Exfoliation glaucoma (pseudoexfoliative glaucoma: PXG) is a secondary open-angle glaucoma associated with exfoliation syndrome (pseudoexfoliation syndrome: PXF/PEX). Abnormal fibrillar granular protein, exfoliation material, progressively deposits in various tissues of the anterior segment, increasing outflow resistance in the trabecular meshwork and elevating intraocular pressure. It is the most common form of secondary open-angle glaucoma2)3).
Exfoliation material deposits not only in intraocular tissues (pupil margin, anterior lens capsule, Zinn zonules, angle, ciliary body, corneal endothelium) but also in systemic tissues such as skin, heart, lung, and liver, making it a systemic disease.
PXF is common in the elderly, found in about 4% of people aged 70 years or older. The Hisayama study reported a prevalence of exfoliation syndrome of 3.4% in those aged 50 years or older. 15–26% of PXF patients develop PXG within 5 years, and eventually about 50% are diagnosed with glaucoma2)3). The progression rate of PXG is about three times that of POAG, and it is not uncommon to find advanced visual field defects at the time of diagnosis3).
PXF/PXG has been reported to be associated with systemic diseases. Associations with coronary artery disease, cerebrovascular disease, arteriosclerosis, abdominal aortic aneurysm, sensorineural hearing loss, inguinal hernia, and pelvic organ prolapse in women have been noted2)3).
QWhat is the difference between exfoliation syndrome and exfoliation glaucoma?
A
Exfoliation syndrome (PXF) is a systemic disease in which exfoliation material deposits in the anterior segment of the eye and throughout the body. Exfoliation glaucoma (PXG) refers to a condition in which elevated intraocular pressure and glaucomatous optic neuropathy develop in association with PXF2)3). Not all patients with PXF develop PXG; ultimately, about 50% are diagnosed with glaucoma. Even in the stage of PXF alone, follow-up with intraocular pressure measurement at least once a year is recommended1).
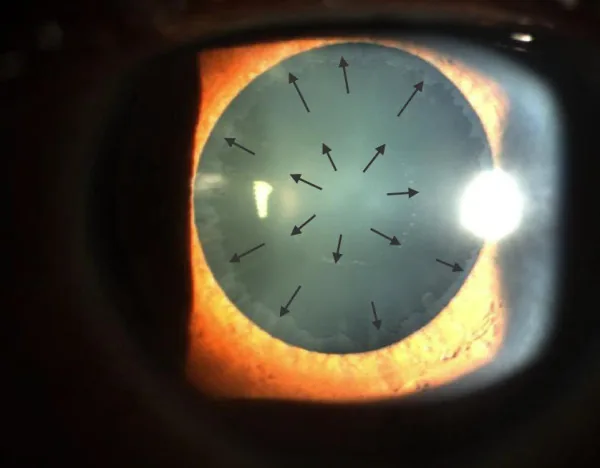
Elhawy E, et al. Pseudoexfoliation syndrome, a systemic disorder with ocular manifestations. Hum Genomics. 2012. Figure 1. PMCID: PMC3500235. License: CC BY.
In a dilated anterior segment photograph, gray-white exfoliation material is deposited on the anterior lens capsule, showing a characteristic double ring pattern consisting of a central disc and a peripheral band. This is a representative image of clinical findings in exfoliation glaucoma.
The subjective symptoms of PXG are similar to those of primary open-angle glaucoma, and are often asymptomatic in the early stages. Because it is unilateral and progresses slowly, it is often unnoticed and may be discovered with advanced visual field defects. During acute intraocular pressure elevation, eye pain, blurred vision, and colored halos may occur. If the lens moves forward, myopia may develop. Due to large diurnal fluctuations in intraocular pressure, a single measurement during an office visit may miss high intraocular pressure3).
Exfoliation material: White fibrous material deposits on the pupillary margin and anterior lens capsule. On the anterior lens capsule, a three-layer structure (bull’s eye pattern) is seen: central disc (central clear zone), intermediate zone (intermediate zone without exfoliation material), and peripheral band. The peripheral band is present in all cases and may only be visible after pupil dilation.
