Pseudophakic glaucoma is glaucoma that occurs in eyes with an intraocular lens (IOL) after cataract surgery, while aphakic glaucoma occurs in aphakic eyes without an IOL. Both are classified as secondary glaucoma1)2)3). The 5th edition of the Glaucoma Clinical Practice Guidelines lists post-cataractglaucoma as an independent category, and it is a clinically important complication in both adults and children1).
Based on the mechanism of onset, it is broadly classified into open-angle and angle-closure mechanisms 6). Open-angle mechanisms include residual ophthalmic viscosurgical device (OVD), postoperative inflammation, lens particles, pigment dispersion, steroid-induced glaucoma, and ghost cell glaucoma. Angle-closure mechanisms include pupillary block, vitreous prolapse, peripheral anterior synechiae, and UGH syndrome. Inflammatory glaucoma after cataract surgery develops through multiple overlapping mechanisms, including trabecular meshwork obstruction by inflammatory cells and proteins, trabeculitis, and formation of peripheral anterior synechiae6).
Transient intraocular pressure elevation after surgery is observed in 29–50% of patients on the first postoperative day 4). However, most cases resolve spontaneously within a few days. The prevalence of chronic glaucoma after standard extracapsular cataract extraction is reported to be 2.1–4%. The prevalence of chronic glaucoma after surgery in aphakic eyes is approximately 3%. With the widespread use of phacoemulsification, the frequency of aphakia has markedly decreased, but it can still occur in cases of posterior capsule rupture or difficulty with intraocular lens insertion.
The mechanism of intraocular pressure fluctuation after cataract surgery varies depending on the time of onset.
Glaucoma after pediatric cataract surgery is an important complication, occurring in 18–26% of cases after congenital cataract surgery. The incidence reaches up to 50% when surgery is performed before 9 months of age 2). It may be associated with developmental abnormalities of the aqueous outflow pathway, and the risk persists throughout life 1). Young age at surgery, microcornea, and microphthalmos are risk factors.
In a large-scale dataset of over 7.5 million cases from the IRIS Registry, the incidence of persistent pseudophakic uveitis (PUPPI) after cataract surgery was reported as 1.68% 5). In diabetic patients, the risk of onset increases by 1.87 times 5).
QCan glaucoma still occur after modern cataract surgery?
A
Even with modern small-incision phacoemulsification, postoperative intraocular pressure elevation can occur. However, it is often transient, and the rate of progression to chronic glaucoma is low at 2–4%. Thorough removal of viscoelastic material, atraumatic tissue manipulation, and early postoperative intraocular pressure monitoring can minimize the risk. In patients with pre-existing glaucoma, early postoperative intraocular pressure elevation may worsen optic neuropathy, so careful management is necessary as described in the “Causes and Risk Factors” section4).
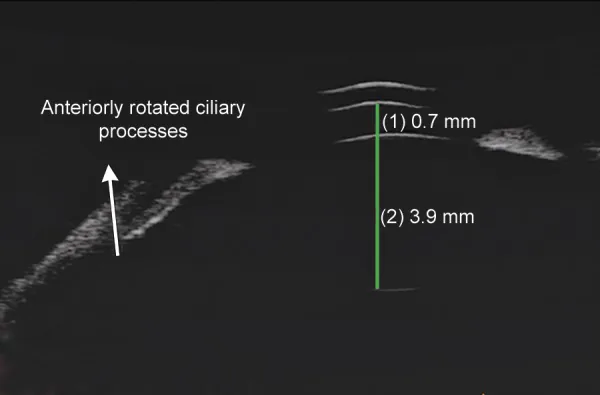
Parivadhini A, et al. Management of Secondary Angle Closure Glaucoma. J Curr Glaucoma Pract. 2014. Figure 1C. PMCID: PMC4741163. License: CC BY.
Anterior segment UBM shows marked shallowing of the anterior chamber and anterior rotation of the ciliary processes. This image demonstrates diagnostic findings of anterior chamber narrowing seen in glaucoma after cataract surgery with intraocular lens implantation or aphakia.
