The Xen gel stent (Xen Glaucoma Treatment System) is a subconjunctival filtration device classified as a minimally invasive glaucoma surgery (MIGS). It directs aqueous humor from the anterior chamber directly to the subconjunctival space, forming a filtration bleb to lower intraocular pressure (IOP).
It was developed by Allergan (now AbbVie). It received CE marking in Europe in 2013 and FDA approval in the United States in 2016. As of February 2019, it is not yet approved in Japan.
The main structural features of the XEN45 are as follows.
Material: Porcine dermis-derived gelatin (cross-linked with glutaraldehyde). It is hydrophilic and flexible, softening within 1–2 minutes upon contact with aqueous humor to conform to tissue.
Dimensions: Total length 6 mm, inner lumen diameter 45 μm, outer diameter 150 μm.
Delivery system: Inserted via a single-use 27G preloaded injector.
Fluid dynamics design: Based on Hagen-Poiseuille law, the resistance of the tube itself achieves a steady-state IOP of 6–8 mmHg.
Variations: In addition to the XEN45, the XEN63 with a lumen of 63 μm and the XEN140 with 140 μm were designed, but only the XEN45 has received FDA approval6).
The XEN45 and PreserFlo MicroShunt are currently available devices as plate-free bleb-forming shunts6). Unlike traditional trabeculectomy, they do not require creation of a conjunctival or scleral flap.
With the widespread adoption of MIGS, surgical intervention has become possible at an earlier stage even for mild to moderate glaucoma8). Among these, the XEN gel stent has a relatively broad indication range and is also used for moderate to advanced glaucoma.
QHow is the XEN gel stent different from trabeculectomy?
A
Trabeculectomy is a conventional method that creates a conjunctival and scleral flap to form an outflow pathway for aqueous humor. The XEN gel stent minimizes conjunctival incision and is placed directly from the anterior chamber using an injector. While surgery and recovery times are shorter, some reports indicate that trabeculectomy achieves a higher rate of low target IOP. See the section “Efficacy and Clinical Outcomes” for details.
FDA-approved indications are for the following types refractory to maximum tolerated medical therapy6):
Primary open-angle glaucoma (POAG)
Pseudoexfoliation glaucoma
Pigmentary glaucoma
Refractory open-angle glaucoma with previous unsuccessful glaucoma surgery
In Europe, the indication is for all open-angle glaucoma with unsuccessful medical therapy. It can also be performed simultaneously with cataract surgery6), and may be indicated for moderate to advanced glaucoma6).
Conjunctival scarring or pterygium in the target quadrant
Keloid tendency
Allergy to porcine-derived products or glutaraldehyde
Relative contraindications include thin or unhealthy conjunctiva, history of vitrectomy or failed filtering bleb surgery, high myopia, congenital glaucoma, and secondary glaucoma6).
Key considerations in patient selection are as follows.
Baseline IOP: Higher baseline IOP tends to result in greater IOP reduction (p<0.001).
Anticoagulant use: Patients on anticoagulants have a higher risk of bleeding complications (10.1% vs. 3.7%), and adequate preoperative risk explanation is necessary4).
QCan Xen gel stent surgery be performed while taking anticoagulants?
A
Surgery itself is possible, but reports indicate that the risk of bleeding complications is approximately 2.7 times higher (10.1% vs. 3.7%) in patients using anticoagulants4). There have also been case reports of suprachoroidal hemorrhage (SCH), requiring individual risk assessment by the attending physician and thorough explanation. For details, see the “Complications and Management” section.
3. Surgical Technique and Perioperative Management
This is the most common surgical technique. The main steps are as follows.
Marking is performed 2.5–3.0 mm posterior to the superonasal conjunctival limbus.
Mitomycin C (MMC) is injected subconjunctivally.
After corneal incision, the anterior chamber is filled with ophthalmic viscosurgical device (OVD).
A 27G injector needle is inserted, traversing the anterior chamber, and passed through the scleral wall above the trabecular meshwork under gonioscopy.
The stent is positioned approximately 1 mm in the anterior chamber, 3 mm in the scleral wall, and 2 mm under the conjunctiva.
There are closed approaches (conjunctival advancement and scleral tunnel creation) and open approaches (conjunctival incision with MMC application via sponge or injection). Compared to ab interno, OVD is not required, and stent placement is considered more precise. Some reports have reduced needling rates to 11.8%.
After injecting air subconjunctivally, additional OVD is injected to dissect Tenon’s capsule and create a pocket for stent placement. Caution is needed regarding mitomycin C toxicity, as cases of corneal epithelial toxicity due to MMC accumulation in the presence of OVD have been reported1).
Mitomycin C suppresses subconjunctival fibrosis and is essential for long-term maintenance of the filtering bleb. It is considered key to the success of the Xen gel stent 7).
There is no significant difference in IOP-lowering effect or complication rate between 0.01% and 0.02% mitomycin C 1).
Higher doses of mitomycin C provide better IOP reduction, but a balance with the risk of bleb leakage and hypotony is necessary 6).
Injection at a distance of 8 mm or more from the limbus is recommended 1).
