Ultrasound Biomicroscopy (UBM) is an imaging device used for diagnosing the anterior segment of the eye. It was first introduced in the early 1990s by Foster and Pavlin as a method to obtain cross-sectional images of the eye with microscopic resolution.
By using high-frequency ultrasound of 30–50 MHz, it provides high-resolution images of anterior segment structures (ciliary body, posterior iris, angle recess) that cannot be observed with a slit lamp. The high frequency achieves tissue resolution of 50–100 μm, optimized for evaluating the anterior segment depth of 5–10 mm.
Compared to conventional B-mode ultrasound (5–10 MHz), the depth of penetration is limited (5–10 mm), but the resolution is significantly improved. Since high-frequency waves are highly attenuated by tissue, low-frequency B-mode is separately needed to evaluate structures deeper than the choroid.
Uveitis: Assessment of cyclitic membranes and ciliary body edema
Post-glaucoma surgery: Evaluation of internal structure of filtering blebs
QHow does ultrasound biomicroscopy differ from conventional ultrasound?
A
Conventional B-mode ultrasound uses 5–10 MHz to observe the entire eye (axial length, retina, choroid, etc.). Ultrasound biomicroscopy uses high frequencies of 30–50 MHz to obtain high-resolution images with tissue resolution of 50–100 μm, specialized for the anterior segment. However, due to the high frequency, the depth of penetration is limited to 5–10 mm, and conventional ultrasound is needed to observe the posterior vitreous and retina.
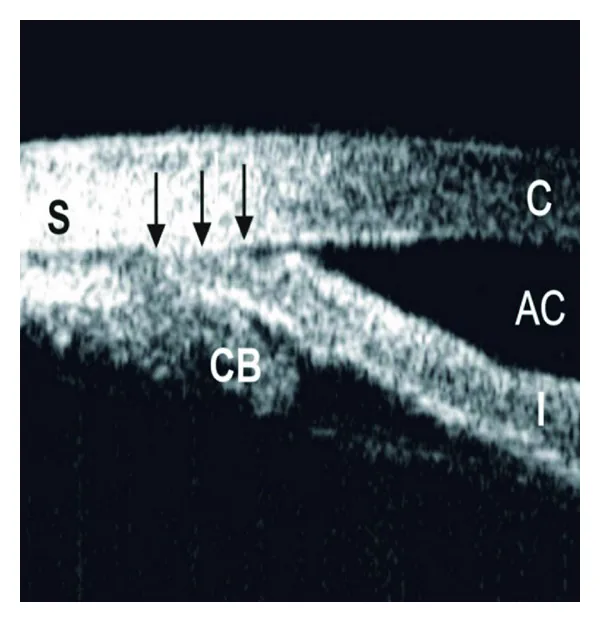
Dorairaj S, et al. Changing trends of imaging in angle closure evaluation. ISRN Ophthalmol. 2012. Figure 4. PMCID: PMC3914273. License: CC BY.
This is an ultrasound biomicroscopy image showing peripheral anterior synechia (PAS). S indicates sclera, CB indicates ciliary body, AC indicates anterior chamber, I indicates iris, C indicates cornea, and the black arrow indicates the extent of PAS. This corresponds to peripheral anterior synechia discussed in the section “2. Examination Techniques and Procedures”.
There is also a method using a probe cap filled with water (no eye cup required). Since examination can be performed in any position, it is suitable for patients who cannot tolerate the usual supine position.
Membrane-type ultrasound biomicroscopes (e.g., UD-8060, Tomey Corporation) do not require an eye cup; Scopisol® is applied to the membrane tip and placed on the examination site. This allows examination in a sitting position.
3. Quantitative Parameters and Interpretation of Findings
Ultrasound biomicroscopy enables quantitative measurement of the anterior chamber angle, and the following parameters are standardly used.
Parameter
Definition
AOD500 (Angle Opening Distance)
Vertical distance between the trabecular meshwork and iris at 500 μm anterior to the scleral spur
ARA (Angle Recess Area)
Area of the triangle bounded by the AOD line and the angle recess
ACD (Anterior Chamber Depth)
Distance from the central corneal endothelium to the anterior lens surface
Lens vault
Distance of the lens located anterior to the vertical line connecting the left and right scleral spurs
The detailed definition of AOD500 is “the vertical distance between the trabecular meshwork and iris at 500 μm anterior to the scleral spur,” and accurate identification of the scleral spur determines measurement accuracy. In primary angle closure glaucoma (PACG), AOD500 and anterior chamber depth are significantly reduced, aiding in diagnosis.
