Aniseikonia is a condition in which the size or shape of the image seen by each eye differs when viewing an object with both eyes.
The image perceived in visual space is primarily determined by the retinal image formed on the retina, which is influenced by complex refractive factors such as the refractive power of each surface of the cornea and lens, anterior chamber depth, and nodal point position, as well as axial length. This image, influenced by anatomical factors such as the number of photoreceptors distributed in the retinal area onto which the image is projected, and complex neural mechanisms including convergence, is perceived in the visual cortex and understood as an ocular image projected into visual space.
It has been traditionally said that aniseikonia exceeding 5% causes disturbances in binocular fusion, leading to asthenopia, and if it becomes stronger, stereopsis is disrupted 5). When binocular visual function is impaired, it can cause asthenopia and headache.
Aniseikonia rarely occurs alone; it often accompanies anisometropia (difference in refractive power between the two eyes). It is particularly problematic in the following situations:
After unilateral cataract surgery: A typical condition causing high refractive anisometropia
After treatment for anisometropic amblyopia: Aniseikonia becomes apparent when wearing fully corrective glasses
After refractive surgery: When a refractive difference between the eyes occurs
After intraocular lens implantation: Postoperative refractive difference causes aniseikonia
Since spectacle lenses are usually placed 12 mm in front of the corneal apex, magnification effects occur. When attempting to fully correct different refractive powers (anisometropia) between the eyes, the difference in image size (aniseikonia) seen through the spectacle lenses can cause symptoms such as asthenopia, headache, diplopia, and abnormal spatial perception. However, in children, strong sensory adaptation is observed, so full correction is often possible.
Aniseikonia is expressed as a percentage (%). It is calculated based on the difference in image size (area) seen by both eyes. The difference in the vertical meridian is called vertical aniseikonia, and the difference in the horizontal meridian is called horizontal aniseikonia. It is important to evaluate each meridian direction individually. Isomagnification refers to a uniform magnification difference across all meridians, while meridional aniseikonia refers to a magnification difference occurring only in a specific meridian direction 8).
Spectacle magnification (SM) is expressed as the product of the following two factors 8):
Shape factor: Magnification due to the lens center thickness, refractive index, and front surface curvature radius
Power factor: Magnification due to the vertex distance and back vertex power
By adjusting these two factors, it is possible to design spectacle prescriptions that minimize aniseikonia. Contact lenses have a power factor close to 1, so their effect on image magnification is smaller compared to spectacles 6).
QWhat is the difference between aniseikonia and anisometropia?
A
Anisometropia refers to the difference in refractive power (D) between the two eyes, while aniseikonia refers to the difference in the size or shape of images seen by the two eyes (%). Anisometropia does not always cause aniseikonia; the degree of aniseikonia differs between axial and refractive anisometropia. For example, in axial anisometropia due to differences in axial length, Knapp’s law states that spectacle correction can make image magnification nearly equal. On the other hand, in refractive anisometropia due to differences in corneal or lens power, spectacle correction may actually increase aniseikonia. For spherical lenses, the tolerable range of aniseikonia is said to be 6–8%, and it is desirable that the difference in spherical power between the two eyes does not exceed 1.5 D7).
Aniseikonia often presents with vague subjective symptoms; patients may complain of “eye fatigue” or “headache” rather than “difficulty seeing.” It is not uncommon for aniseikonia to be discovered for the first time during a detailed examination of patients who present with asthenopia as their main complaint.
The main subjective symptoms are as follows.
Asthenopia: Easy fatigability during near work and reading
Headache: Dull pain around the eyes and temporal region
Diplopia and abnormal spatial perception: Occurs in 5–7% or more
Stereopsis impairment: Depth perception is lost in high-degree aniseikonia
Nausea and vomiting: May accompany high-degree aniseikonia
Correction with cylindrical lenses may cause abnormal spatial perception due to meridional aniseikonia. Two types of abnormal spatial perception—floor tilt sensation, object tilt sensation, and spatial distortion—may coexist. Horizontal meridional aniseikonia makes the floor appear tilted, while vertical meridional aniseikonia makes objects or space appear tilted. These are managed by adjusting the cylindrical lens power or axis.