Early postoperative transient intraocular pressure elevation: May present with eye pain, blurred vision, and decreased visual acuity due to corneal edema. Symptoms appear within hours to days after surgery if caused by residual viscoelastic material or inflammation.
Chronic course: As with glaucoma in general, early stages are asymptomatic; as it progresses, patients become aware of visual field defects (scotomas). Often unnoticed until visual field impairment is advanced.
Acute pupillary block: Presents with severe eye pain, headache, and nausea, similar to acute glaucoma attack. Iris bombé and marked shallow anterior chamber are observed.
UGH syndrome: Characterized by transient visual loss due to recurrent anterior chamber hemorrhage. Repeated blurred vision and hyperemia occur.
Residual ophthalmic viscosurgical device (OVD): Residual OVD is observed in the anterior chamber in the early postoperative period. Dispersive OVDs tend to enter the trabecular meshwork more easily than cohesive types, making removal more difficult and more likely to cause intraocular pressure elevation.
Postoperative inflammation: Increased inflammatory cells and flare in the anterior chamber. Excessive inflammation can cause trabecular meshwork obstruction and fibrosis 2)3).
Steroid-induced glaucoma: Intraocular pressure elevation during postoperative steroid eye drop use. Potency order: dexamethasone ≥ betamethasone > fluorometholone. It is dose-dependent and more pronounced in younger individuals.
Lens particles: White particles floating in the anterior chamber. After extracapsular cataract extraction or YAG laser posterior capsulotomy, residual cortex or nuclear fragments can obstruct the trabecular meshwork.
Pigment dispersion: Iris transillumination defects and trabecular meshwork pigmentation. This is particularly problematic with one-piece IOLs placed in the ciliary sulcus.
Findings of Angle-Closure Mechanism
Pupillary block: Iris bombé and shallow anterior chamber. Can occur with anterior chamber IOLs or ciliary sulcus IOLs 2).
UGH syndrome: Triad of uveitis, glaucoma, and hyphema. The IOL haptic directly contacts and chafes the iris or surrounding tissues, causing inflammation. Released iris pigment can clog the trabecular meshwork, leading to pigmentary glaucoma2)3).
Iris chafing syndrome: Main findings are iris atrophy and recurrent hyphema. It occurs when the haptic or optic edge of a posterior chamber IOL inserted in the sulcus continuously chafes the iris or angle vessels. Bleeding is more common in patients using anticoagulants.
Vitreous prolapse: Acute angle closure due to vitreous in the anterior chamber.
Peripheral anterior synechiae: Chronic angle closure due to postoperative inflammation and shallow anterior chamber.
The mechanisms causing intraocular pressure elevation after cataract surgery are diverse 2)3). The causes of IOP spikes are multifactorial, involving surgical trauma, retained lens material, retained OVD, preexisting outflow obstruction, release of iris pigment, hyphema, and inflammation 4).
The main risk factors include the following.
Pre-existing glaucoma: Postoperative intraocular pressure (IOP) elevation can worsen optic nerve damage. In cases with pseudoexfoliation syndrome (PEX), the risk of IOP elevation within 24 hours after surgery is particularly high4)9).
Improper IOL placement: Ciliary sulcus placement of a one-piece acrylic IOL carries a high risk of pigment dispersion and UGH syndrome. Extracapsular insertion of a single-piece IOL can cause UGH syndrome.
Postoperative steroid eye drops: IOP increases depending on the potency and dose of the steroid. Dexamethasone and betamethasone have a stronger IOP-elevating effect than fluorometholone. Triamcinolone can cause sustained IOP elevation for 9 to 12 months.
Pediatric cataract surgery: Surgery, especially in infants younger than 9 months, carries a significantly high risk of glaucoma2). Microcornea and microphthalmos are also independent risk factors.
Nd:YAG laser posterior capsulotomy: This can cause transient IOP elevation2)3). Lens particles may migrate and obstruct the trabecular meshwork. The risk is higher in patients with pre-existing glaucoma or high myopia.
