Gonioscopy is a contact examination for direct observation of the anterior chamber angle. It provides essential information for diagnosing glaucoma subtypes, determining treatment strategies, and postoperative evaluation by observing the angle, which is the aqueous humor outflow pathway 3). Many diseases other than glaucoma also present abnormal findings in the angle, and it is considered one of the basic ophthalmic examinations.
Gonioscopy should be performed in the following situations.
Glaucoma evaluation at initial visit or when intraocular pressure is elevated
Before and after glaucoma surgery that approaches the angle (MIGS, trabeculectomy)
Evaluation of conditions involving uveitis or anterior segment inflammation
Angle evaluation after ocular trauma
Search for causes of secondary glaucoma (pseudoexfoliation, pigment dispersion, neovascularization, post-traumatic)
The Glaucoma Clinical Practice Guidelines (5th edition) consider gonioscopy essential in glaucoma care and assign a recommendation level of 1A 3).
QWhy is gonioscopy necessary for all glaucoma evaluations?
A
Gonioscopy is essential for classifying glaucoma and is extremely important for determining treatment strategy. Because conditions such as plateau irisglaucoma can have nearly normal central anterior chamber depth despite narrow angles or angle closure, evaluation of anterior chamber depth alone is insufficient. Gonioscopy should be performed in all cases to check for pseudoexfoliation material, pigment dispersion, neovascularization, inflammatory deposits, angle recession, and peripheral anterior synechiae, which can cause secondary glaucoma.
Gonioscopy should be performed in all patients undergoing glaucoma evaluation 2).
Evaluation of Primary Glaucoma
Diagnosis of primary open-angle glaucoma: Careful evaluation of the anterior chamber angle is necessary to rule out angle-closure glaucoma and secondary causes of elevated intraocular pressure4).
Evaluation of primary angle-closure disease: In patients suspected of having primary angle-closure disease, bilateral gonioscopy is mandatory to assess iridocorneal touch (ICT), peripheral anterior synechiae, and plateau iris configuration 5).
Ocular hypertension: Gonioscopy is essential for a thorough workup to rule out secondary causes of elevated intraocular pressure6).
Postoperative evaluation: Important for assessing the condition of the aqueous outflow pathway after MIGS or trabeculectomy, and for evaluating blood clots, iris incarceration, and peripheral anterior synechiae formation.
Others: Also indicated for evaluation of anterior chamber tumors, intraocular foreign bodies, and post-traumatic conditions.
Gonioscopy is fundamental to the staging of primary angle closure disease. The presence or absence of iridotrabecular contact (ITC) of 180 degrees or more is the starting point for staging5).
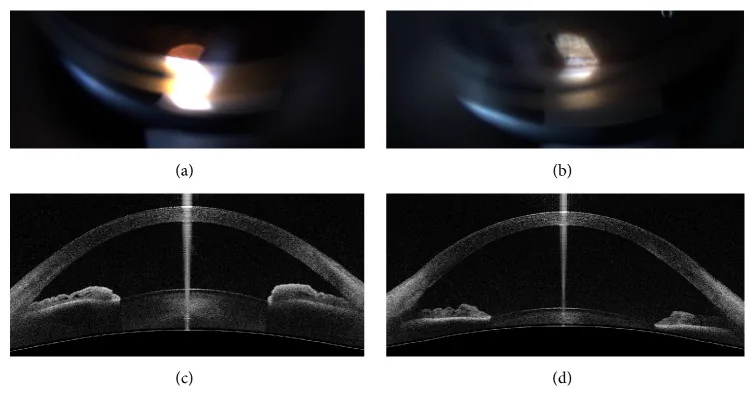
Rigi M, Bell NP, Lee DA, et al. Agreement between Gonioscopic Examination and Swept Source Fourier Domain Anterior Segment Optical Coherence Tomography Imaging. J Ophthalmol. 2016;2016:1727039. Figure 1. PMID: 27990300; PMCID: PMC5136403; DOI: 10.1155/2016/1727039. License: CC BY.
