Visual acuity refers to the ability of the eye to discriminate two points, usually expressed as the threshold at which two points or two lines can be seen as separate (minimum separable). It is included in form sense among visual functions (light sense, color sense, form sense, visual field, stereopsis), and visual acuity testing is one of the most important visual function tests.
Visual acuity testing is frequently used as the “entry” examination in ophthalmology. This is because the absence of major abnormalities from the ocular surface to the posterior segment, fovea, and optic nerve is necessary for normal visual acuity. Visual acuity also serves as a criterion for surgical qualification and social security benefits, giving it significant social importance.
Regarding the history of optotypes, the Landolt C was adopted as the international standard optotype at the International Ophthalmological Congress in 1909 1). Currently, JIS T 7309:2002 (based on ISO 8596:2017) specifies the standards for visual acuity testing devices 1).
The rate of spectacle use among adults is as high as 74.2% (including constant use, occasional use, and switching with contact lenses). Refractive error is considered a disease, and refractive correction is positioned as a medical treatment 1). Visual acuity declines with age, starting around age 45, and at age 80, visual acuity is approximately 0.7 to 0.8.
QWhat does visual acuity of 1.0 mean?
A
Visual acuity of 1.0 means that the direction of the gap in a Landolt C (outer diameter 7.5 mm, gap width 1.5 mm) placed at 5 meters can be identified. At this distance, the visual angle of the gap is exactly 1 minute (1/60 degree). Decimal visual acuity is defined as the reciprocal of the minimum angle of resolution (in minutes), and visual acuity 1.0 corresponds to a minimum angle of resolution of 1 minute.
Uncorrected Visual Acuity and Corrected Visual Acuity
The best visual acuity achieved with full correction of refractive error using glasses or contact lenses is called corrected visual acuity. Without correction, it is called uncorrected visual acuity. In ophthalmology, “visual acuity” usually refers to corrected visual acuity. When both uncorrected and corrected visual acuity are recorded, the corrected visual acuity is written in parentheses (e.g., 0.3 (1.2)). If the patient is using intraocular lenses or contact lenses, this should be specified.
Distance Visual Acuity and Near Visual Acuity
Visual acuity at a distance is called distance visual acuity, and at a near distance, near visual acuity. The testing distance for distance visual acuity is 5 m (standard), and for near visual acuity, it is 30 cm. In other countries, 6 m or 20 feet is used for distance, and 40 cm or 14 inches for near, expressed as fractional visual acuity (Snellen fraction).
Single Optotype Visual Acuity and Linear Optotype Visual Acuity
Visual acuity measured by presenting one optotype at a time is called single optotype visual acuity, while visual acuity measured with a standard chart containing multiple optotypes arranged in lines is called linear optotype visual acuity. In children, linear optotype visual acuity is often worse than single optotype visual acuity, a phenomenon known as crowding. In amblyopia, linear optotype visual acuity is also often worse.
Monocular Visual Acuity and Binocular Visual Acuity
Visual acuity measured with one eye covered is called monocular visual acuity, and visual acuity measured with both eyes open without covering is called binocular visual acuity. Generally, binocular visual acuity is about 10% better than monocular visual acuity. In latent nystagmus, covering one eye induces nystagmus, so binocular visual acuity is better.
Relationship between decimal and fractional visual acuity: 20/20 = 6/6 = decimal 1.0. logMAR visual acuity is log(minimum angle of resolution); logMAR 0.00 corresponds to decimal 1.0, logMAR 0.30 to decimal 0.5, and logMAR 1.00 to decimal 0.1.
The ETDRS chart is an international standard chart measured at a testing distance of 4 m, with 0.1 logMAR steps per line and 5 letters per line. The logMAR value is calculated from the number of readable letters with a weight of 0.02 per letter. For low vision patients, the distance is reduced to 3.2 m, 2.5 m, 2.0 m, and 1.0 m, and 0.1, 0.2, 0.3, and 0.6 are added to the logMAR value respectively for correction.
QWhat is the difference between decimal visual acuity and logMAR?
A
Decimal visual acuity is a notation widely used in daily clinical practice and is defined as the reciprocal of the minimum angle of resolution. logMAR visual acuity is the logarithmic value of the minimum angle of resolution and is standardly used in international clinical research and paper reports. logMAR 0.00 = decimal visual acuity 1.0, logMAR 0.30 ≈ decimal visual acuity 0.5, logMAR 1.00 = decimal visual acuity 0.1. logMAR visual acuity has an equal-interval scale, making it suitable for statistical processing.
Refractive errors (myopia, hyperopia, astigmatism), higher-order aberrations, diffraction, and scattering are major causes of decreased visual acuity. Optical abnormalities of the cornea and lens can be corrected with refractive correction, but higher-order aberrations cannot be corrected with ordinary glasses.
Pupil Diameter
The optimal pupil diameter is approximately 2.4 mm. Below 2–3 mm, the effect of diffraction increases and visual acuity decreases. Above 5 mm, aberrations increase and visual acuity decreases. Pupil dilation in dark conditions leads to decreased night vision due to increased aberrations.