Use of anticoagulants: These make hyphema more likely in iris chafing syndrome.
IOL material and design: Single-piece acrylic IOLs are more prone to cause UGH syndrome when inserted extracapsularly. Even with three-piece IOLs, the risk of iris contact varies depending on the angle and length of the haptics.
The following examinations are performed to identify the mechanism of IOP elevation.
Gonioscopy: Assessment of open or closed angle, presence of peripheral anterior synechiae, degree of trabecular pigmentation, and identification of lens particles or pseudoexfoliation material.
Slit-lamp microscopy: Evaluation of anterior chamber inflammation, hemorrhage, retained ophthalmic viscosurgical devices, and IOL position and stability. It is important to assess IOL decentration or tilt, association with capsular contraction, and correct positioning of sulcus-fixated IOLs. Evaluation of Elschnig pearls, posterior capsule opacification, and capsular contraction is also performed.
UBM (ultrasound biomicroscopy): Evaluation of the contact relationship between the IOL haptic and the iris/ciliary body. Useful for confirming UGH syndrome and iris chafing syndrome.
Optic nerve and visual field evaluation: Assessment of progression of pre-existing glaucoma and detection of new glaucomatous changes. Measurement of retinal nerve fiber layer (RNFL) thickness by OCT is useful for detecting early changes.
Anterior chamber flare measurement: Laser flare photometry allows quantitative assessment of anterior chamber inflammation. Useful for longitudinal monitoring of postoperative inflammation.
In differential diagnosis, systematically exclude each of the following mechanisms.
Differential Diagnosis
Characteristic Findings
Retained ophthalmic viscosurgical device
Onset hours to 1 day postoperatively; spontaneous resolution
The diagnosis of steroid-induced glaucoma is confirmed when elevated intraocular pressure occurs in a patient using steroids and normalizes after discontinuation. The time to normalization is proportional to the duration of steroid use. After triamcinolone use, elevated intraocular pressure may persist for 9 to 12 months, requiring long-term follow-up.
In the diagnosis of lens particle glaucoma, in addition to elevated intraocular pressure days to weeks after extracapsular extraction or trauma, large white particles suspected to be lens material floating in the anterior chamber are observed. It is often accompanied by anterior chamber inflammation, but differentiation from phacolytic glaucoma and phacoanaphylactic glaucoma is important.
QHow is UGH syndrome diagnosed?
A
UGH syndrome is characterized by the triad of uveitis, glaucoma, and hyphema2)3). Recurrent hyphema is the most characteristic finding. UBM examination is important to confirm contact between the IOL haptic and the iris or ciliary body. It occurs more frequently with anterior chamber IOLs or ciliary sulcus-placed IOLs, but can also occur with in-the-bag IOLs if there is zonular instability due to pseudoexfoliation syndrome. Differentiation from iris neovascularization and other causes of bleeding is necessary. In iris chafing syndrome, iris atrophy is the main finding, and recurrent hyphema is common, but IOL malposition plays a larger role.
Transient intraocular pressure elevation due to residual ophthalmic viscosurgical device or postoperative inflammation often resolves with conservative treatment using glaucoma eye drops (beta-blockers, carbonic anhydrase inhibitor eye drops) or oral carbonic anhydrase inhibitors (acetazolamide). If there is marked intraocular pressure elevation (40 mmHg or higher), consider anterior chamber paracentesis for decompression 11). Prophylactic administration of carbonic anhydrase inhibitors or beta-blockers in the early postoperative period has been reported to suppress intraocular pressure elevation 5 hours or more after surgery 4).
After cataract surgery, trauma, or YAG laser posterior capsulotomy, lens material may be released, obstructing the trabecular meshwork and causing elevated intraocular pressure. It typically occurs within a few days after surgery, and the degree of pressure elevation is proportional to the amount of residual lens fragments. It is often transient.