(a) Gonioscopy photograph of a narrow angle and (b) an open angle. In (a), the angle is narrow enough to identify Schwalbe’s line, trabecular meshwork, and scleral spur; in (b), all angle structures including the ciliary body band are clearly observed. These correspond to the landmarks Schwalbe’s line, trabecular meshwork, scleral spur, and ciliary body band discussed in section “3. Anatomy of the angle.”
The normal angle structures, from the corneal side to the iris side, are arranged in the following order3).
Schwalbe’s line: Corresponds to the posterior end of Descemet’s membrane and appears as a white linear ridge protruding into the anterior chamber. In exfoliation glaucoma, wavy pigmentation (Sampaolesi’s line) may be seen anterior to Schwalbe’s line3).
Trabecular meshwork: Located between Schwalbe’s line and the scleral spur. The portion from the middle to the scleral spur corresponds to the functional trabecular meshwork and is observed as a pigmented band. In exfoliation glaucoma and pigmentary glaucoma, marked pigmentation is present3).
Scleral spur: Observed as a white line between the ciliary body band and the trabecular meshwork. Iris processes may be seen on its surface. In pediatric glaucoma, the iris may attach anterior to the scleral spur, making it unobservable3).
Ciliary body band: Corresponds to the anterior surface of the ciliary body and appears as a gray-black band. In traumatic angle recession, the width of the ciliary body band increases3). Even in normal angles, there is variation in the degree of opening; in high myopia, the ciliary body band tends to be wide, while in hyperopia it tends to be narrow.
Angle vessels: Physiologically, ciliary vessels may be observed, but they show concentric or radial regular patterns. Pathological neovascular vessels are irregular, tortuous, and have many branches3). They may be missed when blood flow is interrupted under high intraocular pressure.
4. Examination techniques and classification methods
Since this is a contact examination, topical anesthetic eye drops are administered. Ethyl cellulose (Scopisol®) is applied to the contact lens, and it is placed on the eye to avoid air bubbles between the lens and the cornea.
