Implantable Collamer Lens (ICL) is a type of posterior chamber phakic intraocular lens (pIOL). It corrects refractive errors by inserting a lens between the iris and the natural lens (ciliary sulcus) while preserving the natural lens. It is an intraocular surgery performed under an operating microscope, similar to cataract surgery, but the natural lens is not removed.
The main indication is moderate to high myopia (especially ≥6 D). Since the cornea is not removed, there is no risk of corneal ectasia. It preserves accommodation and offers excellent reversibility. It is particularly useful for cases where LASIK or SMILE is not indicated (thin cornea, high myopia).
Considerations for ICL Surgery Indications (Clinical Decision Flow)
In 1953, Strampelli developed the first anterior chamber pIOL. Early lenses had many complications such as corneal endothelial failure and glaucoma, but in 1977 Worst developed an iris-fixated type, and in 1986 Fyodorov developed a posterior chamber type, improving safety. STAAR Surgical launched the first posterior chamber pIOL in 1993 and received FDA approval in 2005. In March 2022, EVO/EVO+ ICL received FDA approval in the US, and over 2 million lenses have been used worldwide1).
“Collamer” developed by STAAR Surgical is a patented material with the following composition.
Polyhydroxyethyl methacrylate (HEMA): approximately 60%
Water: approximately 36%
Benzophenone: 3.8% (ultraviolet absorber)
Porcine-derived collagen: 0.2%
The collagen content provides high biocompatibility with biological tissues, excellent permeability to gases and metabolites, and extremely low inflammatory response 1). It shows low adsorption of proteins such as fibronectin, and long-term evaluation by specular microscopy and laser flare cell meter confirms no chronic inflammation.
The latest EVO ICL features a 0.36 mm diameter port (KS-AquaPORT) in the center of the optic zone. This provides the following advantages:
Eliminates the need for Nd:YAG laser iridotomy required in previous models
Maintains physiological aqueous humor circulation from the posterior chamber to the anterior chamber
Reduces the incidence of anterior subcapsular cataract and pupillary block
Reduces the risk of postoperative intraocular pressure elevation
The EVO+ model has a larger effective optic zone (up to 7.5 mm), which is expected to reduce glare, halos, and higher-order aberrations in younger patients with larger pupil diameters. In an FDA clinical trial (200 eyes with moderate myopia), 99.7% of eyes maintained appropriate vault, and there were zero cases of angle closure, pigment dispersion, or anterior subcapsular cataract1).
QHow is ICL different from LASIK and SMILE?
A
LASIK and SMILE correct refraction by ablating corneal stroma. ICL preserves the cornea and inserts a lens inside the eye. ICL is reversible (removable) and carries no risk of dry eye or corneal ectasia. For high myopia (6 D or more), ICL is considered superior in visual quality (contrast sensitivity, higher-order aberrations) 1).
Shallow anterior chamber and corneal endothelial damage (endothelial cell density below age-specific minimum)
Pregnancy or breastfeeding
Severe diabetes or severe atopic disease (systemic diseases affecting wound healing)
Precautions include glaucoma, normal-tension glaucoma, systemic connective tissue disease, dry eye, and suspected non-progressive mild keratoconus2).
QPlease tell me the indications and contraindications for ICL.
A
Main indications are myopia of 6D or more, age 21–45, and sufficient anterior chamber depth. Contraindications include progressive keratoconus, active ocular inflammation, cataract, pregnancy, breastfeeding, shallow anterior chamber, and corneal endothelial disorders. Moderate myopia of 3D to less than 6D and high myopia over 15D are considered cautious indications 2).
Design with haptics placed in the anterior chamber angle. Chronic decrease in corneal endothelial cells, pupil ovalization, and nuclear cataract were problematic, and it has now been withdrawn from the market. Not recommended for refractive correction in young patients.
Fixed to the mid-peripheral iris with claws. Chronic decrease in corneal endothelial cells is a concern, but it is safer than the angle-supported type. Requires a large incision, and attention to postoperative astigmatism is necessary 9).
Placed in the ciliary sulcus. It is away from the corneal endothelium, so the risk of endothelial cell loss is low. In EVO/EVO+, the central hole reduces the risk of pupillary block and anterior subcapsular cataract. Can be inserted through a 3.0 mm small incision.
The ESCRS guidelines recommend preoperative evaluation for cataract surgery after anterior chamber pIOL implantation, including checking for iris damage, patency of peripheral iridotomy, and corneal endothelial cell density and morphology 9).
