perform
Refractory pediatric glaucoma: when angle surgery is ineffective3)
Traumatic glaucoma, aphakic/pseudophakic glaucoma, glaucoma after corneal transplantation2)
For primary open-angle glaucoma (POAG), GDD is not recommended as a first-line surgery. It should be considered in cases of reoperation. Evidence regarding normal-tension glaucoma (NTG) is insufficient, and further investigation is needed12).
QWhich patients are suitable for tube shunt surgery?
A
The main indications are cases where trabeculectomy with antimetabolites has failed, or cases with severe conjunctival scarring due to prior surgery12). It is also indicated for conditions where trabeculectomy is unlikely to succeed, such as neovascular glaucoma, uveitic glaucoma, and ICE syndrome. For primary open-angle glaucoma, it is not recommended as a first surgery but should be considered in reoperation cases.
Since GDD is a treatment for glaucoma itself, understanding the clinical features relevant to the indication is important. In cases with the following disease types or background factors, the success rate of trabeculectomy is reduced, and GDD is considered.
Conjunctival scarring: Due to chemical trauma, Stevens-Johnson syndrome, multiple conjunctival surgeries, etc.
In the PTVT Study (comparison in first-surgery eyes), the higher failure rate in the tube group compared to the TVT Study (which included reoperation eyes) is thought to be influenced by the younger age and higher proportion of Black patients in the PTVT group12).
GDDs are classified into two types based on the presence of an intraocular pressure-regulating valve.
Valved
Representative: Ahmed® Glaucoma Valve (AGV)
Mechanism: A pressure-regulating valve is built into the plate. The valve closes at intraocular pressure ≤8 mmHg, preventing early postoperative overfiltration
Advantages: Immediate intraocular pressure reduction postoperatively. No need for tube ligation or Sherwood slit creation. Low risk of hypotony
Disadvantages: Long-term intraocular pressure reduction is slightly inferior to non-valved types (maintaining IOP <18 mmHg at 5 years: approximately 50%)15)
Priming: Before surgery, irrigation fluid must be injected from the tube tip to confirm valve function
Nonvalved
Representative: Baerveldt® Glaucoma Implant
Mechanism: No valve mechanism. The tube is completely ligated intraoperatively with an absorbable suture (Vicryl®), and several Sherwood slits (temporary leakage holes) are created to ensure early partial outflow
Advantages: Superior long-term intraocular pressure reduction (maintaining IOP <18 mmHg at 5 years: approximately 70%). Achievable IOP is lower15)
Disadvantages: There is a period of elevated intraocular pressure for about 1 month postoperatively. Risk of hypotony is higher than valved types (4.5% vs 0.4%)12)
Postoperative management: For about 1 month until the absorbable suture dissolves, glaucoma eye drops are used concurrently for IOP control
The list of plate-type GDDs approved in Japan is shown below12).
Device
Model
Plate Area
Insertion Site
Notes
Baerveldt®
BG101-350
350 mm²
Anterior chamber
Standard size
Baerveldt®
BG103-250
250 mm²
Anterior chamber
Pediatric/short axial length
Baerveldt®
BG102-350
350 mm²
Pars plana
Eyes with prior vitrectomy
Ahmed®
FP7
184 mm²
Anterior chamber
Valve-regulated, most versatile
Ahmed®
FP8
96 mm²
Anterior chamber
Pediatric, short axial length
A plate-less GDD is the Ex-PRESS® glaucoma filtration device (length 2.6 mm, lumen 50 μm, stainless steel). It is inserted from under the scleral flap into the anterior chamber. Contraindications include angle-closure glaucoma, uveitis, and metal allergy. MRI up to 3 Tesla is considered safe12).
The choice between Baerveldt® and Ahmed® is based on the following criteria.
Cases aiming for lower intraocular pressure: Baerveldt® is indicated. It offers superior long-term IOP control, even considering the risk of postoperative complications.
Cases requiring immediate IOP reduction or where hypotony is dangerous: Ahmed® is indicated. This includes aphakic eyes, eyes with sutured IOL, eyes with history of expulsive hemorrhage, and uveitic glaucoma.