Poor dilation: Atrophy of the iris pigment epithelium leads to a moth-eaten appearance of the pupillary margin, known as “moth-eaten pupil” 2)3)
Lens phacodonesis and subluxation: Progressive damage to the zonules of Zinn may cause lens phacodonesis or subluxation. If there is a difference in anterior chamber depth between the two eyes, zonular weakness on the shallower side should be suspected 3)
Findings in pseudophakic eyes: After cataract surgery, exfoliation material may deposit on the IOL surface or pupillary margin. The deposition pattern differs from that in phakic eyes, concentrating in the mid-periphery 8)
Angle and Optic Nerve Findings
Sampaolesi line: Wavy pigmentation anterior to the Schwalbe line, a characteristic finding of exfoliation glaucoma 2)3)
Trabecular meshwork pigmentation: Shows heavy and uneven pigmentation, described as a “salt and pepper” appearance. The pigment is not evenly distributed around the entire circumference of the trabecular meshwork3)
Secondary angle closure: Due to anterior lens displacement from zonular weakness, secondary angle narrowing or closure may occur in 9–18% of cases.
Optic disc: Presents glaucomatous optic neuropathy. Cupping enlargement and rim thinning progress rapidly, and often advanced visual field and optic nerve damage are already present at diagnosis2)3)
Without pupil dilation, exfoliation material may be missed in about 20% of cases. Even if found unilaterally, increased trabecular pigmentation in the fellow eye can be the earliest sign, so detailed observation of both eyes is essential.
The cause of PXG is the production and deposition of abnormal fibrillogranular protein (exfoliation material) in exfoliation syndrome2)3).
LOXL1 gene: Polymorphisms in the lysyl oxidase-like 1 (LOXL1) gene, involved in elastic fiber biosynthesis, are most strongly associated with genetic predisposition to PXF2)3). Representative single nucleotide polymorphisms are rs3825942 (G153D) and rs1048661 (R141L). In Japan, about half of the population carries high-risk polymorphisms.
Aging: Onset occurs after age 50, with frequency increasing rapidly after age 702)3).
Ethnicity: Prevalence is high in Scandinavian and Mediterranean populations, and it is also observed at a certain frequency in East Asians.
Environmental factors: Ultraviolet exposure and oxidative stress are thought to promote production. Even with high-risk LOXL1 alleles, the majority do not develop PXF, suggesting involvement of environmental factors2)3).
Systemic comorbidities: Associations with coronary artery disease, myocardial infarction, cerebrovascular disease, arteriosclerosis, abdominal aortic aneurysm, sensorineural hearing loss, and inguinal hernia have been reported2)3).
Risk alleles are not consistent across populations; an allele considered high-risk in one population may be protective in another. Even within the same population, the majority of individuals with high-risk polymorphisms do not develop PXF.
The diagnosis of PXG is mainly based on clinical findings with slit-lamp microscopy.
Slit-lamp microscopy: Confirm exfoliation material on the pupillary margin and anterior lens capsule. Exfoliation material on the pupillary margin is easier to see with miosis, and exfoliation material on the anterior lens surface is observed with dilation. The peripheral band may only be seen after dilation, so dilated examination is essential.
Gonioscopy: Confirm Sampaolesi line and heavy trabecular pigmentation 2)3). Uneven pigment distribution is useful for differentiating from pigmentary glaucoma.
Visual field testing: Evaluation of visual field defects using Humphrey static perimetry (30-2 and 10-2 programs).
OCT: Assess thinning of the retinal nerve fiber layer (RNFL) and ganglion cell layer (GCC).
OCTA: Decreased peripapillary and macular vessel density (VD) has been reported 4).
Differential diagnoses include primary open-angle glaucoma, primary angle-closure glaucoma, pigment dispersion syndrome, pigmentary glaucoma, true exfoliation (capsular delamination), and amyloidosis. Overlooking exfoliation material may lead to misdiagnosis as primary open-angle glaucoma; therefore, detailed examination under mydriasis is essential.
Feature
Exfoliation glaucoma (PXG)
Pigmentary glaucoma
Age group
More common in elderly
More common in young myopic males
Pigment distribution
Uneven (salt and pepper)
Uniform heavy pigmentation
Characteristic findings
Sampaolesi line, exfoliation material at pupillary margin
Krukenberg spindle, iris transillumination
Pathogenesis
Deposition of exfoliation material in trabecular meshwork
Pigment release from posterior iris
QWhat are the key points for differentiating from primary open-angle glaucoma?