4. Diagnosis and prescription (lens size determination)
Accurate determination of lens size directly affects postoperative outcomes. ICL sizes include 13.2 mm, 13.7 mm, 14.0 mm, and 14.5 mm, and proper size selection is key to vault management.
Direct measurement of the sulcus-to-sulcus (STS) diameter using anterior segment OCT or UBM provides better vault prediction accuracy than WTW and is recommended as a standard preoperative evaluation 4).
The ideal vault (the gap between the ICL and the anterior lens surface) is 250 to 750 μm 2).
Vault status
Risk
Less than 250 μm (low vault)
Contact with the lens → anterior subcapsular cataract
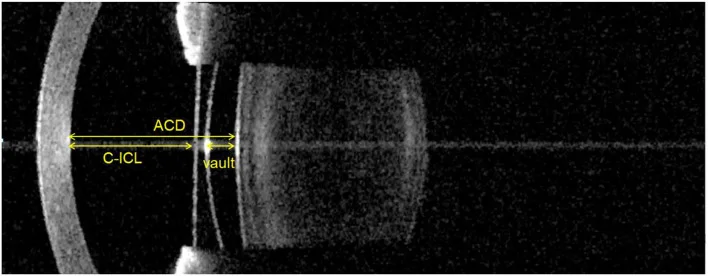
Igarashi A, Kumegawa K, Kamiya K. Comparison of Vault Measurements Using a Swept-Source OCT-Based Optical Biometer and Anterior Segment OCT. Front Med (Lausanne). 2022;9:865719. Figure 1. PMCID: PMC9259877. License: CC BY.
Horizontal cross-sectional image by anterior segment optical coherence tomography (AS-OCT) showing the distance from the corneal endothelium to the anterior ICL surface (C-ICL), the vault from the posterior ICL surface to the anterior lens surface, and the anterior chamber depth (ACD). This corresponds to the postoperative evaluation of vault values (250–750 μm) discussed in the section “4. Diagnosis and Prescription (Lens Size Determination).”
For anterior chamber IOLs, the Van der Heijde nomogram is used to calculate the power from refractive value, corneal refractive power, and anterior chamber depth 9). Postoperative vault tends to decrease over years (due to age-related lens swelling), making regular anterior segment OCT evaluation important 4).
QWhat is vault and why is it important?
A
Vault is the distance between the ICL and the anterior lens surface, measurable with anterior segment OCT. The appropriate range is 250–750 μm. If less than 250 μm, contact with the lens may cause anterior subcapsular cataract. If more than 750 μm, the ICL pushes the iris forward, narrowing the angle and increasing the risk of elevated intraocular pressure and pigment dispersion 2).
Peripheral iridotomy is not required for EVO/EVO+ ICL. When using conventional Visian ICL, YAG laser iridotomy was performed at two superior sites 2–3 weeks before surgery 1).
Since transient intraocular pressure elevation may occur postoperatively, observation for at least 2 hours after surgery is recommended on the day of surgery 2).
Hyphema: Occurs due to rupture of irisciliary body cyst. May heal with conservative treatment (tobramycin/dexamethasone eye drops + atropine gel) 8).
Anterior subcapsular cataract: Occurs when the lens contacts the ICL due to low vault. Incidence 0% in FDA trials for EVO ICL 1).
Retinal detachment: Be aware of preoperative predisposition in high myopia. Preoperative dilated fundus examination to check for retinal tears and lattice degeneration2).
Postoperative monitoring items based on guidelines (8th edition): Check visual acuity, refraction, vault, corneal endothelial cell density, intraocular pressure, and fundus at postoperative day 1, week 1, month 1, month 3, month 6, then every 6–12 months lifelong 2). If vault is less than 250 μm, consider ICL size change or exchange; if over 750 μm, evaluate with gonioscopy.
Differential Diagnosis and Management of Intraocular Pressure Elevation
There are multiple possible causes for early postoperative intraocular pressure elevation3).
In a case reported by Moshirfar et al. (2024), the postoperative IOP elevation was presumed to be due to residual ophthalmic viscosurgical device and early steroid response3). After 6 weeks of observation and steroid tapering, it normalized without requiring lens removal or iridotomy.
The mean corneal endothelial cell loss rate at 6 months was 2.2%1). Long-term studies show stabilization after early postoperative remodeling, with a loss rate of 3.6±7.9% reported at 8 years1). Anterior chamber phakic IOLs carry a higher risk of chronic endothelial cell loss than posterior chamber IOLs, making long-term monitoring important9).