No symptom score specific to aniseikonia has been established, but clinically, multiple symptoms including reading difficulty, loss of stereopsis, and motion sickness-like sensation affect patient QOL. In aniseikonia that develops after cataract surgery, the subjective burden is more easily recognized because pre- and postoperative comparisons are possible 10). Especially in elderly patients, adaptation to prescription changes is slow, and there is a high risk of symptom fixation. Attempts have been made to quantify symptoms using asthenopia scores (e.g., modified Convergence Insufficiency Symptom Survey) 9), but a validated score specific to aniseikonia has not yet been developed.
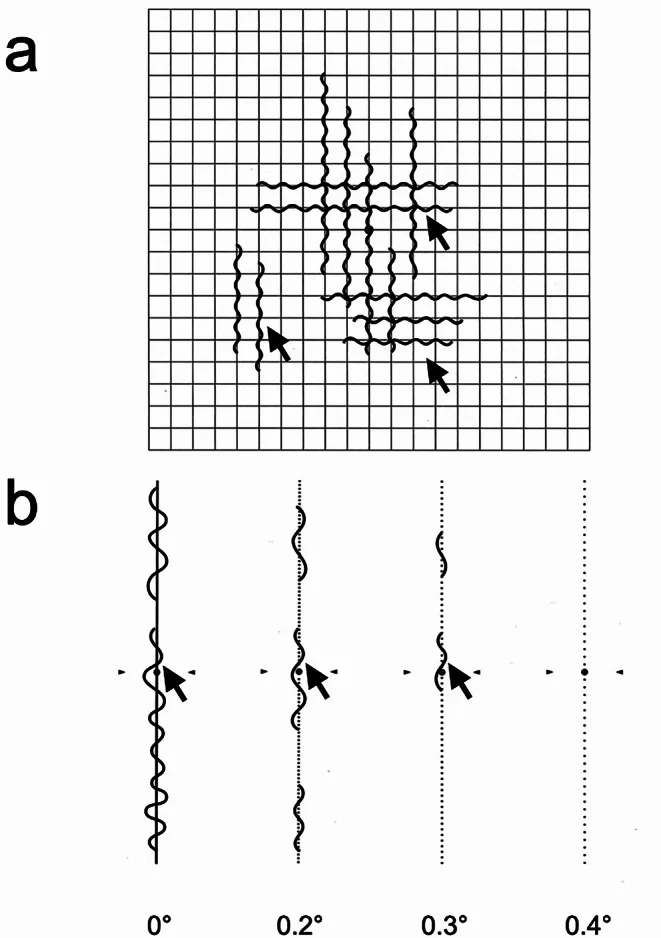
Matoba R, Morizane Y. Epiretinal membrane: an overview and update. Jpn J Ophthalmol. 2024;68(6):603-613. Figure 2. PMCID: PMC11607056. License: CC BY.
Schematic diagram of two examination methods for quantifying metamorphopsia: (A) The Amsler chart consists of a 10 cm square grid; the patient fixates on the center and reports the presence of waviness or distortion—a qualitative test. (B) The M-chart consists of one straight line and 19 dotted lines with dot intervals from 0.2° to 2.0°; the smallest dot interval at which the patient perceives a straight line is recorded as the metamorphopsia score (M-chart score). This corresponds to aniseikonia due to retinal deformation (retinal aniseikonia) caused by epiretinal membrane or macular edema, discussed in the section “Causes and risk factors.”
The causes of aniseikonia are broadly classified into three categories: refractive factors, anatomical factors, and neural mechanisms.
Difference in corneal/lens refractive power: Occurs when the corneal curvature or lens refractive power differs between the two eyes. Typical examples include monocular aphakia, phakic intraocular lens implantation, and post-LASIK.
Magnification difference due to spectacle lenses: The combination of vertex distance (usually 12 mm) and lens power creates a magnification difference. Higher lens power results in greater magnification effect and increased risk of aniseikonia.
