Astigmatism is a refractive condition in which the refractive surface of the eye is not spherical, and the refractive power differs depending on the meridian direction, so that light from a single point in the outside world does not focus at a single point inside the eye. It shows the strongest refractive power (strong principal meridian) in one meridian and the weakest refractive power (weak principal meridian) in the perpendicular direction.
Total astigmatism of the ocular optical system is the sum of corneal astigmatism and lenticular astigmatism. Most is corneal astigmatism. In cases of lens subluxation, lenticular astigmatism becomes stronger.
Classification by astigmatic axis (classified by the direction of the principal meridians):
Classification
Direction of the steeper principal meridian
Characteristics
With-the-rule astigmatism (WTR)
Vertical direction (60–120 degrees)
Most common type of astigmatism. Common in young people.
Against-the-rule astigmatism (ATR)
Horizontal direction (0–30 degrees, 150–180 degrees)
Increases with age.
Oblique astigmatism
Oblique direction (31–59 degrees, 121–149 degrees)
Directions other than horizontal and vertical.
Classification by refractive status:
Classification
Definition
Simple myopic astigmatism
One focal line on the retina, the other in front of the retina
Simple hyperopic astigmatism
One focal line on the retina, the other behind the retina
Compound myopic astigmatism
Both focal lines in front of the retina
Compound hyperopic astigmatism
Both focal lines behind the retina
Mixed astigmatism
One focal line in front of the retina, the other behind the retina
Classification by etiology:
Classification
Definition
Regular astigmatism
Two principal meridians are perpendicular (90 degrees), and refraction is uniform along each meridian. Correctable with cylindrical lenses.
Irregular astigmatism
The two principal meridians are not perpendicular, or refraction is not constant even along the same meridian. Cannot be corrected with cylindrical lenses. Corrected with hard contact lenses.
A systematic review of patients undergoing cataract surgery found that 47% of eyes had pre-existing corneal astigmatism of 1.0 D or more. Approximately one-third of cases have preoperative corneal astigmatism of 1.0 D or greater, making them good candidates for astigmatism correction with toric intraocular lenses. With aging, there is a shift from with-the-rule to against-the-rule astigmatism, so elderly patients undergoing cataract surgery tend to have a higher proportion of against-the-rule astigmatism.
Astigmatism is also important as a cause of anisometropic amblyopia. An astigmatic difference (astigmatic anisometropia) of 1.5 D or more, or binocular astigmatism of 2.0 D or more, significantly increases the risk of amblyopia7). In children, early full correction with glasses for astigmatism over 2 D is effective in preventing meridional amblyopia7).
The prevalence of astigmatism is also high among patients undergoing refractive surgery. In SMILE surgery candidates, the average astigmatic power is about 1–2 D, and accurate setting of the astigmatic correction axis is important in surgical planning 2).
QWhat is the difference between regular and irregular astigmatism?
A
In regular astigmatism, the two principal meridians are perpendicular (90 degrees) to each other, and refraction is uniform along each principal meridian. It can be corrected with cylindrical lenses. In irregular astigmatism, refraction is irregular on the refractive surface; the principal meridians are not perpendicular, or refraction is not constant even along the same meridian. It cannot be corrected with cylindrical lenses; correction is achieved by creating a uniform refractive surface on the anterior cornea with hard contact lenses. Main causes include keratoconus, corneal scars, pterygium, and post-corneal surgery.
Subjective symptoms of astigmatism vary depending on the degree.
Degree
Main Symptoms
Mild (less than 1 D)
Asymptomatic or mild eye strain
Moderate (1–3 D)
Blurred vision, eye strain, headache. Lines in a specific direction appear darker on the astigmatism chart.
High (≥3 D)
Marked visual impairment. In children, risk of meridional amblyopia.
The main complaints are eye strain, headache, and eye pain during near work. In particular, hyperopic astigmatism causes significant eye strain due to accommodative load. Irregular astigmatism cannot be fully corrected with cylindrical lenses, requiring hard contact lenses (HCLs) for correction.
With-the-rule astigmatism (WTR): The steep meridian is vertical. Common in young people and the most frequent type.
