Normal-tension glaucoma is a subtype of primary open-angle glaucoma (broad sense) in which intraocular pressure always remains within the statistically determined normal range during the development and progression of glaucomatous optic neuropathy5). It requires the presence of normal intraocular pressure, normal open angle, normal slit-lamp microscopy findings, glaucomatous optic neuropathy, and glaucomatous visual field defects.
The intraocular pressure distribution in Japanese adults was analyzed in detail in the Tajimi Study, with right eye pressure 14.6±2.7 mmHg and left eye pressure 14.5±2.7 mmHg 5). Defining the normal range as mean ± 2 standard deviations, the upper limit of normal in Japanese is 19.9–20.0 mmHg. Based on this epidemiological data, it is considered reasonable to clinically distinguish primary open-angle glaucoma (narrow sense) from normal-tension glaucoma using an intraocular pressure of 20 mmHg as the cutoff 5).
Primary open-angle glaucoma (broad sense) is a chronic progressive optic neuropathy characterized morphologically by enlargement of the optic disc cupping, thinning of the neuroretinal rim, and defects in the retinal nerve fiber layer (RNFL). Primary open-angle glaucoma (broad sense) is conveniently divided into a high intraocular pressure group (primary open-angle glaucoma, narrow sense) and a normal intraocular pressure group (normal-tension glaucoma), but both have the same treatment strategy and are clinically treated as a continuous disease spectrum 5, 7).
In the Tajimi Study, the prevalence of glaucoma among Japanese individuals aged 40 years and older was reported to be 5.0%, and the prevalence of normal-tension glaucoma was 3.6% 5). Based on population statistics from 2016, the estimated number of glaucoma patients in Japan is approximately 4.65 million. The same study revealed that the rate of newly detected cases reached 89%, indicating that many patients with glaucoma remain undiagnosed and untreated 5).
Normal-tension glaucoma is a representative disease type, accounting for about 90% of primary open-angle glaucoma (broad sense) and about 70% of all glaucoma. It is estimated that approximately 1 in 28 adults aged 40 years or older has normal-tension glaucoma, making it by no means a rare disease.
Normal-tension glaucoma is prone to underdiagnosis due to its glaucomatous changes at normal intraocular pressure levels 7). It has been reported that about 40% of patients with primary open-angle glaucoma do not show elevated intraocular pressure during examination 8), posing a clinical challenge that diagnosis cannot be made based solely on initial intraocular pressure. The limitations of intraocular pressure screening for glaucoma detection are clear, and combined evaluation of the optic disc and retinal nerve fiber layer is key to early detection 5). The 89% new detection rate observed in the Tajimi Study indicates a large number of untreated potential patients, underscoring the importance of screening systems and awareness among high-risk groups 5).
In the past, there was a view that primary open-angle glaucoma (narrow sense) and normal-tension glaucoma were independent diseases. However, due to the similarity in clinical findings, treatment response, and intraocular pressure-related pathophysiology, they are now classified as a continuous disease group under the overarching concept of primary open-angle glaucoma (broad sense) 5, 7). The boundary of 20 mmHg is a convenient classification based on the statistical upper limit of normal in Japanese, and it does not sharply divide disease types by intraocular pressure alone. Cases ranging from ocular hypertension to primary open-angle glaucoma (narrow sense), normal-tension glaucoma, and even those with progressive optic neuropathy at lower intraocular pressures are positioned as a single spectrum.
QAre normal-tension glaucoma and primary open-angle glaucoma (narrow sense) different diseases?
A
Both are subtypes of primary open-angle glaucoma (broad sense) and can be treated as a continuous disease spectrum 5, 7). IOP lowering is central to treatment in both primary open-angle glaucoma (narrow sense) and normal-tension glaucoma. However, normal-tension glaucoma still requires attention to non-IOP factors, differential diagnosis such as compressive lesions, and context-dependent clinical distinction and evaluation.
In the early stages, subjective symptoms are often absent. As the disease progresses, visual field defects become noticeable, and paracentral scotomas are relatively common. The presence of paracentral scotomas means that central visual function (reading letters, recognizing faces) may be affected from an early stage.
Localized scotomas within the central 10 degrees that are not detected by the Humphrey Field Analyzer 24-2 program have been reported, and they may be identified for the first time with the 10-2 program 1). In cases of normal-tension glaucoma with paracentral scotomas, one cannot be reassured solely by the results of the 24-2 test.