A
The most important point is the identification of exfoliation material. Perform a dilated examination and carefully observe the pupillary margin and the anterior lens capsule (especially the peripheral band). In the angle, Sampaolesi line and uneven pigmentation are characteristic of PXG2)3). PXG tends to have higher intraocular pressure levels and greater diurnal fluctuations than primary open-angle glaucoma3). Differentiation from primary open-angle glaucoma is important because it directly affects treatment strategy (need for aggressive intraocular pressure reduction, timing of surgery)1).
The basic treatment policy follows that for primary open-angle glaucoma, aiming to lower intraocular pressure1)2). However, because PXG has large intraocular pressure fluctuations and glaucomatous optic neuropathy progresses faster than POAG, aggressive intraocular pressure reduction is recommended (recommendation grade 1B)1). The target intraocular pressure is individualized based on disease stage, untreated intraocular pressure, and other risk factors, and reassessed repeatedly.
First-line treatment is prostaglandin (PG) analog eye drops1). If the target intraocular pressure is not achieved with monotherapy, the following are used in combination.
Prostaglandin analogs: latanoprost, travoprost, tafluprost, etc. Promote uveoscleral outflow of aqueous humor
Beta-blockers: timolol, etc. Suppress aqueous humor production (contraindicated in bronchial asthma and atrioventricular block)
Because of the heavy pigmentation in the angle, laser trabeculoplasty (ALT/selective laser trabeculoplasty: SLT) is relatively effective1)2). The 5th edition of the Glaucoma Clinical Practice Guidelines reports that outflow reconstruction surgery and laser trabeculoplasty achieve greater intraocular pressure reduction in PXG than in POAG (recommendation grade 1B)1).
However, long-term efficacy is limited, and many cases show reduced effect after several years. It is basically positioned as a bridging therapy until surgery or as an emergency measure when surgery is difficult due to systemic conditions or social circumstances. In the 6-year results of the LiGHT trial, initial SLT strategy showed visual prognosis equal to or better than eye drop strategy in POAG and ocular hypertension, and SLT is being reevaluated as an initial treatment strategy11).
Since many cases already have high intraocular pressure and advanced visual field damage at the time of diagnosis, sufficient intraocular pressure reduction is often required, and early surgery is considered if visual field damage is progressing1).
Glaucoma surgery
Trabeculectomy: It is the first choice in cases with extremely high intraocular pressure or advanced visual field damage1). Mitomycin C combination is standard.
Trabeculotomy: Effective, but may not achieve sufficient intraocular pressure reduction in cases with very high preoperative intraocular pressure, and some cases experience intraocular pressure re-elevation several years after surgery.
Outflow reconstruction surgery/MIGS: Greater intraocular pressure reduction has been reported in PXG compared to POAG1). Introduction of MIGS during combined cataract surgery also contributes to reducing the number of eye drops.
Wipe-out syndrome: Irreversible central vision loss has been reported after filtration surgery for advanced PXG5). It is thought to be caused by postoperative hypotony and ciliary body dysfunction.
Cautions for cataract surgery
Management of poor mydriasis: Consider preparation of iris retractors or a Malyugin ring 6)10)
Management of zonular weakness: Insertion of a capsular tension ring (CTR) is recommended. Create a continuous curvilinear capsulorhexis (CCC) of at least 6 mm to prevent anterior capsule contraction. Use gentle ultrasound maneuvers and nuclear division techniques to reduce stress on the zonules 6)10)
Late postoperative IOL dislocation: PXF is the most common cause of late IOL dislocation, with an approximately 6-fold increased risk reported 9). Long-term postoperative follow-up is essential
UGH syndrome: Even with in-the-bag IOL, instability of the IOL-capsule complex due to zonular weakness can chafe the iris, causing recurrent hyphema and elevated intraocular pressure7)
QWhat are the points to note in cataract surgery?
