Tear film breakup time (BUT) is a tear stability evaluation test that plays a central role in the diagnosis of dry eye. After fluorescein staining, the time from opening the eye until the tear film breaks up is measured in seconds.
According to a large-scale epidemiological study (Koumi Study) targeting residents aged 40 and over, the prevalence of dry eye is 12.5% in men and 21.6% in women, being more common in women and increasing with age 1). In the diagnosis of such a frequent disease, BUT is positioned as an essential indicator along with subjective symptoms.
The 2016 definition of dry eye states that it is “a disease in which the stability of the tear film is reduced due to various factors, causing ocular discomfort and visual dysfunction, and may be accompanied by ocular surface damage” 1), and reduced tear film stability has come to be regarded as the essence of dry eye. In the 2006 diagnostic criteria, cases with only shortened BUT and no epithelial damage (short BUT type dry eye) were classified as “suspected dry eye,” but with the 2016 revision, they are now definitively diagnosed and recognized as targets for treatment 1).
Short BUT type dry eye is characterized by shortened BUT but normal tear secretion, and strong subjective symptoms despite minimal epithelial damage 1). It also significantly affects visual function, with reports of increased higher-order aberrations after blinking and decreased functional visual acuity1).
QCan dry eye be diagnosed by BUT test alone?
A
A definitive diagnosis cannot be made by BUT test alone. According to the dry eye diagnostic criteria (2016 version), a definitive diagnosis of dry eye is made when both “subjective symptoms” and “BUT ≤5 seconds” are present. If there is only shortened BUT without subjective symptoms, the diagnostic criteria are not met. Conversely, if subjective symptoms are present but BUT is normal (≥6 seconds), other diseases must be excluded.
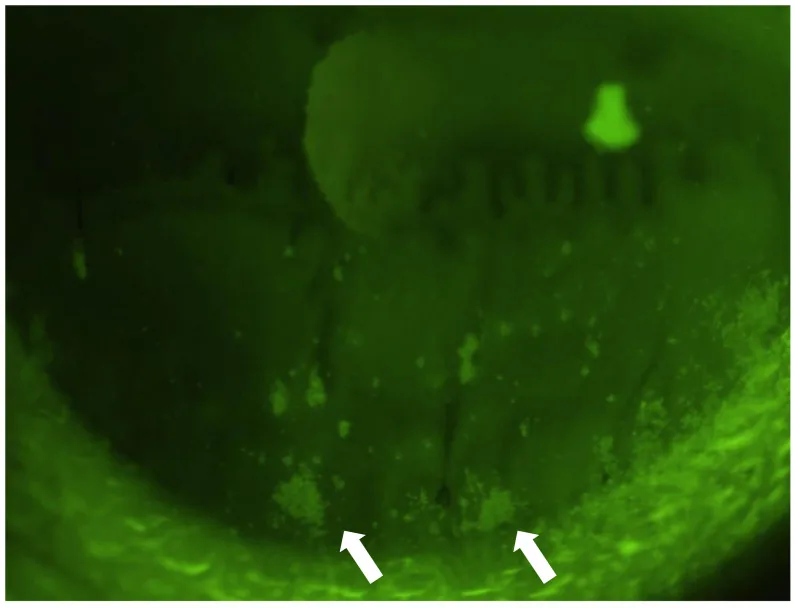
Komai S, et al. Clinical Implication of Patchy Pattern Corneal Staining in Dry Eye Disease. Diagnostics. 2021;11(2):232. Figure 1. PMCID: PMC7913618. License: CC BY.
Slit-lamp microscope image after fluorescein staining under cobalt blue light, showing punctate to patchy fluorescent staining in the lower cornea. This corresponds to the corneal fluorescence pattern during BUT observation with fluorescein staining discussed in the section “2. Examination Technique and Procedure.”
The accuracy of BUT measurement greatly depends on the staining technique. The most important point is to stain without changing the tear volume as much as possible.
Place 1–2 drops of saline on the fluorescein test strip, shake well, and remove excess moisture. Stain by lightly touching the wet end of the strip to the tear meniscus of the lower eyelid margin. Avoid direct contact of the test strip with the eyeball to prevent excess fluid from mixing with the tears, allowing accurate BUT values.
Ask the patient to close their eyes gently (instruct not to close tightly)
Instruct the patient to “open your eyes quickly” and maintain the eyelids open.
Observe the tear film using a cobalt blue filter (preferably with a barrier filter).
Measure the time in seconds from eyelid opening to tear film breakup.
Perform three measurements, calculate the average, and report as an integer (round to the nearest whole number).
If the initial eyelid opening is too forceful, the meibomian glands may be compressed, releasing excess lipids into the tear fluid, resulting in an abnormal BUT value. Gently closing the eyes can prevent this error. Additionally, rapid eyelid opening applies appropriate stress to the ocular surface, allowing accurate observation of tear film dynamics.
The blue-free filter improves image quality during observation under fluorescein staining. Many slit-lamp microscopes now come standard with this filter. Using this filter makes it easier to three-dimensionally capture the thickness and movement of the tear film, allowing clearer observation of tear film breakup. It improves the accuracy of identifying breakup patterns and enhances the precision of subtype classification (TFOD).
