Trabeculectomy is a surgery in which a scleral flap is created, and the limbal tissue under the flap is excised to allow aqueous humor to filter into the episcleral space. A characteristic feature is that the scleral flap is sutured to adjust the amount of aqueous filtration. The filtered aqueous humor is absorbed by the conjunctival tissue, forming a blister called a bleb.
It is the most widely performed procedure for most types of glaucoma, including primary open-angle glaucoma (broad sense)6). To suppress scarring at the filtration site, antimetabolites such as mitomycin C (MMC) or 5-fluorouracil (5-FU) are used during and after surgery6).
In full-thickness filtration surgery, where the sclera is excised in full thickness without creating a scleral flap, complications due to early postoperative hypotony were significant. To solve this problem, trabeculectomy with a scleral flap became widespread. The filtration volume can be adjusted by the number and tension of scleral flap sutures, greatly reducing hypotony complications.
For early to moderate glaucoma with a target intraocular pressure (IOP) around 15 mmHg, outflow reconstruction surgery may be sufficient. However, in advanced cases, a target IOP around 10 mmHg is necessary, making filtration surgery indicated. The European Glaucoma Society Guidelines 6th Edition also states that trabeculectomy is the most effective procedure for advanced open-angle glaucoma and can be offered as a first surgery (evidence level: high, recommendation strength: strong) 8).
The CIGTS (Collaborative Initial Glaucoma Treatment Study) showed that initial trabeculectomy had a greater IOP-lowering effect compared to initial medication and suppressed visual field progression in patients with advanced visual field damage 7).
QWhich patients are indicated for trabeculectomy?
A
It is indicated when IOP control is insufficient with medication or laser treatment7). Cases requiring a target IOP around 10 mmHg for advanced glaucoma, and cases with poor medication adherence are also indications. Even in normal-tension glaucoma, achieving single-digit IOP with filtration surgery is effective in suppressing visual field progression 6). If life expectancy is limited or there is extensive scarring of the superior conjunctiva, tube shunt surgery or cyclodestructive procedures should be considered.
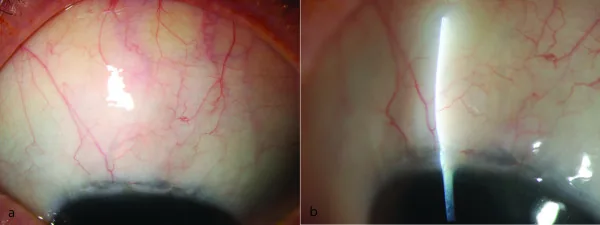
Furrer S, et al. Evaluation of filtering blebs using the ‘Wuerzburg bleb classification score’ compared to clinical findings. BMC Ophthalmol. 2012. Figure 1. PMCID: PMC3439283. License: CC BY.
A raised filtering bleb formed in the superior conjunctiva is shown in the external eye image and slit-lamp photograph. This image allows visual understanding of typical postoperative findings after trabeculectomy.
Trabeculectomy is indicated for cases with progressive disease despite maximum tolerated medical therapy 7). The types of glaucoma for which it is indicated are broad and include the following:
Primary open-angle glaucoma (POAG): In cases with advanced visual field damage, MMC-augmented trabeculectomy is ultimately required with a target IOP in the low teen to subteen range.
Neovascular glaucoma: MMC-augmented trabeculectomy is the first choice. Preoperative (1-7 days before) intravitreal injection of anti-VEGF agents (IVB) suppresses intraoperative and postoperative intraocular bleeding.
Glaucoma secondary to uveitis: MMC-augmented trabeculectomy or tube shunt surgery is performed 6).
Developmental glaucoma: Trabeculectomy with MMC is performed, but attention should be paid to risks in young patients.
Normal-tension glaucoma: Achieving single-digit intraocular pressure is effective for visual field preservation. In 92% of cases with postoperative IOP below 10 mmHg, MD slope improved6).
Cases where surgery is less effective (risk factors)
In cases with a history of intraocular surgery with significant conjunctival scarring, bleb formation is poor and surgical outcomes are unfavorable. Repeat trabeculectomy also yields inferior results.