Before gonioscopy, screening is performed using the van Herick method. The patient looks straight ahead, and a slit beam is directed at the temporal limbus at a 60-degree angle. The ratio of peripheral corneal thickness to peripheral anterior chamber depth is measured.
Criteria: Grade 2 or less (anterior chamber depth/corneal thickness ≤ 1/4) suggests possible angle closure, and gonioscopy should be performed3).
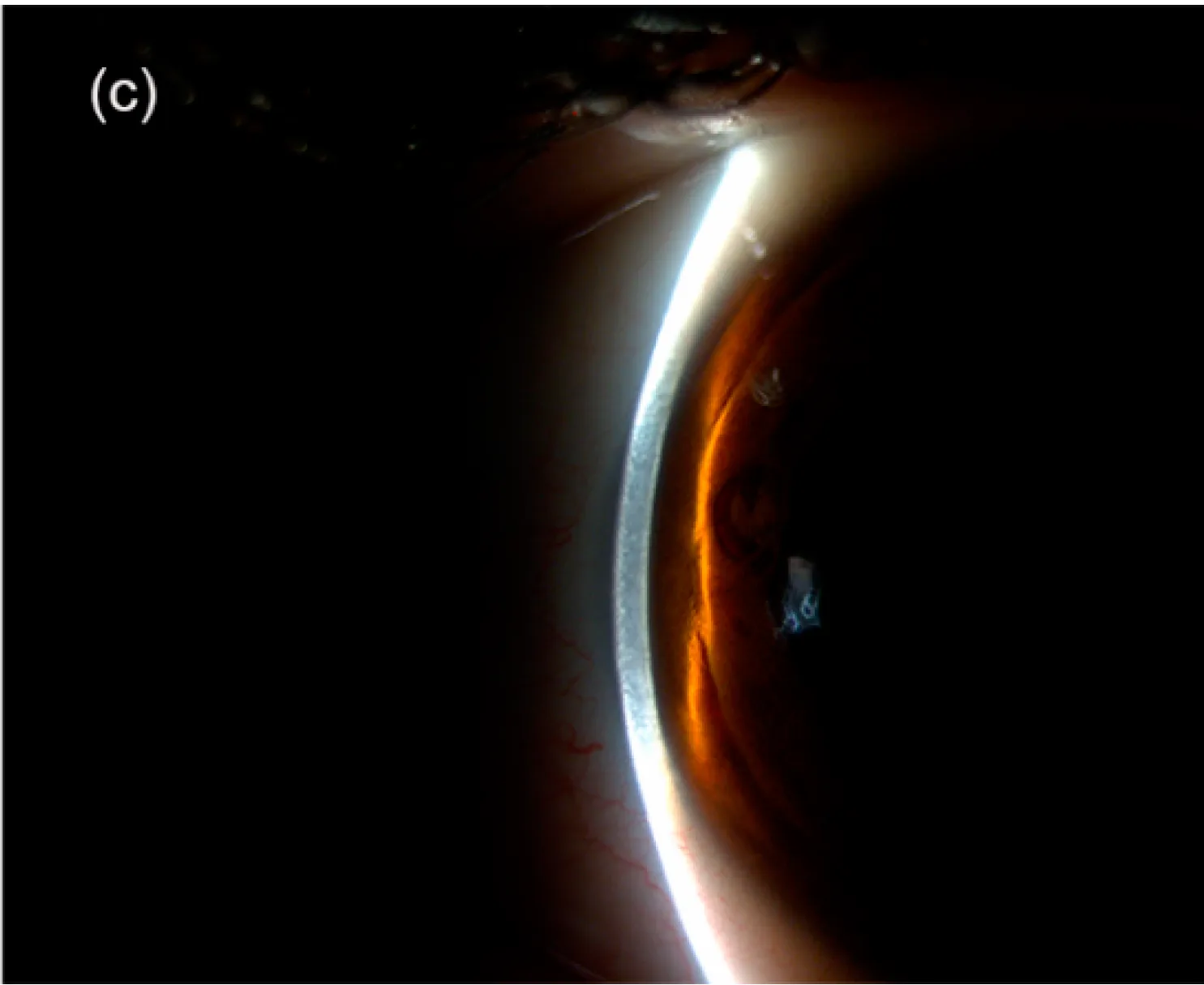
Riva I, Micheletti E, Oddone F, et al. Anterior Chamber Angle Assessment Techniques: A Review. J Clin Med. 2020;9(12):3814. Figure 4(c), cropped. PMID: 33255754; PMCID: PMC7759936; DOI: 10.3390/jcm9123814. License: CC BY 4.0.
Slit-lamp photograph of the van Herick method (limbal anterior chamber depth measurement). A slit beam is directed at the peripheral cornea to visually compare peripheral anterior chamber depth with corneal thickness.
Gonioscopy includes direct gonioscopy using a direct gonioscope and indirect gonioscopy using an indirect gonioscope3).
Direct gonioscopes (Koeppe, Barkan, Swan-Jacob, Hill lenses) are used with the patient in the supine position. They are mainly used in children or during surgery.
Indirect gonioscopes (Goldmann single-mirror, Zeiss four-mirror) can be used with the patient seated at a slit lamp and are most commonly used in daily practice. Note that the image is a mirror image. The Goldmann single-mirror has a higher and steeper mirror, making it suitable for observing the angle recess in narrow angles. The four-mirror allows observation of the entire circumference without rotation and can also be used for indentation gonioscopy.
For accurate diagnosis of angle closure, both static and dynamic gonioscopy should be performed3).
Static gonioscopy: In a dark room, with the slit lamp light intensity as low as possible and avoiding light entering the pupil, the angle opening is assessed without pressing on the eye, under natural pupil conditions3). It cannot differentiate functional from organic closure.