Intraocular pressure: Always 20 mmHg or less is a necessary condition 5). Measurement of diurnal intraocular pressure variation at different times is an essential test. In addition to diurnal variation, intraocular pressure also shows seasonal variation, generally higher in winter and lower in summer, so the time of measurement should also be considered in evaluation 5).
Angle: Normal open angle. Often more typical than in primary open-angle glaucoma (narrow sense).
Slit-lamp examination: No abnormalities in the anterior segment.
Optic disc: Enlarged cupping, thinning of the neuroretinal rim, and retinal nerve fiber layer defects. Since morphological findings are similar to those in primary open-angle glaucoma (narrow sense), differentiation cannot be made based on disc findings alone.
Visual field: Paracentral scotomas and arcuate scotomas are observed.
Retinal nerve fiber layer and retinal ganglion cell layer: Optical coherence tomography (OCT) shows thinning of the retinal nerve fiber layer and thinning of the macular retinal ganglion cell layer (GCL).
Peripapillary atrophy (PPA): Beta zone is frequently observed and commonly occurs at the thinnest part of the rim.
Optic disc findings considered frequent in normal-tension glaucoma
More frequent than in primary open-angle glaucoma (narrow sense)
Size of optic disc cupping
Larger in cases with similar visual field abnormalities
Localized cupping enlargement
Higher proportion observed
Peripapillary atrophy (PPA β zone)
Frequently observed
Based on optic disc findings, a classification method for normal-tension glaucoma into focal ischemic type, myopic type, senile sclerotic type, etc., has also been proposed. These types are thought to reflect differences in the underlying pathophysiology (local circulatory disturbance, myopic structural changes, age-related sclerosis).
Visual field defects in normal-tension glaucoma are characterized by typical glaucomatous patterns such as arcuate scotoma, nasal step, and paracentral scotoma, as well as localized scotomas within the central visual field. Paracentral scotomas within 10 degrees of the fovea directly affect activities of daily living such as reading and face recognition, making them likely to appear as subjective symptoms of progression. On visual field testing, they are detected as threshold reductions near the fixation point. Since the 24-2 program of the Humphrey Field Analyzer has relatively sparse test points within the central 10 degrees, paracentral scotomas may be missed; additional evaluation with the 10-2 program is useful depending on the case 1).
The MD (mean deviation) slope from static automated perimetry is used as an objective indicator of glaucoma progression. In normal-tension glaucoma, the MD slope tends to be more gradual than in primary open-angle glaucoma (narrow sense), but individual variability is large, and rapidly progressive cases occur with a certain frequency. Cases with recurrent disc hemorrhages, poor medication adherence, or nocturnal hypotension are considered to have accelerated progression, requiring adjustment of follow-up frequency 5). Longitudinal changes in retinal nerve fiber layer thickness measured by OCT are also useful for monitoring progression, and structural changes may be detected before visual field abnormalities become apparent.
Even in normal-tension glaucoma, intraocular pressure (IOP) is the strongest factor associated with onset and progression, and clinical evidence has shown that IOP-lowering treatment can suppress progression 5, 11). Even if IOP is within the statistically normal range, each optic nerve has a tolerable IOP level, and IOP values that are excessive for the individual optic nerve are involved in the pathogenesis.
Due to diurnal and seasonal IOP variations, it is possible that high IOP occurs outside of examination times. Furthermore, since the pressure load on the optic nerve head involves not only IOP but also cerebrospinal fluid pressure, the actual pressure load on the optic nerve head may differ among individuals even at the same IOP level 4).
As IOP-independent mechanisms, structural vulnerability of the lamina cribrosa, circulatory disorders, neurotoxic factors, immune factors, and genetic abnormalities have been suggested. In an umbrella review of meta-analyses published in 2024 9), the evidence hierarchy for risk factors of glaucoma in general was organized. Key findings related to the understanding of normal-tension glaucoma pathology are shown below.
Ocular local risk factors
Intraocular pressure: highly suggestive evidence (odds ratio 2.43, 95% confidence interval 1.71–3.47) 9). Even within the normal range, higher values contribute to onset and progression.
Myopia: highly suggestive evidence (odds ratio 1.89, 95% confidence interval 1.55–2.32) 9). In particular, high myopia with optic disc structural changes is deeply involved in onset.
Corneal hysteresis (CH): highly suggestive evidence (odds ratio 0.18, 95% confidence interval 0.13–0.26) 9). Decreased corneal biomechanical properties are associated with progression risk.