Tube shunt surgery (with plate) is indicated for cases where trabeculectomy with MMC has failed, cases with severe conjunctival scarring, and cases where trabeculectomy is unlikely to succeed6).
Comparing trabeculectomy alone versus combined with cataract surgery, the intraocular pressure-lowering effect is superior with trabeculectomy alone 6). The risk of complications with combined surgery is equivalent to that of trabeculectomy alone, and visual improvement is naturally higher in the combined surgery group 6). Since bleb-forming surgery has a higher success rate when performed alone, it is recommended to perform cataract surgery first if the clinical situation permits 8).
For preoperative eye drops, use pilocarpine hydrochloride ophthalmic solution to induce miosis. In the case of combined cataract surgery, instill mydriatic eye drops, and after completion of lens reconstruction, inject Ovisot® (acetylcholine chloride) into the anterior chamber to induce miosis 6).
Suture the scleral flap at several points with 10-0 nylon.
Inject intraocular irrigating solution through the paracentesis site to restore intraocular pressure and confirm aqueous humor filtration from the scleral flap.
Suture the conjunctiva to form a bleb.
If postoperative intraocular pressure remains high, cut the 10-0 nylon sutures transconjunctivally with an argon laser to increase filtration and adjust intraocular pressure.
Conjunctival incision methods include limbal-based and fornix-based conjunctival incisions.
Fornix-based: Good intraoperative maneuverability, and diffuse well-formed filtering blebs are easily obtained. However, the rate of early postoperative bleb leakage is high.
Limbal-based: Wound closure is reliable, but avascular blebs with poor vascularity tend to occur in the late phase, posing risks of aqueous leakage and bleb infection.
QThe application time for MMC 0.04% has a range; what is the standard duration in minutes?
A
The concentration of MMC ranges from 0.02% to 0.04%, and the application time ranges from 2 to 5 minutes. Standardly, 0.04% is applied for 4 minutes and then thoroughly washed with physiological saline. Since excessive administration can cause corneal epithelial damage, conjunctival wound dehiscence, and scleral softening, it is important to adhere to appropriate concentration and application time.
Scarring and wound healing around the scleral flap can lead to filtration failure, and antimetabolites such as MMC and 5-FU are used to maintain intraocular pressure-lowering effects 6).
Pharmacology: Pyrimidine analog. Inhibits DNA synthesis and suppresses fibroblast proliferation.
Administration: 5 mg/day subconjunctival injection daily for 1 week (off-label). Use a 30G needle, inject on the opposite side of the bleb (90–180 degrees), and irrigate the eye immediately after injection8).
Advantages: Inexpensive and has a wide safety margin.
Disadvantages: Less effective than MMC. Higher incidence of corneal epithelial toxicity. Requires multiple injections7).
MMC was also used as eye drops after pterygium surgery, but it was discontinued in the 1980s because it could cause scleral calcification or necrotizing scleritis (scleromalacia perforans) months to years after surgery. 5-FU also had issues with ocular surface toxicity and bleb-related endophthalmitis, so currently, a single intraoperative application of low-concentration (0.02–0.04%) MMC for a short time is the mainstream approach.
There are no reports on whether additional postoperative subconjunctival injections of 5-FU improve surgical outcomes in cases where intraoperative MMC application was used. On the other hand, it is clear that it increases the frequency of corneal epithelial toxicity and aqueous humor leakage6).
QWhich should be used: mitomycin C or 5-FU?
A
Currently, intraoperative application of MMC is the mainstream approach8). MMC is more potent than 5-FU and can achieve lower intraocular pressure, but it carries a higher risk of hypotony-related complications7). 5-FU is inexpensive and has a wide safety margin, but it is less effective than MMC and requires multiple injections. 5-FU is mainly used for postoperative bleb management (e.g., with needling). For cases with high scarring risk (e.g., young age, history of inflammation), MMC use is standard.
