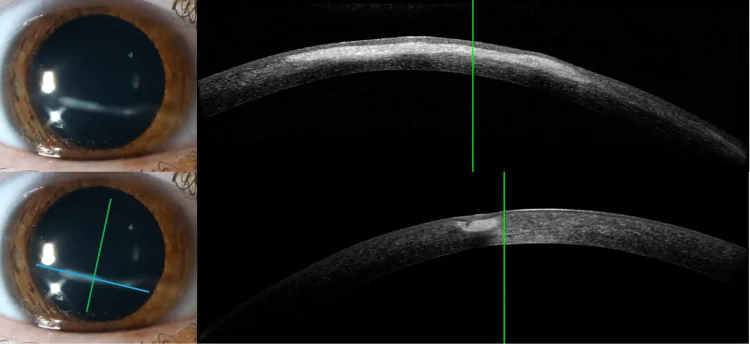
Barrientos LC, Wildes M. Linear Interstitial Keratitis: A Report of Two Cases and Review of Literature. Cureus. 2025. Figure 1. PMCID: PMC12010693. DOI: 10.7759/cureus.80985. License: CC BY 4.0.
Anterior segment examination images (upper left, lower left) showing a slit beam of light on the cornea using a slit lamp, and corresponding AS-OCT cross-sectional images (upper right, lower right). This corresponds to the observation of an optical section of the cornea using slit light, as discussed in the section “1. What is Slit Lamp Microscopy?”
A slit lamp (biomicroscope, abbreviated as SL or BM) is a biological microscope consisting of an illumination system (slit lamp) and an observation system (microscope). It is the most frequently used basic examination device in ophthalmology to detect lesions and abnormal findings in the anterior segment and transparent media, and to assess their extent, range, and characteristics. By using a pre-corneal lens, the observation range can be extended to the retina and vitreous body, and with a Goldmann three-mirror lens, the angle can be directly observed.
By changing the angle, width, and height of the slit light, optical sections from the cornea to the anterior vitreous can be observed, allowing differentiation of tissue depth and layer structure. Magnification can be continuously switched, typically from 6.3× to 40× (representative models such as Haag-Streit BQ900 and ZEISS SL 800 have 5 steps: 6.3×/10×/16×/25×/40×).
In 1911, Swedish physicist Allvar Gullstrand, in collaboration with Carl Zeiss, developed the slit lamp and mentioned it in his Nobel Prize lecture that same year. In the 1920s–1930s, Hans Goldmann established a parfocal design that aligned the focal points of the illumination and observation systems on the same plane, completing the basic form of the modern slit lamp. Haag-Streit began marketing it in 1958.
Tabletop (standard) type: Haag-Streit BQ900, ZEISS SL 800, RO8000, etc. Used routinely in daily practice.
Handheld (portable) type: Suitable for home visits, operating rooms, bedridden patients, and pediatric examinations.
Smartphone-attached (mobile) type: METORI-50, etc. Increasingly used in community medicine and telemedicine.
QIs slit lamp examination painful?
A
Routine anterior segment observation is performed without contact, so there is no pain. Fundus examination using a pre-corneal lens is also non-contact. Only when using a Goldmann three-mirror lens or gonioscope does contact with the ocular surface occur, requiring topical anesthesia (e.g., 0.4% oxybuprocaine hydrochloride eye drops).
Observation methods with the slit lamp are classified into the following seven types based on the relationship between the illumination and observation systems. Selecting the appropriate illumination method according to the target lesion improves diagnostic accuracy.
Direct, Indirect, and Diffuse Illumination Methods
Direct illumination: The focal points of the illumination and observation systems are aligned. The transparent media are observed as optical sections to evaluate tissue thickness, depth, and opacity depth. This method provides high-contrast visualization of opacities in the cornea and lens. Optical sections are obtained by varying the slit width and angle.
Indirect illumination: Surrounding tissues are observed using scattered light from the slit beam. By illuminating areas adjacent to the lesion, this method is effective for detecting faint opacities, corneal edema, anterior chamber flare, keratic precipitates (KP), and vitreous opacities.