Long-term intraocular pressure control depends on the plate surface area. A larger plate area results in a larger surrounding fibrous capsule, allowing more aqueous humor absorption. The double-plate Molteno provided better intraocular pressure control than the single-plate, while in a comparison of 350 mm² and 500 mm² Baerveldt implants, the 350 mm² model was superior1).
QShould a valved or non-valved type be selected?
A
Even considering the risk of postoperative complications, Baerveldt® (non-valved type) is chosen for cases aiming for lower intraocular pressure. Ahmed® (valved type) is selected for cases requiring immediate postoperative pressure reduction or where hypotony is dangerous (e.g., aphakia, uveitic glaucoma). Meta-analysis shows that the mean postoperative intraocular pressure with Baerveldt® (13.2 mmHg) is significantly lower than with Ahmed® (15.8 mmHg)15), but the incidence of hypotony is higher with Baerveldt® (4.5% vs 0.4%)12).
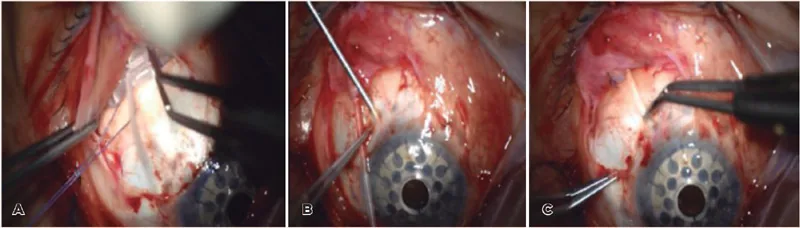
Long scleral tunnel technique for prevention of drainage tube-related complications during Ahmed glaucoma valve implantation. Medicine (Baltimore). 2023;102(42):e35449. Figure 2. PMCID: PMC10589554. License: CC BY 4.0.
Intraoperative photographs showing the key steps of Ahmed glaucoma valve implantation in nine panels (A–I). These correspond to the individual steps of tube insertion, plate fixation, and patch grafting discussed in section “5. Surgical Technique and Complication Management.”
Site selection: The superotemporal quadrant is the first choice. If placement is not possible due to existing surgical scars, the nasal or inferior quadrants may be considered; however, the inferior quadrant carries a higher infection risk, and the nasal quadrant is more prone to ocular motility disturbances, so these should be avoided whenever possible.
Conjunctival incision: A fornix-based incision is made, extending to expose two adjacent rectus muscles. The conjunctiva and subconjunctival tissue are dissected as far posteriorly as possible.
Plate fixation: The plate is inserted under two adjacent rectus muscles and sutured to the sclera with nylon sutures at a position 8–10 mm from the limbus.
Tube ligation (to prevent hypotony): The tube is completely ligated with an absorbable suture (Vicryl®) 2–4 mm anterior to the plate.
Sherwood slit creation (to prevent hypertension): Several temporary venting slits are made in the tube with a needle or blade to reduce immediate postoperative high intraocular pressure.
Tube trimming: The tube is trimmed with a bevel-up cut to a length that allows 2–3 mm insertion into the anterior chamber.
Tube insertion: A 23-gauge needle is used to create a puncture tract at the corneoscleral limbus parallel to the iris plane, and the tube is inserted into the anterior chamber.
Tube fixation and covering: The tube is fixed to the sclera with nylon sutures and covered with a patch graft material such as preserved sclera or cornea12).
Conjunctival closure: The conjunctiva is sutured and covered with absorbable sutures to complete the procedure.
The basic technique is similar to that for the Baerveldt® implant, but the following points differ.
Priming: Irrigating solution is injected from the tube tip to confirm that the pressure-regulating valve opens.
Conjunctival incision size: Because the plate is smaller, a narrower incision than for the Baerveldt® implant is possible.
No ligation or venting hole required: Since the pressure-regulating valve prevents early postoperative hypotony, tube ligation or creation of a Sherwood slit is unnecessary.