Postoperative management is as important as surgical technique in determining surgical outcomes6). Whether the target intraocular pressure can be achieved depends on the adjustment of filtration through the scleral flap in the early postoperative period and the long-term suppression of subconjunctival scarring.
Corticosteroid eye drops: Recommended to suppress excessive scarring after surgery and to form a functional filtering bleb (Glaucoma Practice Guidelines 5th Edition CQ-5: Strong recommendation, evidence B)6)
Antibiotic eye drops: Continuous use for 1 to 3 months after surgery is strongly recommended (CQ-6)6). For long-term use, consider applying a new quinolone antibiotic eye ointment at bedtime if there is aqueous humor leakage from an avascular bleb.
This method involves suturing the scleral flap with multiple nylon sutures at the end of surgery to minimize filtration, and then gradually increasing filtration by cutting the sutures transconjunctivally with a laser according to postoperative intraocular pressure6).
Compress the conjunctiva with a special lens, visualize the sutures, and irradiate them.
The earlier LSL is performed postoperatively, the greater the intraocular pressure reduction, but the risk of overfiltration also increases13).
In trabeculectomy with MMC, the effect of suture lysis diminishes 3 weeks to 1 month after surgery, so appropriate follow-up intervals are necessary to avoid missing the timing13).
Methods include pressing the eyeball with a finger over the eyelid, or pressing near the scleral flap with a glass rod6). Scleral massage during examination is also useful to check outflow from the scleral flap and to determine the need for LSL.
More common with fornix-based conjunctival incision12)
Hyphema is frequently observed because peripheral iridectomy is performed. Aqueous leakage from the conjunctival incision is more common with fornix-based conjunctival incisions.
After trabeculectomy with MMC, a large drop in intraocular pressure can lead to hypotony maculopathy. It is more common in young myopic patients6). Persistent hypotony shortens axial length, causing choroidal folds, macular folds, tortuous retinal vessels, and optic disc edema, resulting in severe visual impairment.
Treatment options include the following:
Transconjunctival scleral flap resuturing: A method of suturing the scleral flap with nylon thread from above the conjunctiva, shown to be effective long-term6)
Autologous blood injection: A method of injecting autologous blood into the bleb near the bleb using a 27G needle, effective for improving hypotony but may cause a sudden rise in intraocular pressure6)
Surgical resuturing: If the above does not improve, open the conjunctiva and resuture the scleral flap under direct visualization.
Long-term postoperative complications include aqueous humor leakage due to thinning of the bleb wall and bleb infection caused by bacterial invasion into the bleb. If bacteria invade the vitreous, bacterial endophthalmitis may occur.
Late infection: The incidence after trabeculectomy with MMC in Japanese patients was 2.2% at 5 years (CBIITS 2 study)9)
Risk factors: Aqueous leakage is a risk factor for bleb infection. Avascular blebs are more likely to occur with limbus-based conjunctival incisions.
Management: If bleb infection is suspected, immediately administer subconjunctival, intracameral, or intravitreal antibiotics, or perform vitrectomy, depending on the stage.
If the scleral flap adheres early and aqueous humor does not filter into the subconjunctival space, needling is required. A 25- to 27-gauge needle or microsurgical knife is inserted through the conjunctiva to lift the scleral flap and break the adhesions6).
Needling with antimetabolites: Efficacy has been reported when the bleb shrinks over time and intraocular pressure rises again6)
Encapsulated bleb: Presents as a high, dome-shaped bleb with a thick wall and dilated vascular invasion. It occurs in about 13% of cases after trabeculectomy and causes elevated intraocular pressure6)
Postoperative bleb evaluation uses the Moorfields or Indiana classification. Morphologically, blebs are classified as cystic, diffuse, or flat. The Seidel test checks for leakage, and signs of infection are assessed. Anterior segment OCT can noninvasively evaluate the internal structure of the bleb (position of the scleral flap, presence of fluid cavities, degree of encapsulation).
QWhat should be done if intraocular pressure rises after surgery?