Luminance
Visual acuity increases in an S-shaped curve relative to the logarithm of luminance. It decreases when luminance exceeds 5,000–10,000 rlx. In visual acuity testing, measurement within the specified luminance range (80–320 cd/m²) is essential for accuracy.
Aging
Visual acuity begins to decline around age 45. This is due to an increase in higher-order aberrations and a decline in retinal and cerebral transmission system function. Age-related diseases such as cataracts, age-related macular degeneration, and glaucoma are also involved.
Anatomical Limits of Photoreceptors
The diameter of foveal cones is 1–1.5 μm, allowing discrimination of visual angles of 0.21–0.31 minutes. In the fovea, each cone is connected in a one-to-one manner (private pathway) to bipolar cells, ganglion cells, and brain cells, achieving high spatial resolution.
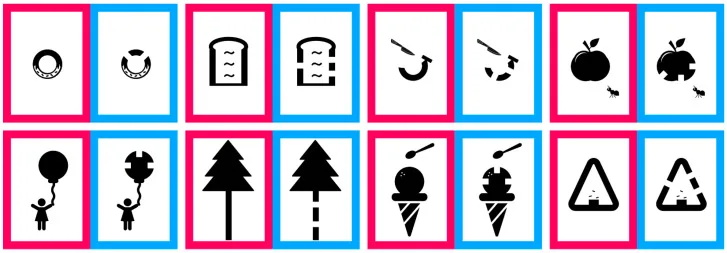
Iwata Y. Investigation of the Visual Acuity Test Success Rate of a New Child-Friendly Minimum-Separable Chart for 2- and 3-Year-Old Children. Vision (Basel). 2025;9(4):100. Figure 2. PMID: 41441558; PMCID: PMC12737760; DOI: 10.3390/vision9040100. License: CC BY.
Optotypes of the minimum separable chart developed for pediatric visual acuity testing. Corresponds to the types of visual targets used in pediatric visual acuity testing discussed in section “4. Examination Methods and Procedures.”
Visual acuity testing devices are classified into three types1). Standard visual acuity testing devices use the 8-direction Landolt C for distance vision and have accuracy compliant with JIS standards (JIS T 7309). Quasi-standard visual acuity testing devices combine the Landolt C with other optotypes, emphasizing practicality. Special visual acuity testing devices include near vision testers and single optotype testers.
The dimensions of the Landolt C, the standard optotype for visual acuity measurement, are specified as follows:
Item
Standard Value
Outer diameter
7.5 mm
Line width
1.5 mm
Gap width
1.5 mm
Gap visual angle at 5 m
1 minute (= decimal visual acuity 1.0)
Visual acuity chart luminance
80–320 cd/m² (recommended 200 cd/m²)
Contrast
74% or more (Michelson formula)
Room illuminance
50 lx or more (not exceeding optotype luminance)
When space is limited, a device equivalent to 5 m at a viewing distance of 0.9 m can be used. It is desirable not to place bright light sources within a 10° visual field diameter in the examination room1).
Step 1 Preparation: Ensure a testing distance of 5 m and set luminance and illuminance to specified values.
Step 2 Occlude one eye: Cover the opposite eye accurately with an occluder. Be careful not to apply pressure.
Step 3 Present optotypes: Present optotypes in order from smallest (or largest). Use an arrangement that includes about 50% horizontal and vertical gaps1).
Step 4 Judgment: Have the patient indicate the direction of the gap (4 or 8 directions). The criterion is 2 out of 2, 2 out of 3, or 3 out of 5 correct answers1). The smallest optotype read without error is recorded as the visual acuity value.
Step 5: Corrected visual acuity measurement: After measuring uncorrected visual acuity, measure corrected visual acuity with glasses or contact lenses.
Visual acuity testing in children and special situations
Infants (3 months and older): Observation of fixation and pursuit (using a penlight or target).
Toddlers: Use single Landolt C ring with hand gesture indication, or dot card/stripe visual acuity test.
Up to middle elementary school: Single optotype visual acuity is standard. If reading a line of optotypes is difficult, use single optotype visual acuity as a substitute.
Upper elementary school and older: Standard line visual acuity test.
Low vision patients: Measure in order: light perception, hand motion, counting fingers. Use ETDRS chart with adjusted distance.
QWhat is suspected when corrected visual acuity is 0.7 or less?
A
Corrected visual acuity below 0.7 suggests organic disease. If visual acuity remains below 0.7 even with glasses or contact lenses, it is necessary to investigate organic causes such as cataract, corneal opacity, macular disease, optic nerve disease, or amblyopia. On the other hand, if only uncorrected visual acuity is reduced and corrected visual acuity is normal, refractive error (myopia, hyperopia, astigmatism) is the cause, and correction with glasses or contact lenses is indicated.