Dynamic gonioscopy: The slit lamp light intensity is increased to induce miosis, and the gonioscope or eye position is tilted to better visualize the angle recess3). It diagnoses the presence and extent of organic closure, nodules, and neovascularization.
Indentation gonioscopy: The center of the cornea is compressed to deform it, moving aqueous humor and pushing the peripheral iris posteriorly to observe the angle recess3). It is the only method that can differentiate functional closure (relative pupillary block) from organic closure (PAS). Care must be taken because excessive pressure can cause Descemet’s membrane folds, which may be mistaken for organic closure.
QWhen is compression gonioscopy necessary?
A
It is performed when the angle is extremely narrow and it is difficult to differentiate functional from organic closure by static and dynamic gonioscopy. A gonioscope with a small contact area with the cornea is used to compress the central cornea, displacing aqueous humor and pushing the peripheral iris posteriorly to observe the angle recess. In areas with peripheral anterior synechiae, the iris is not pushed down, and the trabecular meshwork or angle recess cannot be observed. Excessive compression may reduce visibility due to Descemet’s membrane folds, risking misdiagnosis as organic closure.
It is classified by the angle between the trabecular meshwork and the peripheral iris3).
The main landmarks observed on gonioscopy are Schwalbe’s line, trabecular meshwork, scleral spur, and ciliary body band7). A modified Shaffer grading table incorporating visible structures has also been reported8).
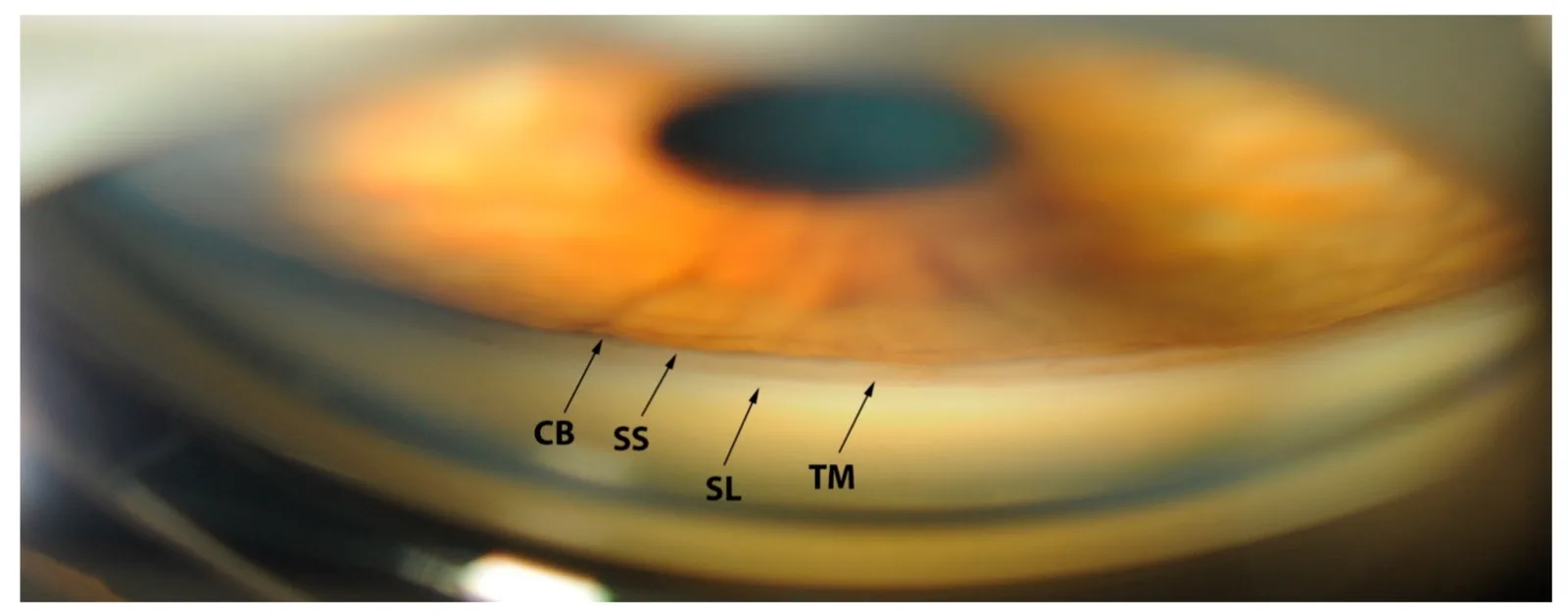
Riva I, Micheletti E, Oddone F, et al. Anterior Chamber Angle Assessment Techniques: A Review. J Clin Med. 2020;9(12):3814. Figure 2. PMID: 33255754; PMCID: PMC7759936; DOI: 10.3390/jcm9123814. License: CC BY 4.0.