Against-the-rule astigmatism (ATR): The steep meridian is horizontal. Increases with age and is common in elderly cataract patients.
Oblique astigmatism: The steep meridian is oblique. Located more than 30 degrees away from 0° or 90°.
Posterior corneal astigmatism (PCA): Average 0.3 D. The steep meridian is often vertical; in WTR eyes, PCA partially cancels anterior astigmatism. In ATR eyes, PCA tends to add to anterior astigmatism5).
Findings in Irregular Astigmatism
Irregular pattern: The two principal meridians are not orthogonal (not 90° apart).
Most corneal astigmatism is due to congenital asymmetry of the corneal shape. Corneal astigmatism accounts for the majority of total ocular astigmatism.
Aging and changes in astigmatism
With-the-rule (WTR) astigmatism is common in young to middle-aged individuals, but a shift to against-the-rule (ATR) astigmatism occurs with aging 5). This is thought to be due to age-related hardening of the peripheral lens and the effect of eyelid pressure, which alter the corneal meridian direction. In elderly patients undergoing cataract surgery, ATR astigmatism is relatively more common.
Causes of irregular astigmatism
Irregular astigmatism can result from keratoconus, corneal scars (post-infection or trauma), pterygium, post-corneal surgery, and ocular surface diseases (dry eye, allergies). It is difficult to diagnose without a corneal topography device, and corneal topography is essential for evaluating the presence of irregular astigmatism.
Causes of postoperative astigmatism
Postoperative astigmatism occurs after cataract surgery and corneal transplantation. Contributing factors include limbal relaxing incisions (LRI), femtosecond laser arcuate keratotomy (FLACS-AK), and suture-induced astigmatism. Astigmatism after extracapsular cataract extraction with sutures may be reduced by suture removal, but note that predictability is low.
Kamari M, et al. Diagnosis of Dry Eye Disease Using Ocular Imaging Techniques. Diagnostics (Basel). 2021;11(8):1466. Figure 1. PMCID: PMC8392046. License: CC BY.
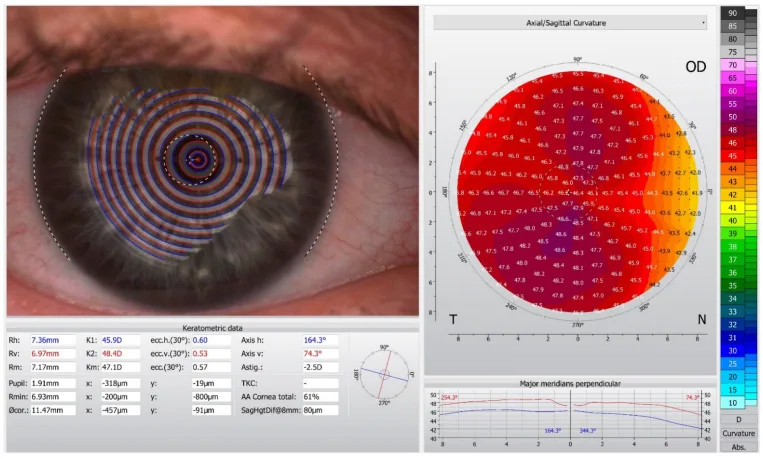
Corneal topography examination with Oculus Keratograph 5M: Left is a captured image of Placido disk concentric rings projected onto the anterior corneal surface; in regular astigmatism, an elliptically deformed ring pattern is observed. Right is a color map of axial (sagittal) curvature, showing a bow-tie pattern with symmetrical distribution of steep and flat meridians. This corresponds to corneal shape analysis (topography) discussed in the section “Diagnosis and Examination Methods.”
Essential for differentiating regular and irregular astigmatism. Confirms presence of irregular astigmatism.
Corneal tomography (Scheimpflug imaging)
Anterior and posterior corneal astigmatism (TCA, 3D)
Recommended for high PCA cases. Provides actual PCA measurements.
Retinoscopy: Objective refraction measurement. Useful for precise examination under mydriasis.
Cross-cylinder method: Subjective examination method used for precise measurement of astigmatism axis and power.