The anterior and posterior surfaces of the cornea, the scleral surface, and the anterior and posterior surfaces of the iris are visualized as high brightness. The corneal stroma, iris stroma, and ciliary body are low brightness. In a normal eye, the iris is slightly convex anteriorly or flat, and the ciliary sulcus can be identified between the iris and the ciliary processes.
In the observation of the anterior chamber angle, identification of the scleral spur and Schwalbe’s line is essential. The scleral spur is a part of the sclera that protrudes into the anterior chamber, with the trabecular meshwork attached anteriorly, and is an important landmark that can always be confirmed.
4. Clinical Significance and Findings in Major Diseases
Anterior iris bowing: A morphology where the posterior chamber pressure increases and pushes the iris forward.
Generalized angle narrowing: The iris is pressed against the cornea from the area of Schwalbe’s line.
Angle closure worsens in the dark: The condition aggravated by mydriasis can be observed.
Plateau Iris
No iris bowing: The central iris is flat and not accompanied by pupillary block.
Anteriorly positioned ciliary body and loss of ciliary sulcus: Characteristic findings. The ciliary body is displaced anteriorly, mechanically pushing the iris root upward.
Iris root occludes the angle upon mydriasis: Closure can be confirmed under darkroom mydriasis.
In plateau iris, the central anterior chamber is relatively deep, the central iris is flat, the iris root is thick and bends toward the anterior chamber, and the angle recess is slit-like narrowed. Anterior displacement of the ciliary body and loss of the ciliary sulcus are characteristic findings.
Observation with ultrasound biomicroscopy is extremely useful for the definitive diagnosis of plateau iris that is not relieved even after laser iridotomy. If intraocular pressure does not decrease after laser iridotomy, or if angle closure similar to the preoperative state is confirmed upon mydriasis, plateau iris is confirmed. Performing laser iridotomy solely for diagnosis should be avoided due to risks such as bullous keratopathy, and ultrasound biomicroscopy is recommended.
Approximately 33% of patients who have undergone laser iridotomy for primary angle-closure glaucoma have plateau iris, and this group has a high risk of peripheral anterior synechiae formation and further angle closure. 2)
Malignant glaucoma is an angle-closure glaucoma caused by anterior displacement of the vitreous due to anterior rotation of the ciliary body or abnormal aqueous flow into the vitreous cavity. Although idiopathic cases exist, confirming UBM findings along with surgical history is essential for diagnosis.
UBM reveals the following findings:
Anterior rotation of the ciliary body: The ciliary body is displaced forward, pushing the iris and ciliary body against the lens or vitreous.
Anterior displacement of the vitreous: Aqueous humor accumulates in the vitreous cavity, causing the entire vitreous to move forward.
360-degree angle closure: The angle is closed circumferentially without presenting a pupillary block pattern.
The vault (gap between the ICL and the anterior lens surface) after ICL (Implantable Collamer Lens) implantation is quantitatively assessed using UBM. The appropriate vault range varies by model and axial length, but insufficient vault (<250 μm) increases the risk of cataract progression, while excessive vault (>1000 μm) increases the risk of corneal endothelial damage and shallow anterior chamber. UBM is also used for monitoring vault changes during long-term follow-up (1–2 times per year). 3)
Sudden increase in intraocular pressure due to external force can cause angle recession, iridodialysis, trabecular meshwork damage, and cyclodialysis. In cyclodialysis, accumulation of aqueous humor in the suprachoroidal space is clearly visualized by ultrasound biomicroscopy.
Yeilta et al. reported a case of an iris-ciliary body melanocytoma measuring 5×3×2 mm that was visualized by ultrasound biomicroscopy (as a relatively well-defined lesion) and used for clinical diagnosis and management. 1) Even in cases of heavily pigmented tumors or intraocular tumors with corneal opacity, the posterior border can be identified, improving the accuracy of detecting invasion into adjacent structures.
QWhy is plateau iris difficult to diagnose?
A
Plateau iris is difficult to differentiate from pupillary block angle closure because the anterior chamber is not shallow (central anterior chamber depth is normal) and the iris does not bulge forward on slit-lamp examination. Confirming anterior rotation of the ciliary body and disappearance of the ciliary sulcus by ultrasound biomicroscopy under dark-room mydriasis is key to diagnosis.
Ultrasound biomicroscopy itself is an examination device and does not perform treatment. The treatment of diseases diagnosed by ultrasound biomicroscopy is described below.