QWhy is the amount of fluorescein important?
A
If too much fluorescein solution is used, the tear volume during measurement increases, leading to BUT measurement under conditions of greater tear volume than normal. This may result in a longer BUT value than actual, potentially causing missed diagnosis of dry eye. Minimal staining, achieved by lightly touching the edge of the test strip to the tear meniscus, is a prerequisite for accurate BUT measurement.
The cutoff values for dry eye diagnosis are as follows.
Assessment
Criteria
Significance
Normal
≥6 seconds
Tear film stability is maintained
Abnormal
5 seconds or less
Meets diagnostic criteria for dry eye
Borderline
6 seconds
Comprehensive judgment with subjective symptoms required
According to the 2016 dry eye diagnostic criteria, a definitive diagnosis of dry eye is made when the following two conditions are met 1).
Subjective symptoms such as ocular discomfort and visual function abnormalities
Tear film breakup time (BUT) of 5 seconds or less
In the 2006 version, both quantitative tear abnormality (Schirmer I test ≤5 mm or BUT ≤5 seconds) and corneal/conjunctival epithelial damage were required. In the 2016 version, the presence of epithelial damage is no longer essential for diagnosis, with emphasis placed on “decreased tear film stability” 1). This revision allowed for definitive diagnosis of BUT-shortened dry eye, where BUT is shortened but epithelial damage is minimal.
BUT-shortened dry eye is often refractory and responds poorly to conventional artificial tears or hyaluronic acid eye drops, but improvement has been reported with diquafosol sodium (Diquas®) and rebamipide (Mucosta®) 1).
4. Tear Film Breakup Patterns (TFOD) and Clinical Significance
By differentiating breakup patterns under fluorescein staining, it is possible to identify which layer of the ocular surface (lipid layer, aqueous layer, mucin layer) is abnormal, allowing classification of dry eye subtypes. This diagnostic method is called tear film oriented diagnosis (TFOD) 1). TFOD enables subtype classification (aqueous-deficient, wetting-decreased, evaporative) not explicitly included in the 2016 dry eye diagnostic criteria, and allows selection of layer-specific treatment (TFOT) based on this 1).
The six breakup patterns and corresponding subtypes and first-line treatments are shown below.
Pattern
Characteristics
Subtype
First-line treatment
area break
Widespread breakup immediately after opening the eyes. Extremely low tear volume.
Area break: Seen when tear volume is extremely reduced. Widespread breakup occurs immediately after eye opening, with no upward movement of fluorescein or only limited downward movement. Since the main cause is insufficient tear volume, punctal plugs are the first choice.
Line break: A vertical linear breakup occurs in the lower cornea during upward extension of the lipid layer. Tear reduction and epithelial damage are mild to moderate. Diquafosol sodium is effective.
Decreased wettability type (spot, dimple, rapid expansion break)
Spot break: Caused by decreased corneal wettability. During the first stage of tear film formation, when water is spread over the corneal surface, it is repelled, resulting in a round breakup immediately after eye opening. Epithelial damage is absent or minimal.
Dimple break / Rapid expansion break: Occurs during lipid layer extension. Linear to irregular breaks near the central cornea. Diquafosol sodium and rebamipide, which act on membrane mucin function, are first-line treatments.
Increased evaporation type (random break)
Random break: Occurs after tear film formation (stages 1 and 2) is complete and the eyelids remain open. The location of breakup has low reproducibility (random). It is caused by increased evaporation of the aqueous layer, suggesting abnormalities in the lipid layer or secretory mucin.
Since it can also occur in normal conditions, it must be evaluated comprehensively with subjective symptoms and other findings. Diquafosol sodium eye drops combined with MGD treatment (warm compresses, eyelid hygiene) are recommended.
QWhat can be learned by observing the breakup pattern?
A
Observing the breakup pattern allows classification of dry eye subtypes (aqueous-deficient, wetting-deficient, evaporative). Since each subtype involves deficiency of different ocular surface components (aqueous, mucin, lipid), selecting a treatment (TFOT) that supplements the deficient component enables more pathophysiology-oriented therapy. For area/line break, punctal plugs; for spot/dimple/rapid expansion, diquafosol sodium or rebamipide; for random break, MGD treatment is first-line.
The concept of treating dry eye by supplementing deficient components on the ocular surface that cause tear film instability, thereby improving tear film stability, is called tear film oriented therapy (TFOT)1).
Oil layer stabilization and increased secretory mucin
Characteristics of Main Drugs
3% Diquafosol sodium ophthalmic solution (Diquas®) is used 6 times daily and has multifaceted actions: promoting water secretion from conjunctival epithelial cells, promoting secretion of secretory mucin (MUC5AC), and increasing expression of membrane-associated mucins (MUC1, MUC4, MUC16)1). The Dry Eye Clinical Practice Guidelines indicate that diquafosol sodium ophthalmic solution improves tear film stability, corneal and conjunctival epithelial damage, and subjective symptoms1).