Anisometropia of astigmatism: Aniseikonia can also occur when the cylinder power or axis differs between the two eyes. However, if the cylinder power and axis are the same in both eyes, even strong astigmatism can often be fully corrected.
Aniseikonia due to axial factors
Axial length difference (axial anisometropia): In an eye with a longer axial length, the retina is stretched, so the same retinal image covers a larger area of photoreceptors, making the perceived image larger. Conversely, in an eye with a shorter axial length, the image is perceived as smaller.
Application of Knapp’s law: In axial anisometropia, spectacle correction nearly eliminates the magnification difference of retinal images (Knapp’s law). Therefore, axial anisometropia is easier to manage with spectacle correction.
Clinical causes (classification by type of anisometropia)
Data on the exact prevalence of aniseikonia are limited. In adult populations with full spectacle correction, the incidence of clinically significant aniseikonia (generally 3-5% or more) is estimated to be a few percent. Studies on patients after cataract surgery report a significant increase in patients who perceive aniseikonia postoperatively 10), especially when residual anisometropia is large after unilateral surgery. Approximately 80% of patients with epiretinal membrane develop metamorphopsia, a substantial portion of which is accompanied by local aniseikonia 11).
Aniseikonia is likely to become problematic when the refractive difference between the operated eye and the fellow eye exceeds 1.5 D after unilateral cataract surgery. Postoperative axis misalignment of a toric IOL (30 degrees or more) can not only eliminate the correction effect but also increase meridional aniseikonia 1). After refractive surgery (LASIK, SMILE, etc.), aniseikonia may become apparent if there is a difference in the amount of correction between the two eyes or if only one eye is operated on 8).
Diagnosis of aniseikonia requires specialized tests that quantitatively measure the difference in image size between the two eyes. The following four main measurement methods exist.
Test method
Principle/method
Features
Pola test
Separates images for each eye using polarizing filters. Shows U-shaped figures facing each other and compares their sizes.
Simple. Uses polarizing glasses. One step indicates 3.5% aniseikonia; two or more steps interfere with binocular vision.
Measures aniseikonia while also testing simultaneous perception, fusion range, and stereopsis.
Allows comprehensive evaluation of binocular function.
Phase difference haploscope
Projects half-moon images with straight edges facing each other onto a screen in front; compares the sizes of the left and right half-moons.
Precise measurement using half-moon images. Allows evaluation under conditions close to daily vision.
New Aniseikonia Tests
Separates eyes with red-green glasses. Uses half-moon figures No. 0 to 24 (1’ to 24’) to quantitatively measure aniseikonia from 1% to 24% (in No. 1’ to 24’, the green half-moon progressively increases by 1% to 24%).
Wide measurement range (1–24%) and high quantitative accuracy. Widely used in clinical practice.
In principle, aniseikonia measurement should be performed after appropriate refractive correction (glasses or contact lenses). Since the degree of aniseikonia varies with correction, measuring separately with glasses and contact lenses is useful for determining diagnosis and treatment strategy.
Additionally, evaluating binocular function (simultaneous perception, fusion range, stereopsis) together with the diagnosis of aniseikonia allows comprehensive understanding of its relationship with symptoms 5). The phase difference haploscope has the advantage of simultaneously evaluating the angle of strabismus, retinal correspondence, suppression, fusion, stereopsis, and aniseikonia under conditions close to daily vision 5).
The New Aniseikonia Tests are performed in a bright room at a testing distance of 40 cm. After refractive correction, the eye with the greater refractive error wears a red filter, and the eye with the lesser refractive error wears a green filter. The number at which the red and green half-moon figures appear equal in size indicates the percentage of aniseikonia, measurable in 1% increments.
The M-Chart is useful for quantifying local aniseikonia (metamorphopsia) caused by epiretinal membrane or macular degeneration. It consists of 19 dotted lines with dot intervals ranging from 0.2° to 2.0°. The smallest dot interval at which the patient perceives the line as straight is recorded as the metamorphopsia score, providing a quantitative assessment 11). While the Amsler chart is qualitative (determining the presence of waviness or distortion), the M-Chart can quantify scores in both vertical and horizontal directions, making it useful for pre- and postoperative follow-up and evaluation of treatment efficacy.