Li et al. (2023) reported two cases of delayed-onset TASS occurring one week after ICL surgery6). Keratic precipitates (KP) and fibrin formation in the anterior chamber were observed, but treatment with oral prednisolone 0.5 mg/kg plus 1% eye drops every hour for 4–5 weeks improved both visual acuity and anterior chamber findings. The incidence rate was 0.24% (2 out of 827 eyes).
Zhang et al. (case report of hyphema) reported a 23-year-old female who developed anterior and posterior chamber hemorrhage due to rupture of an iridociliary cyst after ICL surgery8). Conservative treatment with 0.3% tobramycin/0.1% dexamethasone eye drops (4 times daily) and 1% atropine sulfate ophthalmic gel (twice daily) was continued for 17 days, and healing was achieved without ICL removal.
Zheng et al. (2023) reported a case of Staphylococcus epidermidis endophthalmitis occurring 20 days after ICL surgery7). Intravitreal injections (vancomycin 1 mg + ceftazidime 2 mg) were administered twice, and uncorrected visual acuity recovered to 22/20 without ICL removal or vitrectomy. The incidence of endophthalmitis after ICL surgery is estimated to be approximately 0.017–0.036%.
QWhat should I do if my eye pressure rises after surgery?
A
The most common cause is residual ophthalmic viscosurgical device, which resolves spontaneously within a few days. Management includes tapering steroid eye drops or adding IOP-lowering medications. If due to pupillary block or lens size mismatch, iridotomy or lens exchange may be necessary3).
Collamer has extremely high biocompatibility. Examinations using specular microscopy and laser flare cell meter have confirmed the absence of inflammatory reactions 1). Due to its collagen content, it has high affinity with biological tissues and excellent permeability to gases and metabolic products. Its low surface energy and low adsorption of proteins such as fibronectin are considered reasons for maintaining a long-term low inflammatory state.
The optic zone of the ICL is positioned in an arch-like manner above the lens. Proper maintenance of the vault between the ICL and the lens allows aqueous humor to flow over the lens surface, maintaining nutrient supply to the lens and preventing cataract formation.
The central hole (KS-AquaPORT) of the EVO ICL enables physiological aqueous humor flow from the posterior chamber to the anterior chamber. This provides the following effects:
Prevention of pupillary block (the reason why YAG laser iridotomy, which was necessary in conventional types, is no longer needed)
Maintenance of metabolic product and nutrient supply to the lens
Reduction of the risk of anterior subcapsular cataract
Excessive vault (>750 μm) pushes the iris forward, causing pigment dispersion glaucoma due to contact with the ciliary body. Subsequently, the angle may narrow, potentially progressing to angle-closure glaucoma3). Insufficient vault (<250 μm) leads to accumulation of metabolic products under the anterior lens capsule, forming anterior subcapsular cataract. In FDA trials, 99.7% of eyes achieved satisfactory vault, with zero cases of angle closure, pigment dispersion, or anterior subcapsular cataract1).
In anterior chamber pIOLs, the lens proximity to the corneal endothelium causes micro-movements that exert mechanical stress on endothelial cells. Chronic cell damage leads to a progressive decrease in endothelial cell density over time, potentially resulting in corneal endothelial failure (bullous keratopathy). Posterior chamber ICLs are farther from the corneal endothelium, significantly reducing this risk 9). Long-term data from Kohnen et al. report that the annual endothelial cell loss rate for anterior chamber pIOLs is 2 to 3 times higher than for posterior chamber ICLs 9).
pIOLs adjust the focal point on the retina by placing an additional refractive lens inside the eye. In myopia, a concave (minus) lens delays light convergence, moving the focal point from in front of the retina onto the retina. Unlike glasses, because the lens is positioned near the eye’s principal point, there is almost no image magnification or minification, providing physiological vision. Maintaining good contrast sensitivity is also a characteristic of ICLs.
In an 8-year follow-up by Igarashi et al., the spherical equivalent remained stable (only a change from -10.3 D to +0.09 D), and the decrease rate of corneal endothelial cell density was 3.6 ± 7.9%, indicating that posterior chamber ICL has excellent long-term stability 5). A 5-year follow-up also confirmed maintained efficacy and safety 10). Alfonso et al.’s 5-year follow-up (including Toric ICL) also found no progressive increase in refractive error 10).