Corneal topography: Essential for evaluating irregular astigmatism. It is difficult to determine the presence of irregular astigmatism without corneal topography. If corneal astigmatism and refractive astigmatism differ significantly, check whether the implanted intraocular lens is properly positioned.
For quantifying astigmatism, in addition to the three elements of spherical power, cylindrical power, and axis, Thibos power vector analysis is also used. This method describes astigmatism using three components: spherical equivalent (M), Jackson cross-cylinder component (J0: vertical-horizontal astigmatism), and Jackson cross-cylinder component (J45: oblique astigmatism), and evaluates changes in astigmatism before and after treatment three-dimensionally 9). Particularly in postoperative evaluation of toric IOLs, vector analysis of residual astigmatism and residual axis is useful for estimating the amount of axis misalignment and planning reoperation.
The Alpins method is a statistical analysis method used to evaluate before and after astigmatism correction surgeries such as toric IOL, LASIK, and LRI. It consists of three vectors: target induced astigmatism (TIA), surgically induced astigmatism (SIA), and difference vector (DV), and can calculate correction index, error index, success index, etc. 9). In postoperative evaluation, it is characterized by enabling comprehensive assessment including changes in axis, not just simple comparison of astigmatism power.
After cataract surgery, since the crystalline lens has been removed, most postoperative astigmatism is corneal astigmatism. It is important not to judge solely based on autokeratometer readings but to use corneal topography to confirm the presence or absence of irregular astigmatism 6). The adult cataract PPP sets the target for residual postoperative astigmatism at 0.5 D or less 6).
Flow of postoperative astigmatism evaluation (based on adult cataract PPP)
Provisional refraction assessment (prescription may be deferred due to instability)
3 months post-op
Evaluate residual astigmatism after stabilization. Consider spectacle prescription or additional treatment
Residual astigmatism ≥0.75 D
Assess patient symptoms; consider spectacle prescription or additional laser correction
In procedures involving corneal sutures (e.g., extracapsular cataract extraction), astigmatism may be reduced by suture removal. Although suture-related astigmatism is less common after modern phacoemulsification, appropriate incision size, location, and wound closure are fundamental to minimizing postoperative astigmatism6).
Preoperatively, reference markings are placed at the corneal limbus, and the toric IOL axis is accurately aligned during surgery. Digital eye rotation tracking systems and intraoperative aberrometry contribute to improved axis marking accuracy8).
Procedure for postoperative astigmatism evaluation
Three months or more after cataract surgery, the following should be confirmed6):
Subjective and objective refraction (check amount and axis of residual astigmatism)
Corneal topography (evaluate anterior/posterior astigmatism and total corneal astigmatism)
Slit-lamp illumination and anterior segment OCT are useful for detecting IOL axis misalignment after toric IOL implantation. Early postoperative confirmation (within 1 week) yields higher success rates for rotational correction; after 3 months, capsular fibrosis may make repositioning difficult 4).
QWhy is corneal topography important?
A
Corneal topography is essential for detecting irregular astigmatism and differentiating it from regular astigmatism. Toric IOLs correct only regular astigmatism; irregular astigmatism is a contraindication. In cases with high posterior corneal astigmatism (PCA ≥0.5D), considering total corneal astigmatism (TCA) in IOL calculation improves accuracy, and Scheimpflug imaging for posterior corneal assessment is recommended 5).
Most common. Unsuitable for irregular astigmatism. Beware of meridional aniseikonia.
Soft contact lenses (toric SCL)
Regular astigmatism (mild to moderate)
Convenient. Rotational stability is a challenge.
Hard contact lenses (RGP)
Irregular astigmatism, high regular astigmatism
Forms a uniform refractive surface on the anterior cornea. Mainstay for correcting irregular astigmatism in keratoconus.
Scleral lenses (scleral CL)
High irregular astigmatism (e.g., end-stage keratoconus)
Supported by the sclera, so minimal corneal contact. Excellent for correcting irregular astigmatism.
In children, astigmatism of 2D or more poses a risk of amblyopia (meridional amblyopia), and early full correction with constant spectacle wear is important 7). If aniseikonia is a concern, consider reducing cylinder power or shifting the axis (within 15 degrees).