A
If the anterior chamber is deep, obstruction of the fistula or insufficient outflow from the scleral flap is suspected. Laser suture lysis (LSL) to increase filtration is the first choice 6). If LSL is insufficient, needling with an antimetabolite should be considered. Argon laser is used for iris obstruction of the fistula. If the anterior chamber is shallow, differentiate between suprachoroidal hemorrhage, pupillary block, and malignant glaucoma.
Trabeculectomy is a surgery that creates a small hole at the corneoscleral limbus, forming a new aqueous humor outflow pathway between the anterior chamber and the subconjunctival tissue 6). It bypasses the outflow resistance of the trabecular meshwork and establishes a direct drainage route into the subconjunctival space.
Aqueous humor reaching the filtering bleb is processed through the following pathways:
Filtration into the tear film via the conjunctiva
Absorption by conjunctival vessels and perivascular tissue
Full-thickness filtration surgery creates a direct aqueous outflow pathway from the anterior chamber to the subconjunctival space without creating a scleral flap, but controlling the filtration volume is difficult and complications such as shallow anterior chamber are common 6). In trabeculectomy, a scleral flap is created, and the filtration volume can be adjusted by the number and tension of sutures, allowing gradual increase of filtration postoperatively with LSL.
MMC acts as a DNA crosslinking agent, non-selectively inhibiting fibroblast proliferation 8). 5-FU inhibits DNA synthesis as a pyrimidine analog. Both suppress scarring at the filtration site and contribute to long-term maintenance of the filtering bleb.
When performing MMC-augmented trabeculectomy in young patients, the MMC reaction tends to be strong, and avascular, thin-walled, localized blebs are likely to form. If the wall becomes partially very thin and leakage is observed, the risk of visual impairment due to hypotony and late-onset infection increases, so long-term postoperative follow-up requires special attention.
Fang et al. retrospectively examined visual field changes in 206 eyes that underwent MMC-augmented trabeculectomy1). Mean intraocular pressure decreased by 50.2% from 22.7 mmHg to 10.4 mmHg, and 84.5% were medication-free at 24 months postoperatively. Regarding visual fields, 17% improved, 37.4% remained stable, and 45.6% worsened. Cases with preoperative MD values up to -12 dB showed high rates of visual field improvement/stability, while advanced cases exceeding -24 dB had higher rates of worsening1).
These results suggest the importance of early surgical intervention when visual field damage is at a stage with MD less than -12 dB1).
In the 5-year results of the TVT study (Tube Versus Trabeculectomy Study), there was no significant difference in intraocular pressure control between trabeculectomy and Baerveldt glaucoma implant surgery10). However, the cumulative failure rate was significantly higher in the trabeculectomy group (46.9%) than in the tube shunt group (29.8%)10).
The types of complications differed between the two groups.
More common with trabeculectomy: bleb leakage, hypotony maculopathy, bleb infection
More common with tube shunt surgery: corneal endothelial damage, tube exposure
Tube shunt surgery (with plate) is recommended for cases where trabeculectomy is ineffective or expected to be ineffective6).
Sugimoto et al. reported long-term outcomes of MMC-augmented trabeculectomy for primary open-angle glaucoma in Japanese patients, examining the probability of maintaining intraocular pressure below 16 mmHg with the use of eye drops11). The mean postoperative intraocular pressure in successful cases was around 10 mmHg, and appropriate postoperative management was a key factor influencing outcomes.
Summary: A 10-year-old child with Sturge-Weber syndrome. After normalization of intraocular pressure by trabeculectomy, serous retinal detachment completely resolved within 2 months.
Spontaneous Bleb Reformation after Phacoemulsification
Report: Chanbour et al. (2021) 4)
Summary: A 79-year-old woman with a failing bleb. High intraocular pressure during cataract surgery reopened the scleral flap, leading to spontaneous bleb reformation.
Other case reports: Kandarakis et al. reported a case of bleb failure within 3 days after herpes zoster ophthalmicus occurring 13 months after trabeculectomy 2). Gur Gungor et al. reported a 31-year-old woman who developed hypotony maculopathy due to scleral flap dehiscence from Valsalva maneuver 5.5 years after MMC-augmented trabeculectomy, which was repaired with pericardial patch graft 5).