2% Rebamipide suspension ophthalmic solution (Mucosta®) is used 4 times daily and has actions of promoting secretory mucin secretion by increasing the number of conjunctival goblet cells and increasing membrane-associated mucin expression1). The guidelines indicate that it improves corneal and conjunctival epithelial damage and subjective symptoms1).
Punctal plugs significantly improve tear film stability, corneal and conjunctival epithelial damage, and subjective symptoms1). In tear-deficient types such as area break, punctal plugs are the first-line treatment.
0.1% Sodium hyaluronate ophthalmic solution improves corneal and conjunctival epithelial damage and subjective symptoms1), and artificial tears are useful for improving subjective symptoms1). These can be used as tear replacement for a wide range of subtypes.
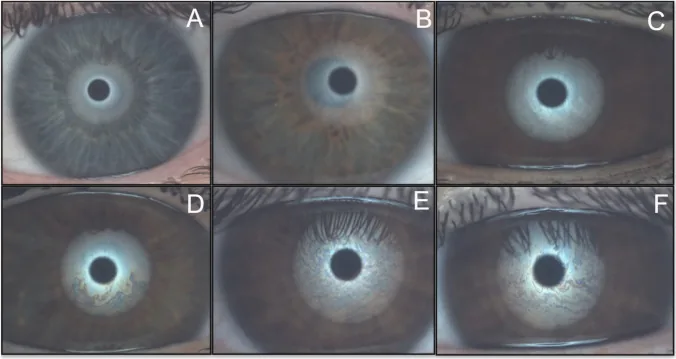
Silva-Viguera MC, et al. Tear film layers and meibomian gland assessment in patients with type 1 diabetes mellitus using a noninvasive ocular surface analyzer. Graefes Arch Clin Exp Ophthalmol. 2023;261(5):1483-1492. Figure 2. PMCID: PMC10148784. License: CC BY 4.0.
Six-grade interference fringe pattern of tear lipid layer captured by ocular surface analyzer (OSA) (A: <15 nm to F: 80–120 nm), showing quantitative assessment of lipid layer thickness based on Guillon classification. This corresponds to non-invasive tear film break-up time (NIBUT) and tear lipid layer interference images discussed in section “6. Measurement Principles and Related Tests.”
The tear film has a three-layer structure: lipid layer, aqueous layer, and mucin layer. The lipid layer consists of lipids secreted by meibomian glands and suppresses tear evaporation. The aqueous layer is composed of aqueous components secreted by the main and accessory lacrimal glands. The mucin layer is composed of secretory mucin secreted by goblet cells and membrane-associated mucin of the corneal epithelium, and is responsible for the wettability of the corneal surface.
BUT reflects the stability time from tear film formation after a blink to its breakup. Abnormality in any of the lipid, aqueous, or mucin layers reduces tear film stability and leads to shortened BUT. Based on this principle, observing the breakup pattern can identify the deficient layer.
As core mechanisms of dry eye, there are two mechanisms: “decreased tear film stability during eyelid opening” and “increased friction during blinking”1). BUT is an index that quantitatively evaluates “decreased tear film stability” among these, and is relatively sensitive.
Non-invasive tear film break-up time (NIBUT) is an alternative measurement method that does not use fluorescein. It detects deformation of the projected image from a keratometer or videokeratography (e.g., Keratograph 5M) to determine tear film disruption. It can be measured without affecting tear volume due to fluorescein instillation, making it suitable for evaluating tear film stability under natural conditions.
According to TFOS DEWS III, NIBUT is positioned as an indicator to be used complementarily with fluoresceinBUT, and is useful as a diagnostic aid 2). Using both fluoresceinBUT and NIBUT improves the accuracy of tear film evaluation.
BUT ≤5 seconds (Japan) NIBUT <10 seconds (DEWS II)
NIBUT <10 seconds
The Schirmer I test evaluates tear secretion and, when combined with BUT, helps differentiate between aqueous-deficient and BUT-shortened dry eye. Although Schirmer values were excluded from the diagnostic criteria in the 2016 version, they remain useful as reference indicators for disease assessment.
Automated NIBUT measurement system: The accuracy of automated analysis of NIBUT using videokeratography is improving. Large-scale studies on the correlation with fluoresceinBUT are ongoing2), and non-invasive BUT measurement may become standardized in the future.
Objective quantification of breakup patterns: Pattern classification based on TFOD currently relies on observer judgment. Development of objective and quantitative pattern classification systems using AI analysis and video analysis is progressing.
Development of “friction enhancement” assessment method: Dry eye involves two mechanisms: “decreased tear film stability” and “increased friction during blinking”1), but a quantitative assessment method for friction enhancement has not been established. Research on quantifying ocular surface friction is being conducted domestically and internationally, and it is expected to be established as a new diagnostic indicator.
Elucidation of the pathophysiology of BUT-shortened dry eye: Research is progressing on the relationship between membrane-type mucin abnormalities and decreased tear film stability, as well as the relationship between changes in corneal sensation (hypersensitivity or hypoesthesia) and dry eye subtypes1).
BUT evaluation in low-humidity and VDT environments: Studies on the association between decreased blinking and shortened BUT in digital device users are accumulating2), and updates to diagnostic criteria considering environmental factors are being considered.