Astigmatism correction via refractive surgery may weaken over the long term. Especially in cases of against-the-rule astigmatism, age-related progression toward against-the-rule may occur, and reoperation may be considered. In LASIK, attention to residual corneal thickness is necessary.
The evidence-based guidelines for corneal refractive surgery (SMILE) indicate that spherical equivalent up to 10D (myopia up to 10D, astigmatism up to 3D) is suitable 2). LASIK and PRK are indicated for both myopic and hyperopic astigmatism, but regression risk is greater for hyperopic correction than for myopic correction 1). Five-year results of femtosecond laser arcuate keratotomy (FLACS-AK) show that mean preoperative astigmatism of 1.63 D significantly decreased to 0.53 D postoperatively and remained stable at 0.55 D after 5 years 3).
SMILE (small incision lenticule extraction) is actively used for myopic astigmatism. The KLEx (keratorefractive lenticule extraction) guidelines recommend a maximum astigmatism correction of 3D, with a design emphasizing residual corneal thickness of at least 250 μm and the sum of flap thickness plus residual stromal bed 2). Compared to LASIK, flap complications are avoided, and it is considered superior in terms of corneal nerve preservation and biomechanical stability, but surgeon experience is required for accurate astigmatic axis setting.
LASIK for hyperopic astigmatism
Hyperopic LASIK has a higher regression rate than myopic correction, and long-term results are unstable for hyperopia of +4D or more. Surgery for hyperopic astigmatism (compound hyperopic astigmatism and mixed astigmatism) requires confirmation of regular astigmatism and thorough preoperative corneal topography evaluation 1).
Cataract surgery is also an opportunity to insert an intraocular lens (IOL), allowing astigmatism correction without additional invasiveness. The target for postoperative residual astigmatism is 0.5 D or less.
The cylindrical power at the IOL plane corresponds to 1.5–6.0 D, enabling correction of 0.75–4.75 D of corneal astigmatism. It should be considered for regular astigmatism of 1.0 D or more, and strong evidence supports its use for astigmatism over 2.0 D4).
A meta-analysis (13 trials) showed that toric IOLs significantly improve postoperative uncorrected distance visual acuity (UDVA) compared to non-toric IOLs (mean difference -0.07 logMAR, 95% CI -0.10 to -0.04) and reduce the risk of not achieving 20/25 or better4).
Effect of axis misalignment: A 1-degree misalignment reduces the corrective effect by approximately 3.3%. A 30-degree misalignment nearly eliminates the corrective effect, and beyond that, postoperative visual function may be worse than with a non-toric IOL.
Contraindications for toric IOL: Irregular astigmatism (keratoconus, corneal scar, corneal ectasia), zonular weakness or rupture, posterior capsule rupture, poor pupil dilation, severe dry eye, history of vitreoretinal surgery with buckling or glaucoma implant.
FLACS-AK (Femtosecond laser arcuate keratotomy)
Because the laser incision design is based on anterior segment OCT measurements, it offers higher incision accuracy and depth uniformity than manual incisions.
Pham et al. (2025) conducted a 5-year follow-up cohort study of 34 eyes and showed that simultaneous FLACS-AK and cataract surgery significantly reduced mean preoperative corneal astigmatism from 1.63±0.886 D to 0.53±0.628 D at 3 months postoperatively (p=0.001), and remained stable at 5 years (0.55±0.624 D)3). The rate of achieving UDVA 20/25 or better was 67.6% and remained unchanged for 5 years, and the proportion of eyes with MRSE within ±0.50 D reached 91.2% at 5 years3).
QWhat happens if the toric IOL axis is misaligned?
A
A 1-degree axis misalignment reduces the corrective effect by approximately 3.3%, and a 30-degree misalignment almost eliminates the effect. With a large misalignment of 30 degrees or more, postoperative visual function may be worse than with a non-toric IOL. IOL rotation tends to occur early, from 1 hour to the next day after surgery, so stable in-the-bag fixation at the end of surgery is important. In eyes with long axial length, the IOL power is low and the optic is thin, making rotation more likely; concurrent insertion of a capsular tension ring (CTR) has been reported to be effective. If axis misalignment is confirmed, early repositioning surgery should be considered.