7b. Comparison of ICL with Other Refractive Surgeries
LASIK corrects refraction by ablating corneal stroma, causing irreversible changes in corneal structure postoperatively. ICL preserves the cornea and has advantages in the following aspects:
Reversibility: ICL can be removed. When cataracts develop, the ICL can be explanted and standard cataract surgery can be performed.
Dry eye: LASIK cuts corneal nerves, leading to frequent dry eye (30-40% at 6 months postoperatively). ICL preserves the cornea, resulting in a lower incidence.
Risk of corneal ectasia: LASIK alters corneal biomechanics, and if the residual stromal bed is thin, there is a risk of corneal ectasia. ICL has no such risk.
IOL calculation for future cataract surgery: LASIK changes corneal curvature, making IOL power calculation prone to errors. ICL does not affect IOL calculation.
Correction of high myopia: LASIK is limited to about 10 D. ICL can correct up to 20 D.
In evidence-based guidelines by Wang Y et al., it is shown that ICL (ICL) has superior characteristics to LASIK in preserving corneal biomechanics12).
SMILE (small incision lenticule extraction) has no corneal flap, so there are no flap-related complications. However, compared to ICL, there are the following differences:
This is an extended depth of focus (EDOF) ICL that received CE mark approval in July 2020. It provides near and intermediate vision correction through an aspheric optical system and is indicated for both phakic and pseudophakic eyes (after monofocal IOL implantation). The target age is 21 to 60 years, and it is awaiting FDA approval in the United States.
Previously, the main indication was high myopia of 6D or more, but with improved safety of EVO ICL, indications are expanding to moderate to low myopia. In FDA clinical trials, about one-third of subjects had moderate myopia less than 6D, and safety and efficacy were consistent across the full range of myopia1).
The advent of swept-source anterior segment OCT has enabled precise measurement of angle-to-angle distance and ciliary sulcus diameter. This has improved the prediction accuracy of postoperative vault and contributes to reducing the risk of cataract and angle closure. In a study by Igarashi et al., vault measurements from swept-source OCT-based optical biometry and anterior segment OCT showed good correlation, but due to systematic differences, it is recommended to use the same device for postoperative monitoring 4).
The global spread of myopia is a serious public health issue, with projections that by 2050, 4.9 billion people worldwide will be myopic and 940 million will have high myopia11). High myopia (≥ -6D) increases the risk of ocular complications such as retinal tears, glaucoma, and macular degeneration. ICL has accumulated long-term safety and efficacy evidence as a standard surgical correction for high myopia of 6D or more.
A meta-analysis by Packer (2016) confirmed that central hole design ICL significantly reduces the risk of anterior subcapsular cataract, angle closure, and pupillary block compared to non-central hole designs 13).
Sun et al. (2023) reported a technique to reduce vault by rotating the ICL 90° in cases of excessive postoperative vault (high vault) 14). The mean vault improved from 1,249 μm to 459 μm, and angle and intraocular pressure normalized. This non-invasive management method avoids ICL exchange. The ESCRS guidelines recommend evaluation of iris damage, patency of peripheral iridotomy, and corneal endothelial cells in cataract surgery after anterior chamber pIOL implantation 15).
QCan presbyopia also be corrected?
A
An ICL for presbyopia correction called EVO Viva has been developed and has received CE mark approval in Europe. It is designed to improve near and intermediate vision using an EDOF optical system, but is awaiting FDA approval in the United States. Currently, it is not a standard treatment.
Expansion of ICL Indications and Management of Low Myopia
Traditionally, ICL was mainly indicated for high myopia of 6D or more, but with improved safety of EVO ICL, indications are expanding to moderate to low myopia. In FDA clinical trials, about one-third of subjects had moderate myopia less than 6D, and safety and efficacy were consistent across the full range of myopia1). The Refractive Surgery Guidelines (8th edition) consider 3D to less than 6D as cautious indication 2), and the indication is determined by comprehensively considering the degree of myopia, corneal shape, and patient needs.
For low myopia (less than 6D), LASIK or SMILE are common options, but ICL can be an option for patients with thin corneas, difficulty wearing contact lenses, or dry eye. The reversibility of ICL is also advantageous in that it can address future postoperative refractive changes (e.g., myopia progression, effects of presbyopia).
In the EVO ICL FDA clinical trial, 97.6% of patients were satisfied with the surgery, and good results were shown in contrast sensitivity, higher-order aberrations, and night vision function in terms of visual quality 1). Freedom from glasses and contact lenses, and the ability to engage in sports and water activities contribute to high satisfaction. However, early postoperative glare and halos (especially light rings in dark conditions) can be problematic for some patients, so preoperative measurement of scotopic pupil diameter and thorough explanation are important.