Laser iridotomy (LPI/LI): First-line treatment. It creates a communication between the posterior and anterior chambers, eliminating the pressure gradient of aqueous humor flow.
Cataract surgery: Replacing the lens with an IOL increases anterior chamber depth and can widen the angle.
Pilocarpine eye drops: Conservative treatment. Effect is uncertain, and caution is needed for side effects from long-term use (poor dilation, posterior synechiae, cataract progression).
Vault insufficiency: ICL exchange (upsize) or early cataract surgery
Vault excess: ICL exchange (downsize) or ICL removal
QHow are abnormalities found on UBM examination treated?
A
For angle-closure glaucoma (pupillary block type), laser iridotomy or cataract surgery is selected; for plateau iris, laser gonioplasty (LGP) is chosen. For malignant glaucoma (ciliary body anterior rotation), cyclophotocoagulation or vitrectomy is indicated. In cases of vault abnormality after ICL, ICL exchange or ICL removal is considered. The treatment strategy is determined based on the mechanism of closure confirmed by ultrasound biomicroscopy.
Ultrasound biomicroscopy uses high-frequency ultrasound (30–50 MHz). The physical principles are as follows.
Wavelength: 50–30 μm (corresponding to 30–50 MHz)
Tissue resolution: 50–100 μm (axial)
Signal generation principle: Reflection intensity changes due to differences in acoustic impedance of tissues, forming tomographic images
Optimized for the anterior segment: Frequency band optimal for evaluating depths of 5–10 mm
Depth limitation: High-frequency ultrasound attenuates significantly in tissue, so low-frequency B-mode (5–10 MHz) is used to evaluate structures deeper than the choroid.
The greatest strength of ultrasound biomicroscopy is the visualization of structures including the posterior iris and ciliary body. Disadvantages compared to AS-OCT include the need for ocular contact via water-bath immersion, longer image acquisition time, and the requirement for a skilled examiner.
Differences in tumor evaluation: For ocular surface squamous neoplasia (OSSN), AS-OCT is superior in showing detailed internal lesion architecture. In contrast, for amelanotic iris tumors, ultrasound biomicroscopy has better ability to identify the posterior border of the lesion and higher reproducibility.
Mechanisms of angle-closure glaucoma and the role of ultrasound biomicroscopy
There are two main mechanisms of angle-closure glaucoma.
Relative pupillary block: Increased posterior chamber pressure causes the iris to bow forward, occluding the angle. UBM shows anterior iris bowing and generalized angle narrowing.
Plateau iris mechanism: Congenital anterior positioning of the ciliary body mechanically pushes the iris root upward. UBM shows anterior ciliary body positioning and loss of the ciliary sulcus.
Preoperative differentiation of these two mechanisms using ultrasound biomicroscopy can optimize treatment strategy (laser iridotomy alone vs. LI + LGP).
Automated quantitative analysis software for ultrasound biomicroscopy images has been developed, enabling automatic measurement of parameters such as angle opening distance, anterior chamber depth, and lens vault. It is expected to reduce inter- and intra-observer variability and improve diagnostic accuracy.
Ultrasound Biomicroscopy in the Management of Melanocytoma
In a case report by Yeilta et al., for pigmentary glaucoma secondary to necrotic iris melanocytoma, ultrasound biomicroscopy was used to evaluate lesion size (5×3×2 mm), and surgical management combining iridocyclectomy and glaucoma shunt surgery was shown to be effective. 1) The diagnostic yield of fine-needle aspiration biopsy (FNAB) is reported to be 88–95%, and ultrasound biomicroscopy findings play a supportive role in differentiating melanocytoma from melanoma.
Research on angle classification and automated diagnosis of UBM images using deep learning is ongoing. It is expected to be applied for early screening of angle-closure glaucoma, but clinical implementation has not yet been achieved. 4)
Gonzalez-Lopez F, Bilbao-Calabuig R, Mompean B, et al. Assessing vaulting changes after phakic collamer lens implantation by ultrasound biomicroscopy and optical coherence tomography. Eur J Ophthalmol 2016;26:36–41.
Jiang H, Wu Z, Lin Z, et al. Machine learning approaches to distinguish angle-closure from open-angle glaucoma using anterior segment features: a systematic review. Br J Ophthalmol 2022;106:1452–1458.
Copy the article text and paste it into your preferred AI assistant.
Article copied to clipboard
Open an AI assistant below and paste the copied text into the chat box.