Postoperative day 1 IOP > 10 mmHg is a predictor of future needling 5), and early evaluation with AS-OCT improves the quality of postoperative management.
Postoperative needling is the most common postoperative procedure for the Xen gel stent.
The needling rate within 12 months is reported to be 46.2%.
The rate of requiring bleb management within 18 months reaches 40.9% 2).
Encapsulated blebs and fibrosis are observed in up to 32% of cases 2).
When postoperative IOP exceeds 20 mmHg, the probability of needing needling is approximately 80%.
AS-OCT-guided needling is effective when Tenon’s capsule compression is suspected, and can be performed while confirming the relationship between the stent opening and surrounding tissues5).
Cause: Fibrin clots, iris pigment granules, and breakdown products of inflammation and hemorrhage are the main causes of obstruction2).
Priority of management: Confirm with gonioscopy → YAG laser → YAG laser iridotomy → needling → if unsuccessful, consider trabeculectomy or tube shunt2).
Prognosis: In one report, all 4 cases required XEN removal and alternative surgery2). Cases have also been reported where fibrin obstruction was confirmed on AS-OCT and resolved spontaneously with intensified steroids5).
Suprachoroidal Hemorrhage
Characteristics: A rare but serious complication resulting from postoperative hypotony4).
Risk factors: Anticoagulant use is an important risk factor. A case has been reported of an 86-year-old patient on anticoagulants who developed kissing SCH requiring surgical drainage4).
Clinical significance: This report is the 4th case of SCH after Xen in the literature and the first reported to require surgical drainage4).
Avascular bleb, corneal stromal opacity, and ptosis have been reported as mitomycin C toxicity1).
In the XEN air technique, mitomycin C may accumulate in the presence of OVD, potentially causing corneal epithelial toxicity1).
QWhat is postoperative needling?
A
It is a procedure performed in the outpatient setting using a needle (usually 26-30G) to release adhesions around the bleb when the bleb becomes fibrotic or encapsulated and intraocular pressure rises again. It is required in approximately 46% of cases within 12 months and is recognized as a frequent postoperative procedure specific to the Xen gel stent.
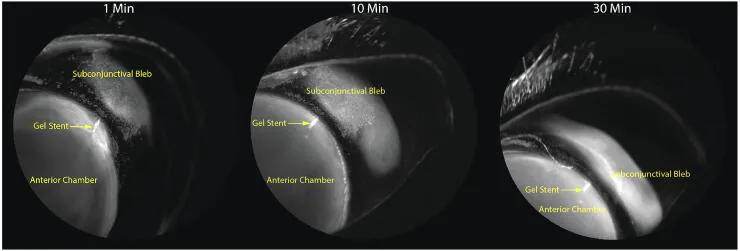
Susan S Lee; Saumya Nagar; Lakshmi Rajagopalan; et al. Using a Novel, Subconjunctival, Sustained-Release Mitomycin C Formulation in a Rabbit Model of Filtration Surgery with Gel Stent Implantation. Journal of Ocular Pharmacology and Therapeutics. 2024 Jun 17. Figure 5. PMCID: PMC11296147. License: CC BY.
Cross-sectional images showing the bleb and anterior chamber stent position over time after XEN gel stent placement. Postoperative bleb formation and temporal changes in stent position are depicted as cross-sectional images.
Multiple studies have reported the intraocular pressure lowering effect of the XEN gel stent.
In a meta-analysis, the mean IOP difference before and after XEN was −7.80 mmHg, and the mean medication number difference was −1.99. A reduction in the number of medications was confirmed in all studies10).
In a systematic review by Panarelli et al. (2023), multiple cohorts receiving XEN gel stent showed consistent IOP reduction and decrease in the number of eye drops from before to after surgery10).
In a systematic review and meta-analysis of MIGS for angle-closure disease by Paik et al. (2025), Sng et al. (19 eyes, primary angle-closure glaucoma) reported improvement from preoperative IOP 21.7±3.7 mmHg to 11.7±3.0 mmHg at 1 year (medication count 1.4→0.2), and Gabbay et al. (13 eyes) reported improvement from preoperative 24.6 to 16.4 mmHg at 1 year (medication count 2.9→0.6)9).
In the AAO Preferred Practice Pattern pivotal trial, IOP at 1 year was reported to reach the midteens7).
Lindland et al. (2021) reported a case of aniridia-related glaucoma (60-year-old male) treated with a Xen gel stent, where IOP decreased from 30 mmHg (on 4 medications) preoperatively to 12 mmHg (on 1 medication) at 2 years. Needling was not required 3).
At 12 months of follow-up, no statistically significant difference was observed in IOP reduction or medication reduction 2). However, trabeculectomy was superior in achieving low target IOP (≤12 mmHg). The Xen gel stent has the advantage of being a minimally invasive MIGS procedure.
The Xen gel stent bypasses the trabecular meshwork and Schlemm’s canal, directing aqueous humor directly from the anterior chamber to the subconjunctival space near the limbus. It can provide an effective outflow pathway even in cases with obstructed Schlemm’s canal 9).