Packer M. The EVO ICL for Moderate Myopia: Results from the US FDA Clinical Trial. Clinical ophthalmology (Auckland, N.Z.). 2022;16:3981-3991. doi:10.2147/OPTH.S393422. PMID:36510599; PMCID:PMC9738966.
Moshirfar M, Moin KA, Pandya S, Karimian F, Zaugg B, Khan S, et al. Severe intraocular pressure rise after implantable collamer lens implantation. Journal of cataract and refractive surgery. 2024;50(9):985-989. doi:10.1097/j.jcrs.0000000000001534. PMID:39183446; PMCID:PMC11338031.
Du Y, Jin C, Yin S, Wang G, Ma Q, Li Y, Chen B, Wang H, et al. Comparison of Vault Measurements Using a Swept-Source OCT-Based Optical Biometer and Anterior Segment OCT. Frontiers in medicine. 2022;9:865719. doi:10.3389/fmed.2022.865719. PMID:35814765; PMCID:PMC9259877.
Igarashi A, Shimizu K, Kamiya K. Eight-year follow-up of posterior chamber phakic intraocular lens implantation for moderate to high myopia. American journal of ophthalmology. 2014;157(3):532-9.e1. doi:10.1016/j.ajo.2013.11.006. PMID:24239774.
Li L, Zhou Q. Late-onset toxic anterior segment syndrome after ICL implantation: two case reports. BMC Ophthalmol. 2023;23:61. doi:10.1186/s12886-022-02713-3.
Zheng K, Zheng X, Gan D, Zhou X. Successful antibiotic management of Staphylococcus epidermidis endophthalmitis after implantable collamer lens implantation. BMC ophthalmology. 2023;23(1):410. doi:10.1186/s12886-023-03127-5. PMID:37828437; PMCID:PMC10568818.
Zhang W, Li F, Zhou J. Anterior Segment Hemorrhage after Implantable Collamer Lens Surgery. Ophthalmology. 2025;132(4):e72. doi:10.1016/j.ophtha.2024.06.015. PMID:39046379. 2023.
Kohnen T, Kook D, Morral M, Güell JL. Phakic intraocular lenses: part 2 — results and complications. J Cataract Refract Surg. 2010;36:2168-2194. doi:10.1016/j.jcrs.2010.10.007. PMID:21111322.
Alfonso JF, Baamonde B, Fernández-Vega L, Fernandes P, González-Méijome JM, Montés-Micó R. Posterior chamber collagen copolymer phakic intraocular lenses to correct myopia: five-year follow-up. Journal of cataract and refractive surgery. 2011;37(5):873-80. doi:10.1016/j.jcrs.2010.11.040. PMID:21511154.
Holden BA, Fricke TR, Wilson DA, et al. Global prevalence of myopia and high myopia and temporal trends from 2000 through 2050. Ophthalmology. 2016;123(5):1036-1042. doi:10.1016/j.ophtha.2016.01.006. PMID:26875007.
Wang Y, Xie L, Yao K, Sekundo W, Alió JL, Mehta JS, Goel S, Elmassry A, Schallhorn J, Shilova T, Cao H, Xu L, Chen X, Zhang F, Bai J, Zhang W, Liu Q, Zhou X, Chen Y, Wang Z, Jhanji V, Yang K, Writing Committee for the Guideline Working Group. Evidence-Based Guidelines for Keratorefractive Lenticule Extraction Surgery. Ophthalmology. 2025;132(4):397-419. doi:10.1016/j.ophtha.2024.11.016. PMID:39577672.
Packer M. Meta-analysis and review: effectiveness, safety, and central port design of the intraocular collamer lens. Clinical ophthalmology (Auckland, N.Z.). 2016;10:1059-77. doi:10.2147/OPTH.S111620. PMID:27354760; PMCID:PMC4907705.
Jiang Y, Luo Y, Li Y, Lu T. The long-term observation of the rotation of implantable collamer lens as the management of high postoperative vault. Frontiers in medicine. 2023;10:1104047. doi:10.3389/fmed.2023.1104047. PMID:36910497; PMCID:PMC9995363.
European Society of Cataract and Refractive Surgeons (ESCRS). ESCRS Clinical Guidelines for Cataract Surgery. Brussels: ESCRS; 2024.
Copy the article text and paste it into your preferred AI assistant.
Article copied to clipboard
Open an AI assistant below and paste the copied text into the chat box.