Anti-inflammatory and intraocular pressure-lowering medications: Combination of steroid eye drops and intraocular pressure-lowering medications
Anterior chamber washout: Performed when drug therapy is ineffective
Complete removal of lens cortex: If cortex remains, remove completely
This is a common mechanism occurring during postoperative steroid eye drop management after cataract surgery. Increased extracellular matrix production and cytoskeletal changes in trabecular meshwork cells contribute to elevated intraocular pressure.
Reduction or discontinuation of steroids: Reduce or discontinue steroids as much as possible. Decision is made in consideration of inflammation control of the primary disease.
Intraocular pressure-lowering medications: Various eye drops and oral carbonic anhydrase inhibitors
Surgical treatment (when drug control is poor or visual function impairment progresses):
Trabeculotomy: First choice because many cases are young and complications are few. Postoperative management is easy.
Trabeculectomy: Selected when lower postoperative intraocular pressure is required
Triamcinolone use cases: Removal of intravitreal remnants or excision of sub-Tenon’s capsule mass may be effective in some cases
It has been reported that outflow reconstruction surgery achieves greater intraocular pressure reduction than in POAG (evidence level 1B) 1)
Long-term effects of steroid eye drops and atropine eye drops are low. Once a definitive diagnosis is made, removal of the IOL irritating the iris is the first choice. After removal, insert an IOL with a shorter vertical diameter, or perform IOL suturing or intrascleral fixation.
If medical therapy fails to control the condition, surgical treatment is performed2)3).
Open-angle mechanism: Consider outflow reconstruction surgery. For steroid-induced glaucoma, trabeculotomy is the first choice.
Angle-closure mechanism: Consider goniosynechialysis or trabeculectomy.
Pseudophakic eye: Since trabeculectomy outcomes are poorer than in phakic eyes, glaucoma drainage devices (tube shunt surgery) are also an option2)3).
Postoperative glaucoma in children: Treatment follows that for primary congenital glaucoma (PCG)1). Due to poor surgical outcomes, tube shunt surgery with a plate may eventually be required1).
QHow is chronic glaucoma after cataract surgery managed?
A
First, identify the mechanism of intraocular pressure elevation. For open-angle mechanisms, medical treatment similar to POAG is given1). For angle-closure mechanisms, consider LPI or goniosynechialysis. In steroid-induced glaucoma, reducing or discontinuing steroids is most important; if surgery is needed, trabeculotomy is the first choice. If medical therapy is insufficient, proceed to surgery, but in pseudophakic eyes, trabeculectomy outcomes are poor, so consider using a glaucoma drainage device2). If IOL-related issues (pigment dispersion, UGH syndrome) are the cause, IOL exchange is the definitive treatment.
QWhat are the precautions when using glaucoma eye drops after cataract surgery?
A
Omidenepag (Eybelis) is contraindicated in eyes with IOL implantation or aphakia and cannot be used. Even if one eye is phakic, it is contraindicated at the patient level, so Eybelis cannot be prescribed. Other PG preparations (latanoprost, travoprost, etc.), beta-blockers, carbonic anhydrase inhibitors, and alpha-2 agonists can be used as for POAG1). During postoperative steroid eye drops, there is a risk of steroid-induced glaucoma, so carefully monitor the steroid potency, dose, duration, and intraocular pressure trends.
In open-angle mechanisms, viscoelastic substances, inflammatory cells, pigment granules, lens particles, ghost cells, etc., obstruct the trabecular meshwork. Persistent stimulation of the trabecular meshwork leads to fibrosis and chronic increase in aqueous outflow resistance.
Viscoelastic substances: Dispersive OVDs have small particle sizes and easily enter the trabecular meshwork, posing a higher risk of postoperative IOP elevation compared to cohesive types. Cohesive types are easier to remove as a mass, but if retained in the angle, they similarly elevate IOP.
Steroid-induced glaucoma: The core pathology involves increased extracellular matrix production and cytoskeletal changes in trabecular meshwork cells. Individual susceptibility varies greatly, and it is more common in children and the elderly. The IOP-elevating effect correlates with the anti-inflammatory potency of steroids: dexamethasone ≥ betamethasone > fluorometholone. It is dose-dependent and more pronounced in younger individuals. With triamcinolone, the drug remains in the eye for a long time, causing sustained IOP elevation for 9–12 months.