Gonioscopic landmarks: SL, Schwalbe’s line; TM, trabecular meshwork; SS, scleral spur; CB, ciliary body band. In Shaffer grading, wider angles generally allow more posterior structures to be seen.
Classification is based on the visible structures 3). Grade 0 (WIDE) shows all structures, while Grade IV is the narrowest state where even Schwalbe’s line is not visible.
Grade
Visible range of angle structures
IV
Cannot be observed
III
Posterior half of trabecular meshwork cannot be observed
The morphology of the angle is described by three factors: the site of iris attachment, the angle of iris insertion, and the peripheral iris shape (concave q, flat r, convex s). A high correlation with ultrasound biomicroscopy has been reported 4).
In gonioscopy, it is important not to overlook the following abnormal findings. Many findings, such as angle nodules and neovascularization, can only be confirmed with sufficient magnification. Carefully observe the entire circumference.
Peripheral anterior synechia (PAS): Adhesion between the angle and peripheral iris, with various shapes such as tent-shaped, trapezoidal, or broad planar forms 3). It occurs in primary angle closure glaucoma, as well as neovascular glaucoma, uveitis, ICE syndrome, after blunt trauma, and after laser or intraocular surgery. The height varies from slight involvement of the scleral spur to complete occlusion of the trabecular meshwork.
Pathological neovascularization: Secondary to ocular ischemic conditions, new vessels arise from the iris root and form fine branches 3). Once the open-angle phase transitions to the closed-angle phase, intraocular pressure control becomes difficult. During high intraocular pressure, blood flow may be interrupted, making them easy to overlook.
Pigmentation: In exfoliation glaucoma, a pigmented band extending beyond Schwalbe’s line (Sampaolesi line) is characteristic 3). In pigmentary glaucoma, the entire trabecular meshwork shows uniform heavy pigmentation.
Angle recession: Seen after blunt trauma, this finding shows widening of the ciliary body band 3). The extent and width vary depending on the severity of the trauma.
Angle dysgenesis (developmental glaucoma): In developmental glaucoma, high iris insertion is present. Compared to PAS, the width is narrower, and sponge-like iris processes are often observed. In Axenfeld-Rieger syndrome, cord-like uveal remnants and thickening of Schwalbe’s line (posterior embryotoxon) are seen.
Postoperative findings: Gonioscopy is essential for differentiating between blood clot adhesion, synechia, peripheral anterior synechia formation after MIGS, and blood clots or iris incarceration at the surgical site after trabeculectomy.
Childhood glaucoma is caused by elevated intraocular pressure due to various angle abnormalities. By age 4–5, examination similar to adults is possible, but adequate examination in the clinic is difficult and often requires general anesthesia or sedation.
Early-onset developmental glaucoma: Shows high iris insertion. The developmental abnormality is confined to the angle.
Late-onset developmental glaucoma: Identification of abnormalities on gonioscopy is difficult. Corneal enlargement is not observed.