The formed filtering bleb absorbs aqueous humor through the following pathways:
Evaporation through the conjunctival epithelium
Absorption into surrounding blood and lymphatic vessels
Alternative pathway via microcysts (successful filtering blebs have large cystic spaces)
Porcine gelatin material: Uses glutaraldehyde-crosslinked porcine dermal gelatin. Excellent hydrophilicity and flexibility, with high tissue compatibility. Non-inflammatory, low risk of migration and erosion.
Softening by aqueous humor: Softens within 1–2 minutes upon contact with aqueous humor, conforming to the shape of adjacent tissues. This reduces friction and tissue damage.
Fluid Dynamics Design
Hagen-Poiseuille law: Flow rate in a tube is proportional to the fourth power of the lumen radius and inversely proportional to length. The 45 μm lumen of the XEN45 utilizes this relationship and is designed to achieve a steady-state IOP of 6–8 mmHg.
Lumen size optimization: The 45 μm lumen diameter is optimized to achieve sufficient IOP reduction while avoiding hypotony.
QWhy is porcine-derived gelatin used as the material?
A
Porcine dermal gelatin is a material with excellent hydrophilicity, flexibility, and biocompatibility. It softens quickly upon contact with aqueous humor and conforms to tissue shape. Being non-inflammatory, it suppresses fibrosis around the stent due to foreign body reaction and has low risk of migration and erosion. However, allergy to porcine-derived products is a contraindication, so preoperative confirmation is necessary.
7. Latest Research and Future Perspectives (Research-stage Reports)
This technique involves injecting air under the conjunctiva to dissect Tenon’s capsule and create a pocket for stent placement. It is expected to reduce the needling rate, but attention to the risk of corneal toxicity due to mitomycin C accumulation has been reported 1).
Systematization of postoperative management using anterior segment OCT is progressing. It visualizes the relationship between the stent opening and surrounding tissues, aiding in the identification of fibrin occlusion and the determination of needling indications 5). An IOP >10 mmHg on postoperative day 1 has been identified as a predictor of future needling, helping in early intervention decision-making 5).
Use of the Xen gel stent in special indications where conventional surgery is difficult, such as aniridia-related glaucoma3) and uveitic glaucoma1), is accumulating at the case report level.
Management of Lumen Occlusion and Long-Term Outcomes
Knowledge about the mechanisms and management of lumen occlusion is accumulating 2). Long-term outcome data of 3 years or more are beginning to be reported, and evaluation of long-term efficacy and safety is progressing 9).
QHow does AS-OCT help in postoperative management?
A
Anterior segment OCT (AS-OCT) can visualize the relationship between the stent opening and surrounding tissues as tomographic images. It is useful for differentiating the cause of outflow obstruction, such as fibrin occlusion, compression by Tenon’s capsule, or encapsulation of the filtering bleb, and supports the determination of needling indications and sites 5). Evaluation with AS-OCT from the early postoperative period is recommended.
Baeg JY, Choi HS, Lee SH. A case of mitomycin C toxicity after XEN gel stent implantation with the XEN air technique in a glaucoma patient. BMC Ophthalmol. 2023;23:407.
C Amarasekera D, A Shankar V, Razeghinejad R. XEN Gel Stent Failure Due to Luminal Obstruction. Journal of ophthalmic & vision research. 2024;19(3):386-391. doi:10.18502/jovr.v19i3.9404. PMID:39359526; PMCID:PMC11443999.
Lindland A, Michelet JTE, Slagsvold JE. Use of the XEN gel implant in a patient with aniridia-associated glaucoma. Am J Ophthalmol Case Rep. 2021;22:101080.
Wang K, Wang JC, Sarrafpour S. Suprachoroidal Hemorrhage after XEN Gel Implant Requiring Surgical Drainage. Journal of current glaucoma practice. 2022;16(2):132-135. doi:10.5005/jp-journals-10078-1378. PMID:36128082; PMCID:PMC9452709.
Chen YC, Ko YC, Liu CJ. Optical coherence tomography-guided early postoperative management of XEN Gel implant. Taiwan journal of ophthalmology. 2022;12(4):495-498. doi:10.4103/tjo.tjo_17_22. PMID:36660131; PMCID:PMC9843565.
European Glaucoma Society / World Glaucoma Association. Surgical Innovation for Glaucoma. 2023.
Gedde SJ, Vinod K, Wright MM, et al. Primary Open-Angle Glaucoma Preferred Practice Pattern. Ophthalmology. 2021 Jan;128(1):P71-P150. doi:10.1016/j.ophtha.2020.10.022. PMID:34933745.
Reporting Clinical Endpoints in Studies of MIGS. Ophthalmology. 2025.
Paik D, et al. Outcomes and complications of minimally invasive glaucoma surgery in primary angle closure disease: a systematic review and meta-analysis. Clin Ophthalmol. 2025;19:485-507.
Panarelli JF, Vera V, Sheybani A, et al. Intraocular pressure and medication changes associated with Xen gel stent: a systematic review of the literature. Clin Ophthalmol. 2023;17:25-46.
Copy the article text and paste it into your preferred AI assistant.
Article copied to clipboard
Open an AI assistant below and paste the copied text into the chat box.