A
Cataract surgery in PXF patients presents three major problems. First, poor mydriasis: prepare iris retractors or a Malyugin ring 6)10). Second, zonular weakness: gentle maneuvers and use of a CTR are recommended. Create a continuous curvilinear capsulorhexis of at least 6 mm to prevent anterior capsule contraction 10). Third, risk of late IOL dislocation: long-term follow-up is necessary 6)9). The risk of vitreous loss is 5 to 10 times higher than usual. In elderly patients on multiple eye drops, combining MIGS with cataract surgery may be an option to reduce the number of drops 1).
Exfoliation material is an abnormal fibrillogranular protein with a structure consisting of a protein core surrounded by a glycoprotein complex 2)3). It is produced by multiple cells in the anterior segment, including non-pigmented ciliary epithelial cells, trabecular endothelial cells, and equatorial anterior lens epithelial cells. Oxidative stress is thought to promote its production.
The produced exfoliation material is released into the extracellular space and progressively deposits on the zonules, pupillary margin, anterior lens capsule, trabecular meshwork, and corneal endothelium. It is also present in systemic tissues such as skin, heart, lung, and liver, not only in ocular tissues 2)3).
Deposition of exfoliation material in the trabecular meshwork increases resistance to aqueous humor outflow, which is the main cause of intraocular pressure elevation. Additionally, the following mechanisms are involved.
Production of exfoliation material by trabecular meshwork cells themselves
Phagocytosis of pigment granules by trabecular meshwork cells
Abnormal deposition of extracellular matrix due to inhibition of elastic fiber formation
Excessive pigment release due to atrophy of the iris pigment epithelium and consequent pigment loading of the trabecular meshwork
OCTA studies have shown that in PXG eyes, the peripapillary and macular vessel density is significantly reduced compared to control eyes 4). It is thought that exfoliation material accumulates in endothelial cells, smooth muscle cells, and pericytes of small blood vessels, leading to microcirculatory dysregulation and vascular occlusion 4).
The fact that PXG progresses faster than POAG even when intraocular pressure is controlled suggests the existence of intraocular pressure-independent pathological mechanisms 4). The lamina cribrosa has been reported to be thinner and less rigid in PXG eyes compared to POAG eyes 4).
Deposition of exfoliation material on the zonules of Zinn causes progressive weakening. This leads to lens instability, anterior movement, myopia, and secondary angle closure. It also contributes to increased complications during cataract surgery and late postoperative IOL-capsular bag dislocation 6)9).
A systematic review by Chatziralli et al. consistently reported that peripapillary and macular VD is significantly reduced in PXG eyes compared to control eyes 4). Comparisons between PXG and POAG have yielded mixed results, with some reports showing lower VD in PXG and others showing no difference 4). Peripapillary VD is particularly impaired in the inferonasal and nasal regions, suggesting that the nasal part of the lamina cribrosa is vulnerable to glaucomatous damage 4).
Exfoliation material deposition in pseudophakic eyes
Park et al. reported rare cases of exfoliation material deposition on the IOL surface in pseudophakic eyes 8). It appears 2 to 20 years after cataract surgery, and the deposition pattern differs from phakic eyes, concentrating in the mid-periphery. Since exfoliation material on the IOL may be a sign of progression from PXF to PXG, regular dilated slit-lamp examination is recommended 8).
Nakagawa et al. reported a two-stage IOLintrascleral fixation technique that preserves the lens capsule in aphakic eyes where IOL insertion was difficult due to zonular weakness caused by PXF 6). Capsule preservation is expected to prevent intraoperative vitreous prolapse, suppress iris instability, and prevent IOLpupillary capture6).
Erdinest et al. reported IOLscleral fixation using the triangular suture technique (TST) 9). This technique creates an artificial ciliary sulcus with a triangular prolene suture to support the IOL, and stability has been confirmed for up to 4 years 9). Since the risk of IOL dislocation is approximately 6 times higher in PXF patients, these new techniques are clinically important 9).
Park et al. reported UGH syndrome occurring with in-the-bag IOL in a PXG patient 7). Asymptomatic IOL-bag complex oscillation due to zonular instability abraded the posterior iris surface, causing recurrent hyphema and intralenticular hemorrhage 7). Hemorrhage tends to be prolonged in patients on anticoagulant therapy 7).