Steroid eye drops: Tapered over approximately 6 months.
Baerveldt® postoperative hypertensive phase: Intraocular pressure remains around 20 mmHg for about one month until the absorbable suture ligating the tube dissolves. Pressure is managed with glaucoma eye drops or oral medications, and the pressure often decreases after 1–2 months. Another method involves passing a nylon suture through the tube and removing it to adjust pressure during early hypertension.
To prevent early postoperative hypotony with non-valved devices, the following techniques are used.
Intraluminal stent: A 4-0 or 5-0 suture is inserted into the tube lumen and removed under slit lamp after capsule formation.
External ligation: The tube is ligated with an absorbable suture (7-0 or 8-0 Vicryl®). A venting slit may be added to allow early partial outflow.
Two-stage surgery: In the first stage, only the plate is fixed; after 4–6 weeks, once capsule formation is complete, the tube is inserted into the anterior chamber.
Tube exposure: A complication specific to GDD, occurring in 4.3–14.3% of cases7). Tube exposure through conjunctival erosion carries a risk of endophthalmitis and requires early repair8). Patch grafting or scleral tunnel coverage is performed. To prevent tube exposure, patch materials such as preserved sclera or cornea, or a partial-thickness scleral flap should be used to cover the tube12).
Hypotony: More common with non-valved devices1). The incidence of hypotony is 4.5% with Baerveldt® and 0.4% with Ahmed®12). If the anterior chamber depth is maintained, conservative management is possible; however, if there is lens-cornea touch, anterior chamber reformation with viscoelastic injection is needed.
Tube obstruction: Can occur due to fibrin, iris, hemorrhage, or vitreous. For anterior chamber tubes, Nd:YAG laser is used; for vitreous cavity tubes, vitrectomy is performed6). In cases of corneal opacity, intraocular endoscopy is useful for identifying and treating the cause6).
Diplopia and ocular motility disturbance: Occurs in about 5% of cases. Placement of the plate in the superonasal quadrant should be avoided. After 6 months of observation, management with prism glasses or surgery is considered.
Corneal endothelial damage: If the tube tip is close to the corneal endothelium, long-term endothelial cell loss and bullous keratopathy may occur1). In elderly patients, simultaneous cataract surgery may be recommended.
Tenon cyst (encapsulation): Fibrous capsule thickening around the plate leads to elevated intraocular pressure. The frequency is 40–80% with AGV and 20–30% with non-valved devices10). It often appears as a hypertensive phase 3 weeks to 3 months postoperatively.
Large filtering bleb: Rarely, a large filtering bleb forms around the plate5). It is classified into an anterior expansion type (foreign body sensation, cosmetic issues) and a posterior expansion type (eye deviation, diplopia; T2-weighted MRI evaluation is useful)5). There have also been reports of staphyloma formation after GDD removal11).
QHow often do complications of glaucoma drainage devices occur?
A
In the 5-year data from the TVT Study, the incidence of serious complications was 34% in the tube group and 36% in the trabeculectomy group13). Major complications include tube exposure (4.3–14.3%)7), hypotony (Baerveldt® 4.5%, Ahmed® 0.4%)12), and diplopia (approximately 5%). The types of complications differ between the two procedures: tube shunt surgery is associated with more corneal endothelial damage and tube exposure, while trabeculectomy is associated with more bleb leakage, hypotony maculopathy, and bleb infection13).
The choice between tube shunt surgery and trabeculectomy should be made based on a comprehensive assessment of the treated eye, patient background, and the surgeon’s proficiency with each technique12).
For primary open-angle glaucoma as an initial surgery, some reports suggest that trabeculectomy may achieve lower intraocular pressure more easily.
In eyes with prior surgery or secondary glaucoma, tube shunt surgery may be advantageous.
The decision should be individualized, considering target intraocular pressure, conjunctival scarring, corneal endothelium, history of vitrectomy, and ease of postoperative management.
There is no significant difference in intraocular pressure control between the two procedures, and no significant difference in the incidence of serious complications that impair visual function. However, complications related to hypotony and postoperative infection are more common with trabeculectomy, while implant exposure and corneal endothelial damage are more common with tube shunt surgery12).