Calculation of Aniseikonia in Spectacle Lens Design
Predictive calculation of aniseikonia when prescribing spectacles can be performed using the following steps:
Check the correction power, vertex distance, and lens design parameters (front curvature, center thickness, refractive index) for each eye.
Calculate the shape factor and power factor for each eye, and determine the respective magnification.
Calculate the percentage difference in magnification between the two eyes.
If the calculated value exceeds 5%, consider changing the correction method (switching to contact lenses or adjusting vertex distance).
This calculation becomes more complex when using toric lenses, requiring individual calculations for each meridian 8).
QHow is aniseikonia measured?
A
There are four main methods for measuring aniseikonia: (1) Pola test (comparing the size of a U-shaped figure using polarizing filters), (2) Major amblyoscope (simultaneously measuring aniseikonia and evaluating binocular vision), (3) Phase difference haploscope (comparing the size of half-moon images, allowing evaluation close to natural viewing), and (4) New Aniseikonia Tests (quantifying 1–24% in 1% increments using red-green glasses). All methods are based on the principle of optically separating the images of both eyes and comparing their sizes. The New Aniseikonia Tests have a wide measurement range and are most widely used in clinical practice. Since results vary depending on the correction state (spectacles or contact lenses), it is important to measure under each condition.
A radical cure for aniseikonia has not yet been established. The goal of treatment is to keep aniseikonia within the acceptable limit (5% or less) by selecting an appropriate refractive correction method.
An iseikonic lens is a lens that optically corrects aniseikonia by magnifying the image of the smaller eye. However, iseikonic lenses have limitations in magnification and are not commercially available because the lens becomes extremely thick and impractical. Therefore, it is important to minimize aniseikonia or keep it within acceptable limits during refractive correction.
Selection of Correction Method (Optimization According to Type of Anisometropia)
To minimize aniseikonia, it is important to select a correction method according to the type of anisometropia (axial or refractive).
Axial Anisometropia (Mainly Due to Axial Length Difference)
Spectacle correction is advantageous. According to Knapp’s law, placing the correcting lens at the anterior focal point of the eye nearly eliminates the difference in image magnification. Since the vertex distance of spectacles is usually close to the condition of Knapp’s law, aniseikonia can be minimized with spectacle correction in axial anisometropia6).
Refractive Anisometropia (Mainly Due to Difference in Corneal or Lens Refractive Power)
Contact lenses or refractive surgery are advantageous. Contact lenses correct at a position closer to the cornea than the anterior focal point, thus reducing the difference in image magnification compared to spectacles6). In cases of high refractive anisometropia, such as after unilateral cataract surgery, contact lenses are often the first choice.
In cases where aniseikonia is problematic, switching to contact lens correction or prescribing monovision spectacles (determining the power of the fellow eye based on the eye with weaker myopia or stronger hyperopia, leaving the fellow eye myopic) are also options.
Management of Meridional Aniseikonia
When meridional aniseikonia becomes problematic with cylindrical lens correction, the following measures can be taken:
Reduce the cylindrical power (visual acuity may be sacrificed due to increased residual astigmatism).
Shift the cylinder axis to 180 or 90 degrees (preferably within 15 degrees).
Set a shorter vertex distance.
In measures ① and ②, spectacle visual acuity may be sacrificed due to increased residual astigmatism, so adjustments should be made on a case-by-case basis while considering the trade-off between visual acuity and wearing comfort.
Management Protocol for Post-Cataract Surgery Aniseikonia
If postoperative aniseikonia is severe and uncorrectable, consider IOL power change surgery.
To prevent postoperative aniseikonia, preoperative binocular refraction assessment and target refraction setting are important. The adult cataract PPP recommends setting the residual refraction target to match the refraction of the healthy eye during unilateral surgery4).