Diffuse illumination (diffuser method): A method that captures the area as a whole. It is used to assess the overall appearance of structures such as conjunctival papillae, follicles, meibomian gland openings, and iris crypts.
Retroillumination, Transillumination, Scleral Scatter, and Specular Reflection Methods
Retroillumination (posterior illumination): The cornea is illuminated using light reflected from the iris or lens. This method can visualize keratic precipitates (KP), corneal edema, and fine, faint lesions.
Transillumination (retroillumination from fundus): Uses the red reflex from the fundus. It is effective for assessing the morphology and extent of lens opacities (posterior subcapsular cataract, retrodots), intraocular lens dislocation, and posterior capsule opacification.
Scleral scatter: The entire cornea is observed using scattered light from the sclera adjacent to the cornea. This is useful for detecting subtle lesions such as faint corneal opacities and radial keratoneuritis.
Specular reflection: The angle of incidence is adjusted to equal the angle of reflection, obtaining a specular reflection image of the corneal endothelium. This is applied to observe the shape and size of corneal endothelial cells and is the principle behind the specular microscope.
Anterior Chamber Depth Assessment by Van Herick Method
A method in which a slit beam is directed perpendicularly onto the temporal limbal cornea and observed at an angle of approximately 60°. The anterior chamber depth is evaluated by the ratio of the distance from the posterior corneal surface to the iris surface (PAC) to the corneal thickness (CT), and is used for screening narrow angles.
By combining a precorneal lens such as +60D, +78D, or +90D with a slit-lamp microscope, the retina, vitreous, and optic disc can be observed three-dimensionally under mydriasis. The image is inverted. This non-contact method is relatively easy to perform and is widely used in daily clinical practice. Using the central portion of a Goldmann-type three-mirror lens allows direct (contact) high-magnification observation, and the slit beam can be used to assess the extent and depth of cupping 2).
Using red-free light improves the contrast of disc hemorrhages and retinal nerve fiber layer defects, enhancing detection accuracy 1).
QWhy can so much information be obtained just by shining a slit light?
A
The illumination and observation systems of the slit-lamp microscope can be rotated independently, but their rotation axes are coaxial and the focal planes are also designed to be the same. When slit light is directed at tissue, an optical section is obtained, allowing the depth and layer structure of the tissue to be distinguished. By changing the angle, width, and height of the slit, it becomes possible to observe individual layers of the corneal epithelium, stroma, and endothelium, or to measure the depth of the anterior chamber.
In slit-lamp microscopy, it is recommended to systematically observe in the following order. The basic procedure is to first examine the overall view at low magnification (6.3–10×) and then scrutinize lesions at high magnification (16–40×).
The examination is performed in a dark or semi-dark room. The patient places their chin on the chin rest and adjusts so that the outer canthus aligns with the height indicator (mark on the forehead rest). Remove any bangs that obstruct the visual field, and contact lenses should be removed before the examination.
Procedure for Anterior Segment Examination
Magnification setting: Observe the entire area at 6.3–10× (low magnification). Examine in order: eyelids → conjunctiva → cornea.
Illumination adjustment: Adjust slit width, height, and angle (typically 45°) according to the purpose. Use cobalt blue filter (fluorescein staining) and red-free filter (RNFL/hemorrhage evaluation) as needed.
Fluorescein staining: After staining with 1% fluorescein test paper or eye drops, evaluate corneal epithelial defects and tear film patterns under cobalt blue light.
Anterior chamber inflammation evaluation: Set slit width to about 1 mm, height to 3 mm, and maximum brightness. Quantify cells (floating leukocytes) and flare (protein exudation) using the SUN classification (0–4+).
Lens evaluation: Determine nuclear hardness using the Emery-Little classification (Grade 1–5). Evaluate posterior subcapsular cataract using retroillumination. Maximum pupil dilation (tropicamide 0.5% + phenylephrine 0.5% combination eye drops) is required for detailed observation.
Procedure for Fundus and Optic Disc Examination
Dilation: Instill tropicamide 0.5% + phenylephrine 0.5% combination eye drops (Mydrin P®) to achieve sufficient dilation (usually after 20–30 minutes).