No implant required: No foreign body, and no risk of tube exposure1)
Corneal endothelium: Lower risk of long-term corneal endothelial damage
Cost: Cost per QALY compared to conservative treatment is $8,289 for trabeculectomy and $13,896 for Baerveldt®, with trabeculectomy being lower cost12)
Advantages of GDD
High-risk cases for filtration surgery: Suitable for conjunctival scarring and secondary glaucoma1)
Postoperative management: Relatively lower burden of postoperative care
Reoperation: In the TVT Study at 5 years, additional glaucoma surgery was significantly more frequent in the trabeculectomy group (p=0.025)13)
Baerveldt 350 vs TLE+MMC (previously operated eyes)
Cumulative failure rate: tube 29.8% vs TLE 46.9% (p=0.02)13)
PTVT Study (3 years)
Baerveldt 350 vs TLE+MMC (primary surgery eyes)
Cumulative failure rate: tube 33% vs TLE 28% (no significant difference)14)
ABC/AVB pooled (5 years)
Ahmed vs Baerveldt
Baerveldt 13.2 mmHg vs Ahmed 15.8 mmHg (p<0.001)15)
TVT Study (Tube Versus Trabeculectomy Study) is a multicenter RCT of eyes with prior cataract surgery or trabeculectomy13). At 5 years, the tube group had a higher success rate than the trabeculectomy group. Intraocular pressure reduction, medication use, serious complications, and vision loss were similar, but the number of additional glaucoma surgeries was significantly higher in the trabeculectomy group (p=0.025)13). Postoperative QOL assessment using the NEI VFQ-25 showed no significant difference between groups12).
PTVT Study (Primary TVT Study) is an RCT of eyes undergoing first-time surgery14). At 3 years, success rates were similar between groups, but lower intraocular pressure was achieved with fewer medications in the trabeculectomy group14).
ABC/AVB Study is a multicenter RCT comparing Ahmed and Baerveldt15). Over 5 years of follow-up, the Baerveldt group was superior to the Ahmed group in intraocular pressure reduction and medication reduction, but serious complications were fewer in the Ahmed group15). The incidence of hypotony after Baerveldt surgery (4.5%) was significantly higher than with Ahmed (0.4%) (p=0.002)12).
In a comparative study of Ahmed vs trabeculectomy, cumulative success rates (at 41–52 months) were 69.8% in the Ahmed group and 68.1% in the trabeculectomy group, with no significant difference. Tube exposure was more common in the Ahmed group, while bleb leakage and bleb infection tended to be more frequent in the trabeculectomy group16).
Intraoperative use of mitomycin C (MMC) in GDD has been examined in several RCTs but has not been shown to improve success rates1). Prolonged hypotony and increased complications have been reported, and antifibrotic agents are not generally used in GDD.
In pediatric glaucoma, angle surgery (goniotomy or trabeculotomy) is the first choice, but its efficacy is limited in secondary glaucoma, and GDD may be used as primary treatment3).
Stallworth et al. conducted a systematic review and meta-analysis of 32 studies (1,221 eyes, 885 children)3). The mean preoperative intraocular pressure was 31.8±3.4 mmHg. The pooled mean IOP at 12 months postoperatively was 16.5 mmHg (95% CI: 15.5–17.6), with a success rate of 0.87 (95% CI: 0.83–0.91). At 24 months, the mean IOP was 17.6 mmHg and the success rate was 0.77 (95% CI: 0.71–0.83). The success rate decreased to 0.54 at 48 months, 0.60 at 60 months, and 0.37 at 120 months. There was no significant difference in success rates between Ahmed and Baerveldt at 12 and 24 months. The most common complications were shallow anterior chamber (13.6%), hypotony (11.7%), and choroidal detachment (8.3%). Ninety percent of the studies used Ahmed, and data on Baerveldt in children are limited.