Currently, there is no treatment that can cure aniseikonia itself. Iselkonic lenses, an optical correction method, are theoretically effective but have not been put into practical use. The goal of treatment is to keep aniseikonia within the tolerable limit (5% or less) by selecting the optimal refractive correction method. For axial anisometropia, spectacle correction is chosen; for refractive anisometropia, contact lenses or refractive surgery are chosen. In many cases, symptoms can be reduced or eliminated. Localized aniseikonia caused by epiretinal membrane or macular disease may not completely disappear even after treatment of the underlying disease.
The root cause of aniseikonia is the difference in size and shape of the retinal image between the two eyes. The factors causing this difference can be categorized as follows.
Refractive Factors
Differences in corneal curvature, refractive power of each lens surface, anterior chamber depth, and nodal point position between the eyes directly affect the magnification of the image formed on the retina. Eyes with stronger refractive power tend to have smaller (minified) retinal images. With spectacle correction, the image magnification changes depending on the relative position of the lens and the eye (vertex distance), so spectacle correction itself can increase or decrease aniseikonia.
Axial Factors (Knapp’s Law)
In eyes with longer axial length, the retina is stretched, so even if the retinal image is the same size, the photoreceptors cover a wider area, making the perceived image larger. Conversely, in eyes with shorter axial length, the image is perceived as smaller.
Knapp’s law is an optical principle stating that when a lens is placed at the anterior focal point of the eye, the magnification effect of the correcting lens becomes zero. Since the position of spectacle lenses approximately satisfies this condition, spectacle correction does not affect the retinal image magnification difference due to axial anisometropia, and aniseikonia caused by axial anisometropia is almost eliminated when wearing spectacles.
Anatomical Factors
The density of retinal photoreceptors is not uniform. Even if the retinal image area is the same, if the number of recruited photoreceptors differs between the eyes, the perceived image size at the visual cortex will differ. Retinal deformation due to epiretinal membrane or macular edema causes local changes in photoreceptor density, leading to localized aniseikonia (metamorphopsia).
Neural Mechanisms
Binocular fusion requires complex information integration in the visual cortex. When the images from the two eyes differ significantly, fusion processing in the cortex fails, resulting in eye strain, diplopia, and impaired stereopsis. Fusion disturbance begins when the difference exceeds 5%, and fusion becomes impossible at 7% or more.
Why Wearing Spectacles for Refractive Anisometropia Worsens Aniseikonia
Contact lenses correct vision at a position closer to the corneal surface than the anterior focal point of the eye. In this case, because the conditions of Knapp’s law are not met, even in refractive anisometropia, there is an effect on image magnification, and aniseikonia can often be reduced compared to spectacles. This is the optical basis for the claim that contact lenses are advantageous for refractive anisometropia.
On the other hand, when contact lenses are used in axial anisometropia, the conditions of Knapp’s law are no longer satisfied, and aniseikonia may increase compared to spectacle wear. Therefore, accurately differentiating between axial and refractive anisometropia is directly linked to selecting the optimal correction method.
In children, sensory adaptation to aniseikonia is more likely to occur during the sensitive period of binocular visual development, and even in cases of high anisometropia, full correction is often tolerated. In contrast, adults have reduced capacity for sensory adaptation, and symptoms are more likely to become apparent when aniseikonia occurs suddenly (e.g., after cataract surgery).
To maintain binocular fusion, the retinal images of both eyes must maintain a certain similarity in size, shape, and contrast. As aniseikonia increases, the binocular response of corresponding neurons in the visual cortex decreases, interocular suppression becomes dominant, and fusion breaks down.
Although a threshold of 5% has been historically proposed, there is actually wide individual variation, ranging from patients who complain of asthenopia even with 2-3% aniseikonia to those who are asymptomatic even with 8% 8). The capacity to maintain fusion also depends on accommodative reserve, convergence amplitude, and stereopsis, and when these functions are reduced (e.g., fatigue, presbyopia), tolerance to aniseikonia tends to decrease.
Conventional testing instruments (e.g., New Aniseikonia Tests) use analog targets, but quantitative measurement systems using computers or digital screens are being developed. Reports indicate that aniseikonia quantification methods using tablet devices show good correlation with conventional methods, and they are expected to be put into practical use as simple examination tools in outpatient settings.