Reevaluation of Initial SLT Strategy (LiGHT Trial)
The 6-year follow-up of the LiGHT trial showed that initial SLT strategy in POAG and ocular hypertension provided visual function QOL and visual field preservation equivalent or superior to the eye drop strategy, with a significantly lower conversion rate to invasive surgery 11). Although PXG was not the main target of the LiGHT trial, it is known that SLT responsiveness is good in PXG with strong angle pigmentation, so there is room to actively consider SLT as an early treatment option 1)11). However, long-term attenuation of SLT effect in PXG remains a challenge, and continuous IOP and visual field evaluation is essential.
QHow do you manage the risk of IOL dislocation?
A
In PXF patients, the risk of IOL dislocation is approximately 6 times higher 9). For prevention, the use of CTR, continuous curvilinear capsulorhexis of 6 mm or more, and atraumatic surgical technique are important 6)10). If dislocation occurs, IOLintrascleral fixation is an option. New techniques such as capsule preservation 6) and triangular suture method 9) have also been reported. Long-term follow-up after surgery is essential, and signs of IOL oscillation or displacement should be checked with a slit lamp.
European Glaucoma Society. European Glaucoma Society Terminology and Guidelines for Glaucoma, 5th Edition. Br J Ophthalmol. 2021 Jun;105(Suppl 1):1-169. doi:10.1136/bjophthalmol-2021-egsguidelines. PMID:34675001.
Pazos M, Traverso CE, Viswanathan A; European Glaucoma Society. European Glaucoma Society - Terminology and guidelines for glaucoma, 6th Edition. Br J Ophthalmol. 2025;109(Suppl 1):1-212. doi:10.1136/bjophthalmol-2025-egsguidelines. PMID:41026937.
Chatziralli I, Milionis I, Christodoulou A, Theodossiadis P, Kitsos G. The Role of Vessel Density as Measured by Optical Coherence Tomography Angiography in the Evaluation of Pseudoexfoliative Glaucoma: A Review of the Literature. Ophthalmology and therapy. 2022;11(2):533-545. doi:10.1007/s40123-022-00483-1. PMID:35211880; PMCID:PMC8927482.
Kaur J, Yogesvaran R, Mohd Khialdin S, Md Din N. Wipe-Out Syndrome After PreserFlo MicroShunt Implantation in a Patient With Pseudoexfoliation Glaucoma. Cureus. 2025;17(12):e99396.
Nakagawa S, Kanda S, Ishii K. Secondary Intrascleral Intraocular Lens Fixation With Lens Capsule Preservation for Aphakic Eyes in Patients With Pseudoexfoliation Syndrome: A Case Series. Cureus. 2024;16(10):e70688. doi:10.7759/cureus.70688. PMID:39372382; PMCID:PMC11452084.
Park JH, Ensor W, Olson J, Hale B. Intracapsular hemorrhage in the setting of pseudoexfoliation syndrome. Digital journal of ophthalmology : DJO. 2021;26(2):4-6. doi:10.5693/djo.02.2020.02.003. PMID:33867875; PMCID:PMC8031965.
Park IK, Kim KW, Chun YS. Pseudoexfoliation Syndrome Showing Different Deposition Patterns in Pseudophakic Eyes: Two Case Reports. Korean journal of ophthalmology : KJO. 2024;38(2):173-175. doi:10.3341/kjo.2023.0115. PMID:38351487; PMCID:PMC11016691.
Erdinest N, Eshel Y, Saban O, Averbukh E, Khateb S, Lavy I. The novel triangular suture technique for intraocular Lens fixation in patients with pseudoexfoliation syndrome suffering from dislocation: Case series. European journal of ophthalmology. 2025;35(4):NP1-NP6. doi:10.1177/11206721241310468. PMID:40080848; PMCID:PMC12181633.
Gazzard G, Konstantakopoulou E, Garway-Heath D, Adeleke M, Vickerstaff V, Ambler G, et al. Laser in Glaucoma and Ocular Hypertension (LiGHT) Trial: Six-Year Results of Primary Selective Laser Trabeculoplasty versus Eye Drops for the Treatment of Glaucoma and Ocular Hypertension. Ophthalmology. 2023;130(2):139-151. doi:10.1016/j.ophtha.2022.09.009. PMID:36122660.
Copy the article text and paste it into your preferred AI assistant.
Article copied to clipboard
Open an AI assistant below and paste the copied text into the chat box.