In children, the risk of tube or plate exposure is high. This is attributed to frequent eye rubbing and a strong immune response. In pediatric secondary glaucoma, particularly after cataract surgery, surgical outcomes are poor, and GDD may eventually be required12).
QWhich is better: glaucoma drainage devices or trabeculectomy?
A
The optimal choice depends on the patient’s condition. For primary open-angle glaucoma as an initial surgery, the PTVT Study showed that trabeculectomy achieved lower intraocular pressure14). On the other hand, in eyes with prior surgery or secondary glaucoma, the TVT Study favored tube shunt surgery13). In clinical practice, the surgical technique is selected based on the treated eye, patient background, and surgeon’s expertise12).
A tube coverage method using an autologous scleral tunnel that eliminates the need for a patch graft has been developed.
Tanito et al. created a microincision scleral tunnel (MIST) using a 1 mm crescent knife and applied it for tube insertion into three sites: the anterior chamber, ciliary sulcus, and vitreous cavity4). This technique requires no sutures, can shorten surgical time, and resulted in no postoperative tube exposure.
Miura et al. reported a scleral tunnel creation method using a 22-gauge needle, with no tube exposure observed during a maximum follow-up of 21 months7).
These techniques offer advantages in avoiding difficulties in obtaining patch graft materials and the risk of viral infection.
Kawashima et al. identified obstruction of the tube tip by fibrous tissue using an intraocular endoscope in cases of failed AGV where slit-lamp examination was difficult due to corneal opacity, and achieved intraocular pressure reduction by removing the tissue 6). Endoscopy was shown to be useful for diagnosing GDD failure in cases with corneal opacity.
Katsev et al. inserted an AGV in a case with combined outflow obstruction and reduced aqueous production, where the therapeutic range of eye drops was extremely narrow, and stabilized unstable intraocular pressure by creating a compliant outflow pathway 9). Intraocular pressure was maintained at 8–10 mmHg without medication for 15 months.
Intraocular pressure reduction by GDD is achieved through the following pathways:
Tube: A silicone tube that guides aqueous humor from the eye to the plate
Plate: Fixed near the equator of the eye. Provides a space to store aqueous humor guided through the tube
Fibrous capsule: Connective tissue formed around the plate 4–6 weeks after surgery. Aqueous humor is absorbed from the outer surface of the capsule into surrounding tissues (Tenon’s capsule and subconjunctival tissue)
Effect of plate area: A larger plate area results in a larger surrounding capsule, allowing absorption of more aqueous humor
Immediately after surgery: Since the tube is ligated with absorbable suture, there is no aqueous flow to the plate. Only minimal leakage through the Sherwood slit
Approximately 1 month after surgery: The absorbable suture dissolves, and aqueous flow to the plate begins. Intraocular pressure starts to decrease from this period
2–3 months after surgery: The fibrous capsule around the plate matures, and outflow resistance stabilizes
Long-term: As capsular fibrosis progresses, outflow resistance may increase, leading to elevated intraocular pressure (Tenon’s cyst).
The Ahmed® valve is a unidirectional valve that utilizes the Venturi effect; theoretically, the valve closes when intraocular pressure is 8 mmHg or lower. This prevents excessive filtration immediately after surgery and reduces the risk of hypotony-related complications (e.g., choroidal detachment, hypotony maculopathy). However, because the plate area is smaller than that of the Baerveldt® implant, the final achievable intraocular pressure is somewhat inferior to that of the Baerveldt®.
Pazos M, Traverso CE, Viswanathan A; European Glaucoma Society. European Glaucoma Society - Terminology and guidelines for glaucoma, 6th Edition. Br J Ophthalmol. 2025;109(Suppl 1):1-212. doi:10.1136/bjophthalmol-2025-egsguidelines. PMID:41026937.
Gedde SJ, Vinod K, Wright MM, et al. Primary Open-Angle Glaucoma Preferred Practice Pattern. Ophthalmology. 2021 Jan;128(1):P71-P150. doi:10.1016/j.ophtha.2020.10.022. PMID:34933745.