Advantages: Allows non-contact observation of the angle, with less patient burden. Resolution is superior to UBM, and it has excellent quantifiability and reproducibility. It can scan all four quadrants simultaneously in a short time, non-contact and non-invasive 1).
Limitations: Cannot evaluate color information, so assessment of angle nodules, neovascularization, and angle pigmentation is not possible. It also cannot differentiate organic angle closure (PAS) 1). It detects more iridocorneal contact than gonioscopy and may produce false positives 1).
Role: Useful as an adjunct to gonioscopy, but not a replacement 2). The STAR360 program enables analysis of the three-dimensional structure of the angle in 128 directions around the entire circumference.
Ultrasound biomicroscopy (UBM)
Advantages: Allows cross-sectional observation of fine structures of the anterior segment including the angle, iris, and part of the ciliary body3). Excellent for imaging the ciliary body, and observation in complete darkness is possible. Angle evaluation is possible even with corneal opacity. Improvements have made it feasible in the sitting position.
Limitations: Contact method with greater patient burden. Resolution is inferior to OCT. Only provides a single tomographic image at an arbitrary location, limited to planar evaluation.
Role: Plays an important role in the diagnosis of plateau iris, malignant glaucoma, and secondary glaucoma due to iridociliary tumors.
360-degree angle camera
Features: Uses a 16-face multi-mirror prism to automatically and simultaneously capture and record the entire circumference of the angle. Provides a 360-degree color image of the angle, and is currently the only device that can evaluate color information.
Role: Can potentially replace static gonioscopy. However, dynamic and compression gonioscopy cannot be performed, so it does not completely replace gonioscopy. A representative device is the GS-1 by Nidek.
Gonioscopy allows evaluation of color tone, dynamic assessment via compression gonioscopy, and direct confirmation of peripheral anterior synechiae, which cannot be replaced by imaging in these aspects 2). On the other hand, imaging is superior for quantitative and objective documentation and is suitable for longitudinal comparison. It is important to use both complementarily.
QCan anterior segment OCT completely replace gonioscopy?
A
It cannot replace it. Anterior segment OCT is non-contact, has excellent quantifiability and reproducibility, and imposes less patient burden, but it is difficult to evaluate peripheral anterior synechiae, pigmentation, and fine abnormal findings (neovascularization, nodules, etc.). It also detects more iridocorneal contact than gonioscopy, potentially causing false positives. The European Glaucoma Society (EGS) guidelines also state that anterior segment imaging should not replace gonioscopy 2).
The Nidek GS-1 is a stationary contact-type gonioscopy device that uses a 16-mirror goniolens to capture and stitch together 360-degree angle images. Multi-focal imaging allows post-hoc adjustment of focus on different angle structures. It is expected to improve inter- and intra-observer agreement.
GonioPen is a handheld gonioscopy device developed in Singapore that provides high-resolution images of the iridocorneal angle. It is small, compact, and can be used by technicians with minimal training.
A smartphone camera with a slit-lamp adapter can capture gonioscopic photos and videos. Direct smartphone imaging without a slit lamp has also been reported. This is expected to be useful in areas with limited medical resources.
Conventional direct surgical goniolenses require tilting the head or microscope, but the double-mirror goniolens uses two internal mirrors to provide an upright view of the angle, allowing observation and manipulation of the entire circumference without tilting. With the development of MIGS, surgical goniolenses continue to evolve.
Pazos M, Traverso CE, Viswanathan A; European Glaucoma Society. European Glaucoma Society - Terminology and guidelines for glaucoma, 6th Edition. Br J Ophthalmol. 2025;109(Suppl 1):1-212. doi:10.1136/bjophthalmol-2025-egsguidelines. PMID:41026937.
European Glaucoma Society. European Glaucoma Society Terminology and Guidelines for Glaucoma, 5th Edition. Br J Ophthalmol. 2021 Jun;105(Suppl 1):1-169. doi:10.1136/bjophthalmol-2021-egsguidelines. PMID:34675001.