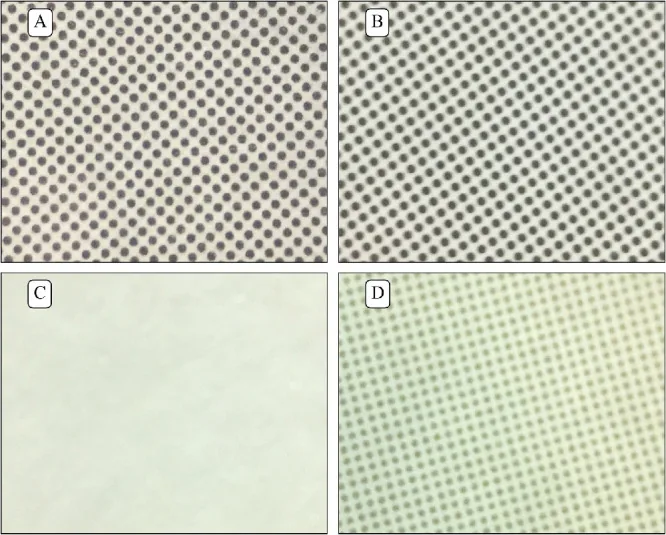
Vivas-Mateos G, Livingstone IAT, Hamilton R, et al. Too Many Shades of Grey: Photometrically and Spectrally Mismatched Targets and Backgrounds in Printed Acuity Tests for Infants and Young Children. Transl Vis Sci Technol. 2020;9(12):12. Figure 4. PMID: 33240565; PMCID: PMC7671855; DOI: 10.1167/tvst.9.12.12. License: CC BY.
(A) Teller Acuity Cards (TAC), (B) Keeler Acuity Cards for Infants (KACI), (C) Lea Paddles (LP), (D) Cardiff Acuity Cards (CAC) – close-up of background patterns of four printed visual acuity test cards. Corresponds to visual acuity testing using the preferential looking method in infants, discussed in section “4. Examination methods and procedures.”
For a regular driver’s license, binocular corrected visual acuity of 0.7 or higher is required. In school health screenings, a corrected visual acuity below 0.7 warrants a detailed examination. The grade of physical disability certificate is determined based on corrected visual acuity (e.g., Grade 1: binocular visual acuity 0.01 or less).
QCan amblyopia be treated in adulthood?
A
Treatment of amblyopia requires intervention during the visual sensitive period (ages 3 to 8 years). After this period, treatment effectiveness is significantly limited. Adult amblyopia is generally difficult to improve. Therefore, early detection of amblyopia through 3-year-old health checkups and school screenings, and initiation of occlusion therapy and refractive correction within the sensitive period, is important.
A visual angle of 1 minute corresponds to 4.85 μm² on the retinal surface. The diameter of foveal cones is 1 to 1.5 μm, theoretically allowing discrimination of details corresponding to a visual angle of 0.21 to 0.31 minutes. In the fovea, each cone connects in a one-to-one manner to bipolar cells, ganglion cells, and brain cells (line labeled private pathway), enabling anatomical maximum resolution that theoretically exceeds visual acuity of 1.0.
Visual acuity (VA) is defined as the reciprocal of the minimum angle of resolution (MAR) in minutes of arc (VA = 1/MAR). The logarithm of the minimum angle of resolution is called logMAR. The ISO uses an equal-interval scale that divides 1 log unit (between decimal visual acuity 0.1 and 1.0) into 10 equal steps (each step is the 10th root of 10 = 1.259).
The ETDRS chart implements this principle, with each line corresponding to a 0.1 logMAR step and 5 letters per line, enabling precise visual acuity assessment.
Visual acuity is obtained only when the entire visual pathway from the ocular optical system → retina (photoreceptors) → optic nerve → optic chiasm → optic tract → lateral geniculate nucleus → optic radiation → primary visual cortex (V1) in the occipital lobe is normal. Damage anywhere in the visual pathway reduces visual acuity.
With the widespread use of digital devices, visual stress and the importance of quality of vision are increasing1). It is important to comprehensively evaluate not only simple visual acuity but also contrast sensitivity, glare visual acuity, and retinal image quality (quality of vision).
Electronic visual acuity charts (auto-charts, tablet-based testing devices) reduce examiner-dependent variability and enable objective measurements. Automation allows efficient testing of many subjects.
Binocular open-field visual acuity testing (polarization method) measures each eye’s visual acuity under natural binocular conditions without an occluder, and is useful for patients with latent nystagmus or children who dislike occlusion.
Contrast sensitivity testing is useful for evaluating patients who complain of “difficulty seeing” despite normal visual acuity (e.g., cataract, optic nerve disease, after refractive correction) and complements standard visual acuity testing.
The WHO classification of visual impairment defines corrected visual acuity less than 0.3 as moderate visual impairment, less than 0.1 as severe visual impairment, and less than 0.05 as blindness, used for international assessment and comparison of disease burden.
Birch EE, Hudgins LA, Jost RM, Cheng-Patel CS, Morale SE, Kelly KR. Web-based visual acuity testing for children. J AAPOS. 2022;26(2):61.e1-61.e5. PMID: 34920136.
Painter SL, Hamilton R, Livingstone IAT. Diagnostic Accuracy of Online Visual Acuity Testing of Paediatric Patients. Br Ir Orthopt J. 2023;19(1):35-43. PMID: 37124456.
Copy the article text and paste it into your preferred AI assistant.
Article copied to clipboard
Open an AI assistant below and paste the copied text into the chat box.