Stallworth JY, O’Brien KS, Han Y, Oatts JT. Efficacy of Ahmed and Baerveldt glaucoma drainage device implantation in the pediatric population: A systematic review and meta-analysis. Surv Ophthalmol. 2023;68(4):578-590. doi:10.1016/j.survophthal.2023.01.010. PMID:36740196; PMCID:PMC10293048.
Tanito M, Ohtani H, Ida C, et al. Tube Insertion of Ahmed Glaucoma Valve Using a Micro-incision Scleral Tunnel Technique. Cureus. 2024;16(12):e75899. doi:10.7759/cureus.75899.
Ugarte R, Sugihara K, Sano I, Murakami K, Iida M, Shimada A, et al. Two different types of giant bleb formation following Ahmed Glaucoma valve implantation. American journal of ophthalmology case reports. 2024;33:102008. doi:10.1016/j.ajoc.2024.102008. PMID:38374947; PMCID:PMC10875191.
Kawashima R, Baba K, Matsushita K, Soma T, Kurashige M, Umeda D, et al. Intraocular Endoscopy Resolved Tube Occlusion of an Ahmed Glaucoma Valve. Case reports in ophthalmology. 2021;12(2):706-711. doi:10.1159/000518286. PMID:34594208; PMCID:PMC8436709.
Miura Y, Fukuda K, Yamashiro K. A Novel Scleral Tunnel Technique for the Prevention of Ahmed Glaucoma Valve Tube Exposure. Cureus. 2025;17(2):e79290. doi:10.7759/cureus.79290. PMID:40125231; PMCID:PMC11927520.
Mansoori T. Management of Ahmed glaucoma valve tube exposure after scleral patch graft shrinkage. Indian J Ophthalmol. 2022;70(9):3432. doi:10.4103/ijo.ijo_623_22.
Katsev B, Campagna G, Liu JC. Ahmed glaucoma valve implantation in a case of volatile intraocular pressure and preoperative hypotony. Am J Ophthalmol Case Rep. 2025;38:102285. doi:10.1016/j.ajoc.2025.102285.
Goel R, Gaonker T, Arya D, Golhait P. Outcome of combined single-loop fixation of intraocular lens with Ahmed glaucoma valve implantation. BMJ case reports. 2023;16(6). doi:10.1136/bcr-2022-254240. PMID:37380374; PMCID:PMC10410958.
Kolipaka PG, Krishnamurthy R, Bagga B. Unusual sequelae of staphyloma following Ahmed glaucoma valve explantation and its management. BMJ case reports. 2021;14(3). doi:10.1136/bcr-2020-239585. PMID:33758043; PMCID:PMC7993286.
Gedde SJ, Schiffman JC, Feuer WJ, Herndon LW, Brandt JD, Budenz DL, et al. Treatment outcomes in the Tube Versus Trabeculectomy (TVT) study after five years of follow-up. American journal of ophthalmology. 2012;153(5):789-803.e2. doi:10.1016/j.ajo.2011.10.026. PMID:22245458; PMCID:PMC4460598.
Gedde SJ, Feuer WJ, Lim KS, et al; Primary Tube Versus Trabeculectomy Study Group. Treatment outcomes in the primary tube versus trabeculectomy study after 3 years of follow-up. Ophthalmology. 2020;127(3):333-345. doi:10.1016/j.ophtha.2019.10.002.
Christakis PG, Zhang D, Budenz DL, et al; ABC-AVB Study Groups. Five-year pooled data analysis of the Ahmed Baerveldt comparison study and the Ahmed versus Baerveldt study. Am J Ophthalmol. 2017;176:118-126. doi:10.1016/j.ajo.2017.01.003.
Wilson MR, Mendis U, Paliwal A, Haynatzka V. Long-term follow-up of primary glaucoma surgery with Ahmed glaucoma valve implant versus trabeculectomy. American journal of ophthalmology. 2003;136(3):464-70. doi:10.1016/s0002-9394(03)00239-3. PMID:12967799.
Copy the article text and paste it into your preferred AI assistant.
Article copied to clipboard
Open an AI assistant below and paste the copied text into the chat box.