In a retrospective study of 206 eyes by Fang et al., visual field improvement and stability rates were higher in eyes with mild to moderate damage (preoperative MD up to -12 dB) 1). In the CIGTS, the initial trabeculectomy group suppressed visual field progression 7). Even in normal-tension glaucoma progressing at low intraocular pressure, achieving single-digit IOP with filtration surgery is effective for visual field preservation 6). Early surgical intervention with appropriate patient selection is considered to contribute to visual field preservation.
Fang CEH, Hakim MT, Siddiqui MM, Armstrong D, Shankar V. A retrospective study to assess visual field improvement following augmented trabeculectomy. Indian J Ophthalmol. 2023;71(5):1953-1959. doi:10.4103/ijo.IJO_2071_22.
Kandarakis SA, Karampelas M, Soumplis V, et al. Acute trabeculectomy failure following herpes zoster ophthalmicus. Ther Adv Ophthalmol. 2021;13:25158414211022461.
Barbosa RS, Salgado CM, Salgado RS, et al. Serous retinal detachment resolution after trabeculectomy in Sturge-Weber syndrome. J Glaucoma. 2021;30:e325-e328.
Chanbour W, Chanbour H, Tomey KF, Khoueir Z. Spontaneous Trabeculectomy Bleb Reformation and Regain of Function Following Phacoemulsification. Cureus. 2021;13(8):e16979. doi:10.7759/cureus.16979.
Gur Gungor S, Ceylan OM, Gul A, et al. Scleral flap wound dehiscence with Valsalva maneuver years after trabeculectomy with mitomycin C. Case Rep Ophthalmol Med. 2022;2022:8534641.
Gedde SJ, Vinod K, Wright MM, et al. Primary Open-Angle Glaucoma Preferred Practice Pattern. Ophthalmology. 2021 Jan;128(1):P71-P150. doi:10.1016/j.ophtha.2020.10.022. PMID:34933745.
Pazos M, Traverso CE, Viswanathan A; European Glaucoma Society. European Glaucoma Society - Terminology and guidelines for glaucoma, 6th Edition. Br J Ophthalmol. 2025;109(Suppl 1):1-212. doi:10.1136/bjophthalmol-2025-egsguidelines. PMID:41026937.
Yamamoto T, Sawada A, Mayama C, Araie M, Ohkubo S, Sugiyama K, et al. The 5-year incidence of bleb-related infection and its risk factors after filtering surgeries with adjunctive mitomycin C: collaborative bleb-related infection incidence and treatment study 2. Ophthalmology. 2014;121(5):1001-6. doi:10.1016/j.ophtha.2013.11.025. PMID:24424248.
Gedde SJ, Herndon LW, Brandt JD, Budenz DL, Feuer WJ, Schiffman JC, et al. Postoperative complications in the Tube Versus Trabeculectomy (TVT) study during five years of follow-up. American journal of ophthalmology. 2012;153(5):804-814.e1. doi:10.1016/j.ajo.2011.10.024. PMID:22244522; PMCID:PMC3653167.
Sugimoto Y, Mochizuki H, Ohkubo S, et al. Intraocular pressure outcomes and risk factors for failure in the collaborative bleb-related infection incidence and treatment study. Ophthalmology. 2015;122:2223-2233.
Kirwan JF, Lockwood AJ, Shah P, Macleod A, Broadway DC, King AJ, et al. Trabeculectomy in the 21st century: a multicenter analysis. Ophthalmology. 2013;120(12):2532-2539. doi:10.1016/j.ophtha.2013.07.049. PMID:24070811.
Morinelli EN, Sidoti PA, Heuer DK, Minckler DS, Baerveldt G, LaBree L, et al. Laser suture lysis after mitomycin C trabeculectomy. Ophthalmology. 1996;103(2):306-14. doi:10.1016/s0161-6420(96)30699-4. PMID:8594519.
Copy the article text and paste it into your preferred AI assistant.
Article copied to clipboard
Open an AI assistant below and paste the copied text into the chat box.