Pigment dispersion: The haptic or optic edge of the IOL contacts the posterior iris surface, mechanically stripping the iris pigment epithelium. Released pigment granules accumulate in the trabecular meshwork, increasing aqueous outflow resistance. This is particularly problematic with one-piece acrylic IOLs placed in the ciliary sulcus.
Adhesion between the iris and the anterior vitreous face (in aphakia) or pupil block by an IOL (anterior chamberIOL, sulcus IOL, reverse-inserted IOL) impedes aqueous humor flow into the anterior chamber2). Postoperative shallow anterior chamber and inflammation promote peripheral anterior synechiae formation, leading to chronic angle-closure glaucoma.
Pathophysiology of UGH syndrome: When an IOL is fixated outside the capsule or asymmetrically, the haptic directly contacts the iris or surrounding tissues. Iris chafing causes iris pigment to clog the trabecular meshwork, resulting in pigmentary glaucoma. Severe iris damage may be accompanied by iridocyclitis and hyphema2)3). This was more common with anterior chamber IOLs in the past, but now that in-the-bag fixation of posterior chamber IOLs is standard, its frequency is rare. It can occur with out-of-the-bag insertion of single-piece acrylic IOLs.
Pathophysiology of iris chafing syndrome: The haptic or optic edge of a posterior chamber IOL inserted out of the bag persistently chafes the iris or angle vessels. It was thought to be more common with angled loops or long-axis IOLs, but in reality, IOL malposition is often the cause. Secondary high IOP results from dispersion of iris pigment or hyphema. With current standard in-the-bag fixation, it is very rare.
Effects of Cataract Surgery on Intraocular Pressure
After cataract surgery, intraocular pressure is known to decrease due to deepening of the anterior chamber and widening of the angle following lens removal 8)10). A more significant reduction in intraocular pressure is achieved in angle-closure glaucoma4). Even in open-angle glaucoma, cases with higher preoperative intraocular pressure show a greater reduction 10). Poley et al. (2009) reported that the reduction in intraocular pressure at one year was maintained for 10 years 8).
Hayashi et al. (2001) examined intraocular pressure control after cataract surgery in glaucoma patients and showed that phacoemulsification and IOL implantation resulted in a significant reduction in intraocular pressure7).
Acharya et al. (2024), analyzing over 7.5 million cases from the IRIS Registry, reported that the incidence of persistent pseudophakic uveitis (PUPPI) was 1.68%, with diabetes (IRR 1.87), race, and sex as risk factors 5).
Pathophysiology of Glaucoma after Pediatric Cataract Surgery
In cases requiring cataract surgery during childhood, there may be associated developmental abnormalities of the aqueous outflow pathway 1). Anatomical changes in the anterior segment due to lens removal also contribute. It can occur in both aphakic and pseudophakic eyes, and in both open-angle and angle-closure glaucoma. Caution is needed because a thick central cornea may cause apparent high intraocular pressure1).
Recent advances in anterior segment optical coherence tomography (OCT) and UBM are enabling more precise evaluation of the postoperative angle and iris-IOL relationship. Quantitative assessment of IOL-iris contact, tilt, and decentration is expected to facilitate early diagnosis and preventive intervention for UGH syndrome and iris chafing syndrome. Anterior segment OCT can non-contact and non-invasively visualize angle structures with high resolution, making it useful for longitudinal monitoring of postoperative angle changes.
Improvements in IOL design and sizing algorithms have significantly reduced the risk of pigment dispersion and UGH syndrome. Optimization of IOL sizing based on axial length and anterior chamber depth, as well as improvements in material and haptic design, are progressing. However, addressing unpredictable risk factors such as exfoliation syndrome and zonular weakness associated with high myopia remains a future challenge.
With the development of MIGS (minimally invasive glaucoma surgery), options for postoperative intraocular pressure management through combined cataract and MIGS procedures are expanding. For patients with pre-existing glaucoma, simultaneous insertion of MIGS devices during cataract surgery is expected to improve postoperative intraocular pressure control.