Light incident on an astigmatic eye forms an anterior focal line in the direction of the steep meridian and a posterior focal line further posteriorly in the direction of the flat meridian. Between these two focal lines, a circle of least confusion is formed (Sturm’s conoid). The spherical equivalent is the average refractive value of the steep and flat meridians and corresponds to the refractive state at the position of the circle of least confusion.
Total astigmatism of the ocular optical system is the sum of corneal astigmatism and lenticular astigmatism. Most is accounted for by corneal astigmatism, but lenticular astigmatism becomes stronger when there is lens subluxation. Since lenticular astigmatism disappears after cataract extraction, postoperative astigmatism is essentially only corneal astigmatism.
The posterior cornea has negative refractive power, and its steep meridian is vertically oriented in most eyes. Therefore, PCA often acts in the opposite direction to anterior corneal astigmatism. In with-the-rule (WTR) astigmatism, PCA partially cancels anterior astigmatism; in against-the-rule (ATR) astigmatism, PCA adds to anterior astigmatism.
Jin et al. (2023) reported in a retrospective study of 62 eyes with high PCA (≥0.5 D) that toric IOL calculation using total corneal astigmatism (TCA) resulted in postoperative overcorrection in both the ATR group (correction index 1.14±0.29) and the WTR group (correction index 1.25±0.18) 5). The error magnitude was 0.22±0.52 D (p=0.03) in the ATR group and 0.65±0.60 D (p=0.00) in the WTR group, both significantly shifted toward overcorrection 5). Overcorrection in WTR eyes can cause axis reversal and induce postoperative ATR astigmatism; therefore, TCA-based toric IOL calculation is recommended for ATR eyes, but caution is needed especially in WTR eyes 5).
In young individuals, with-the-rule astigmatism (WTR) is common, but it shifts to against-the-rule astigmatism (ATR) with aging. This is thought to be due to changes in corneal meridian direction caused by hardening of the peripheral lens and eyelid pressure with age. This shift is a factor to consider in toric IOL power calculation and LRI planning.
The speed of the ATR shift in astigmatism accelerates with age and becomes particularly noticeable after the 60s. This shift provides the basis for planning that accounts for future astigmatic changes during IOL calculation (e.g., leaving a slight with-the-rule residual astigmatism) 4). In eyes with long axial length (high myopia), the shift to ATR tends to be faster, and toric IOL calculation in these cases requires more careful evaluation 4).
In astigmatism of 3D or more, meridional amblyopia, in which visual development in the steep meridian is suppressed, may be present. For astigmatism exceeding 2D, full correction on a regular basis is important for visual development. Early detection and early correction can lead to good visual acuity outcomes.
The Amblyopia PPP (2022 revision) recognizes anisometropic astigmatism (strong astigmatism in one eye only) of 1.5D or more as a risk factor for amblyopia, and early detection through refractive screening (photoscreening) is recommended 7). Particularly in oblique astigmatism (axis near 45° or 135°), visual function in peripheral and motion vision is more likely to be reduced compared to central vision.
In cycloplegic refraction for astigmatism, accurate evaluation of cylinder power and axis is essential. If there is a large change in cylinder power or axis before and after atropine instillation, involvement of lenticular astigmatism should be suspected. In aphakic and pseudophakic eyes, corneal astigmatism accounts for almost all astigmatism 6).
Keratoconus is a progressive corneal ectasia that presents with marked irregular astigmatism. Tomography using Scheimpflug imaging (e.g., Pentacam) shows characteristic patterns such as posterior elevation, thinning, and positive Amsler grid. The KLEx (SMILE) guidelines mandate strict preoperative screening, considering suspected keratoconus cases (e.g., posterior maximum elevation ≥16 μm) as contraindications 2).
This is a lens whose refractive power can be fine-tuned postoperatively by ultraviolet irradiation. By confirming residual refraction after surgery and then adjusting the power with light irradiation, improved accuracy of astigmatism correction is expected 4).