In refractive surgeries such as LASIK and ICL, aniseikonia may become a problem postoperatively in patients with large preoperative anisometropia. The importance of evaluating aniseikonia preoperatively and planning surgery to minimize the postoperative interocular refractive difference is recognized 1). Particularly in monocular surgery, informed consent after predicting postoperative aniseikonia is important. Five-year outcomes of femtosecond laser arcuate incisions (FLACS-AK) show that preoperative astigmatism stabilizes at 0.55 D postoperatively 3).
IOL Power Optimization Algorithm after Cataract Surgery
In cataract patients with high anisometropia, research is progressing on IOL power optimization algorithms that link the refractive status of the healthy eye with the postoperative target refraction. It is suggested that setting a postoperative refractive target considering aniseikonia contributes to improvement in visual function and quality of life.
Attempts to correct binocular image size in real time using augmented reality (AR) technology and electronic image correction are also in the research stage. The possibility of functioning as an alternative to iseikonic lenses in the future is discussed, but it has not yet reached clinical application.
For retinal aniseikonia caused by epiretinal membrane, macular hole, or macular edema, vitrectomy with membrane peeling or treatment is performed. While membrane peeling may improve metamorphopsia and aniseikonia in some cases, improvement may be incomplete or new symptoms may occur after surgery, so explanation to the patient is important 2).
Matoba R, Morizane Y. Epiretinal membrane: an overview and update. Jpn J Ophthalmol. 2024;68(6):603-613. doi:10.1007/s10384-024-01127-6. PMID:39466371; PMCID:PMC11607056.
Pham TMK, Nguyen XH, Pham TTT, Hoang TT. Five Years Follow-Up Outcomes of Femtosecond Laser-Assisted Cataract Surgery on Patients with Preexisting Corneal Astigmatism. International medical case reports journal. 2025;18:373-379. doi:10.2147/IMCRJ.S506198. PMID:40129561; PMCID:PMC11932028.
Miller KM, Oetting TA, Tweeten JP, Carter K, Lee BS, Lin S, et al. Cataract in the Adult Eye Preferred Practice Pattern. Ophthalmology. 2022;129(1):P1-P126. doi:10.1016/j.ophtha.2021.10.006. PMID:34780842.
American Academy of Ophthalmology. Adult Strabismus Preferred Practice Pattern. Ophthalmology. 2023.
Jin T, Yu L, Li J, Zhou Y. Refractive outcomes of toric intra-ocular lens implantation in cases of high posterior corneal astigmatism. Indian J Ophthalmol. 2023;71(8):2967-71. doi:10.4103/IJO.IJO_3385_22
American Academy of Ophthalmology. Amblyopia Preferred Practice Pattern 2022 Update. Ophthalmology. 2023;130(3):P136-P178.
Wang Y, Xie L, Yao K, et al. Evidence-based guidelines for keratorefractive lenticule extraction surgery. Ophthalmology. 2025;132(4):397-419. doi:10.1016/j.ophtha.2024.11.016. PMID:39577672.
Scheiman M, Kulp MT, Cotter SA, Lawrenson JG, Wang L, Li T. Interventions for convergence insufficiency: a network meta-analysis. The Cochrane database of systematic reviews. 2020;12(12):CD006768. doi:10.1002/14651858.CD006768.pub3. PMID:33263359; PMCID:PMC8092638.
Venter JA, Pelouskova M, Collins BM, Schallhorn SC, Hannan SJ. Visual outcomes and patient satisfaction in 9366 eyes using a refractive segmented multifocal intraocular lens. J Cataract Refract Surg. 2013;39(10):1477-1484. doi:10.1016/j.jcrs.2013.03.035
Mukit FA, Cape HT, Huq SS, Bohn S. An Isolated Case of Unilateral Macro-Ophthalmia With Resultant Anisometropic Amblyopia in Neurofibromatosis 1. Cureus. 2023;15(9):e44679. doi:10.7759/cureus.44679. PMID:37809258; PMCID:PMC10550781.
Copy the article text and paste it into your preferred AI assistant.
Article copied to clipboard
Open an AI assistant below and paste the copied text into the chat box.