For glaucoma after pediatric cataract surgery, long-term outcomes of long-tube drainage devices have been reported, and they are an important treatment option for cases that are difficult to manage with medication alone 2).
Acharya et al. (2024) calculated the incidence of PUPPI as 1.68% using data from over 7.5 million patients in the IRIS Registry 5). Diabetes (IRR 1.87), female sex, and African American race were independent risk factors, demonstrating the usefulness of large-scale real-world data surveillance for postoperative complications.
Levkovitch-Verbin et al. (2008) examined intraocular pressure elevation within 24 hours after cataract surgery in patients with glaucoma or PEX, and reported the importance of early postoperative intraocular pressure monitoring 9).
Chen et al. (2015) systematically reviewed intraocular pressure changes after phacoemulsification as an AAO report, confirming a medium-term intraocular pressure-lowering effect in glaucoma patients 10).
European Glaucoma Society. European Glaucoma Society Terminology and Guidelines for Glaucoma, 5th Edition. Br J Ophthalmol. 2021 Jun;105(Suppl 1):1-169. doi:10.1136/bjophthalmol-2021-egsguidelines. PMID:34675001.
Pazos M, Traverso CE, Viswanathan A; European Glaucoma Society. European Glaucoma Society - Terminology and guidelines for glaucoma, 6th Edition. Br J Ophthalmol. 2025;109(Suppl 1):1-212. doi:10.1136/bjophthalmol-2025-egsguidelines. PMID:41026937.
European Society of Cataract & Refractive Surgeons. ESCRS Clinical Guidelines: Cataract Surgery.
Acharya B, Hyman L, Tomaiuolo M, Zhang Q, Dunn JP. Prolonged Undifferentiated Postoperative Pseudophakic Iridocyclitis. Ophthalmology. 2025;132(4):504-506. doi:10.1016/j.ophtha.2024.12.012. PMID:39672310.
Bodh SA, Kumar V, Raina UK, et al. Inflammatory glaucoma. Delhi J Ophthalmol. 2011;21:37-41. doi:10.4103/0974-620x.77655.
Hayashi K, Hayashi H, Nakao F, et al. Effect of cataract surgery on intraocular pressure control in glaucoma patients. J Cataract Refract Surg. 2001;27:1779-86. doi:10.1016/s0886-3350(01)01036-7.
Poley BJ, Lindstrom RL, Samuelson TW, Schulze R Jr. Intraocular pressure reduction after phacoemulsification with intraocular lens implantation in glaucomatous and nonglaucomatous eyes: evaluation of a causal relationship between the natural lens and open-angle glaucoma. J Cataract Refract Surg. 2009;35(11):1946-55. doi:10.1016/j.jcrs.2009.05.061. PMID:19878828.
Levkovitch-Verbin H, Habot-Wilner Z, Burla N, et al. Intraocular pressure elevation within the first 24 hours after cataract surgery in patients with glaucoma or exfoliation syndrome. Ophthalmology. 2008;115:104-8. doi:10.1016/j.ophtha.2007.03.058.
Chen PP, Lin SC, Junk AK, Radhakrishnan S, Singh K, Chen TC. The Effect of Phacoemulsification on Intraocular Pressure in Glaucoma Patients: A Report by the American Academy of Ophthalmology. Ophthalmology. 2015;122(7):1294-1307. doi:10.1016/j.ophtha.2015.03.021. PMID:25943711.
Hildebrand GD, Wickremasinghe SS, Tranos PG, Harris ML, Little BC. Efficacy of anterior chamber decompression in controlling early intraocular pressure spikes after uneventful phacoemulsification. Journal of cataract and refractive surgery. 2003;29(6):1087-92. doi:10.1016/s0886-3350(02)01891-6. PMID:12842672.
Copy the article text and paste it into your preferred AI assistant.
Article copied to clipboard
Open an AI assistant below and paste the copied text into the chat box.