This is a system that measures the refractive state of the aphakic or phakic eye in real time during surgery and guides the optimal IOL power and axis. Both IA and the Barrett Toric Calculator achieve residual astigmatism of less than 0.5 D in 75% of eyes, surpassing the 53% of the preoperative calculation group. Real-time correction is expected to reduce the risk of reoperation, but dedicated equipment and additional time are required 4).
Development of personalized IOLs based on detailed preoperative corneal imaging and patient-specific refractive profiles is underway. Approaches to precision medicine that elucidate the genetic background of refractive errors and establish treatment plans according to individual eye characteristics are being explored 4).
Comparison of Astigmatism Correction Outcomes between SMILE and LASIK
The KLEx guidelines include a systematic review comparing astigmatism correction outcomes of SMILE and LASIK 2). The accuracy of astigmatism correction (achievement rate of residual astigmatism within 0.5 D) is reported to be 75–90% for SMILE, which is equivalent to or slightly better than LASIK (70–85%). However, some reports indicate that LASIK is slightly more stable in terms of astigmatism axis predictability.
In SMILE astigmatism correction, axis accuracy management is a challenge; preoperative digital ocular cyclotorsion tracking and intraoperative nomogram adjustment are key to improving accuracy. Since even a slight misalignment of the femtosecond laser irradiation position directly leads to residual astigmatism, surgical experience and technical proficiency are essential 2).
Long-term Management after Astigmatism Correction Surgery
Long-term outcomes after astigmatism correction surgery (LASIK, SMILE, toric IOL) may involve the following issues:
Regression: Particularly noticeable after hyperopic astigmatism correction with LASIK. Age-related ATR shift may compound the deficiency in correction amount.
IOL axis rotation: Axis stabilization continues within the first year after toric IOL implantation. Late rotation due to capsular contraction has also been reported 4).
Corneal ectasia: Occurs when the residual stromal bed is too thin after LASIK or PRK. Early detection and CXL intervention affect prognosis.
To minimize these complications, preoperative screening (including corneal topography with pachymetry and calculation of residual stromal bed) and long-term postoperative follow-up are essential 1).
Wang Y, Xie L, Yao K, et al. Evidence-based guidelines for keratorefractive lenticule extraction surgery. Ophthalmology. 2025;132(4):397-419. doi:10.1016/j.ophtha.2024.11.016. PMID:39577672.
Pham TMK, Nguyen XH, Pham TTT, Hoang TT. Five Years Follow-Up Outcomes of Femtosecond Laser-Assisted Cataract Surgery on Patients with Preexisting Corneal Astigmatism. International medical case reports journal. 2025;18:373-379. doi:10.2147/IMCRJ.S506198. PMID:40129561; PMCID:PMC11932028.
Jin T, Yu L, Li J, Zhou Y. Refractive outcomes of toric intra-ocular lens implantation in cases of high posterior corneal astigmatism. Indian J Ophthalmol. 2023;71(8):2967-71. doi:10.4103/IJO.IJO_3385_22
Miller KM, Oetting TA, Tweeten JP, Carter K, Lee BS, Lin S, et al. Cataract in the Adult Eye Preferred Practice Pattern. Ophthalmology. 2022;129(1):P1-P126. doi:10.1016/j.ophtha.2021.10.006. PMID:34780842.
American Academy of Ophthalmology. Amblyopia Preferred Practice Pattern 2022 Update. Ophthalmology. 2023;130(3):P136-P178.
Kamari M, et al. Diagnosis of Dry Eye Disease Using Ocular Imaging Techniques. Diagnostics (Basel). 2021;11(8):1466.
Kanclerz P, Przewłócka K, Arnold RW. Agreement in non-cycloplegic and cycloplegic refraction between a photoscreener and a calibrated autorefractor. BMC Ophthalmol. 2024;24(1):130. doi:10.1186/s12886-024-03375-z. PMID:38528448; PMCID:PMC10962162.
Copy the article text and paste it into your preferred AI assistant.
Article copied to clipboard
Open an AI assistant below and paste the copied text into the chat box.