Holding the condensing lens: Hold a +78D (standard) or +90D (wide-angle) lens a few millimeters in front of the cornea.
Focusing: Project the slit light into the eye and focus on the inverted fundus image using the joystick.
Using the slit beam: Set the beam length to 1 mm or 2 mm and place it on the optic disc to assess the vertical diameter. Evaluate the cup-to-disc ratio (vertical cup diameter/vertical disc diameter).
Recording: Record findings by sketching or digital photography (slit lamp camera or smartphone-mounted adapter).
QIs mydriasis necessary?
A
Anterior segment observation (eyelids, conjunctiva, cornea, anterior chamber, iris, anterior lens) can be performed without mydriasis. Mydriasis is recommended for detailed observation of the fundus, posterior lens surface, and vitreous body. After mydriasis, photophobia and blurred vision persist for 4–6 hours, so advise the patient to avoid driving on the day. In patients at risk of angle closure (shallow anterior chamber, Van Herick Grade 1–2), evaluate the angle before mydriasis.
5. Representative abnormal findings and management
According to the Glaucoma Practice Guidelines (5th edition), the following quantitative criteria are set for suspected glaucoma2).
Vertical C/D ratio ≥ 0.7: Only about 5% of normal individuals exceed 0.7
R/D ratio ≤ 0.1: The rim is extremely thinned
Asymmetry ≥ 0.2: Seen in less than 3% of normal individuals
Deviation from the ISNT rule (rim width: inferior > superior > nasal > temporal), optic disc hemorrhage, and enlargement of β-zone peripapillary atrophy (PPA) are also findings suggestive of glaucomatous changes1)3). Morphological changes of the optic disc and retinal nerve fiber layer defects (RNFLD) may appear before visual field defects, making them important findings for early detection1).
The optical system of the slit lamp microscope consists of a combination of an illumination system and an observation system. The sophisticated design of both systems enables real-time cross-sectional observation of living tissue.
Illumination system: A convergent light beam from a halogen lamp (conventional) or LED light source (currently mainstream) is projected through a slit diaphragm. LEDs have a large short-wavelength component, which is advantageous for observing fine findings in the anterior chamber inflammation and vitreous. The slit width is continuously variable from 0 to 14 mm (varies by model).
Observation system: Keplerian binocular microscope. Zoom magnification ranges from 6.3× to 40×. The balance between observation magnification and resolution is adjusted according to the purpose.
Confocal design: The illumination and observation systems can rotate independently, but the rotation axis is coaxial and the focal plane is designed to be the same. Since the illumination light is always positioned at the center of the observed field, lesions can be reliably captured at the focal plane.
Optical section: When the slit light is narrowed and directed obliquely into the tissue, a cross-sectional image is obtained as if the tissue were cut. This principle allows individual identification of the corneal epithelium, stroma, and endothelium.
Gullstrand (1911): Inventor of the slit lamp. His optical insights as a physicist laid the foundation for ophthalmic diagnostics.
Integrated device with anterior segment OCT (AS-OCT): Integrated systems that quantitatively evaluate corneal cross-sections, angle morphology, and intraocular lens position abnormalities in real time are becoming more widespread. Complementary use with slit lamp findings is advancing.
AI-based anterior segment image analysis: AI is being introduced for automated cataract grading, quantitative evaluation of corneal opacities, and classification of KP patterns using slit lamp photographs. In the future, objective and automated staging of disease is expected.
Digital slit lamp and remote consultation: Standardized imaging using digital slit lamps with built-in high-resolution cameras and cloud-based remote consultation systems are becoming more widespread.
Enhanced functionality of portable slit lamps: Smartphone-attachable and handheld slit lamps continue to improve in optical performance, expanding their use in home healthcare, outreach clinics, and pediatric ophthalmology.
Pazos M, Traverso CE, Viswanathan A; European Glaucoma Society. European Glaucoma Society - Terminology and guidelines for glaucoma, 6th Edition. Br J Ophthalmol. 2025;109(Suppl 1):1-212. doi:10.1136/bjophthalmol-2025-egsguidelines. PMID:41026937.