Central corneal thickness: Thin cornea is a risk factor for progression 5, 9).
Disc hemorrhage: Frequent in normal-tension glaucoma. After its appearance, visual field progression accelerates 5).
Peripapillary choroidal atrophy (PPA β-zone): Enlargement of the β-zone is associated with progression 5).
Systemic Risk Factors
Decreased ocular perfusion pressure (OPP): suggestive evidence9). It is also clearly listed as a progression risk factor in the 5th edition of the Glaucoma Clinical Practice Guidelines5).
Decreased diastolic and systolic blood pressure: including nocturnal hypotension, associated with progression5).
Four main genes are involved in normal-tension glaucoma. OPTN (optineurin) mutations, particularly the E50K variant, are strongly associated with early-onset disease. Copy number variations of TBK1 are also associated with normal-tension glaucoma and contribute to retinal ganglion cell loss. METTL23 mutations have been identified in familial normal-tension glaucoma cases. MYOC, associated with primary open-angle glaucoma, is also involved in some normal-tension glaucoma cases.
Lamina Cribrosa and Trans-lamina Cribrosa Pressure Difference
Structural vulnerability of the lamina cribrosa: structural abnormality that cannot withstand normal intraocular pressure.
Increased trans-lamina cribrosa pressure difference: decreased retrolaminar cerebrospinal fluid pressure, rather than increased intraocular pressure, may cause an increase in the trans-lamina cribrosa pressure difference4).
Impaired cerebrospinal fluid dynamics: patients with normal-tension glaucoma have elevated L-PGDS concentration in the cerebrospinal fluid, suggesting systemic cerebrospinal fluid dynamic abnormalities4).
Glymphatic system insufficiency: The hypothesis that reduced metabolic waste removal in the optic nerve contributes to glaucomatous damage
Aging, Family History, Myopia
Aging: Age is an independent risk factor for the onset and progression of glaucoma5)
Family history: A family history of glaucoma increases the risk of developing the disease5)
Myopia: Especially high myopia is deeply involved in the pathology through changes in optic disc structure5, 9)
Female: Some epidemiological studies report a slightly higher prevalence in women, but the Tajimi Study found no significant gender difference in Japanese5)
QAre sleep apnea syndrome and Raynaud's phenomenon related to normal-tension glaucoma?
A
Yes, associations have been reported. A 2024 meta-analysis umbrella review classified both obstructive sleep apnea syndrome and migraine as suggestive evidence risk factors for glaucoma9). Primary vascular dysregulation, including cold sensitivity and Raynaud’s phenomenon, is frequently observed in normal-tension glaucoma and is presumed to affect optic nerve head circulation through fluctuations in ocular perfusion pressure5). Management of these systemic conditions is also positioned as an adjunctive measure to slow progression in glaucoma practice guidelines5).
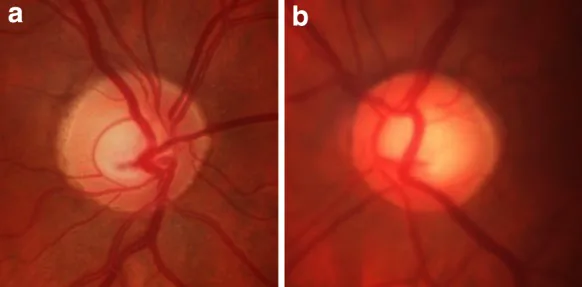
Joanna Karaśkiewicz; Monika Drobek-Słowik; Wojciech Lubiński. Pattern electroretinogram (PERG) in the early diagnosis of normal-tension preperimetric glaucoma: a case report. Doc Ophthalmol. 2014 Oct 19;128(1):53-58. Figure 1. PMCID: PMC3890055. License: CC BY.
The left and right fundus photographs show enlargement of the optic disc cupping. This is a useful visual aid to explain that optic nerve damage progresses even in normal-tension glaucoma.
Exclusion of other optic nerve diseases and secondary intraocular pressure elevation
In diagnosing normal-tension glaucoma, it is necessary to rule out any history of elevated intraocular pressure, both current and past, and to exclude other causes of optic nerve damage besides intraocular pressure load. A history of trauma, steroid use, and inflammatory diseases such as optic neuritis should be excluded through patient interview, and gonioscopy should be performed to check for findings suggestive of past intraocular pressure elevation (e.g., narrow angle, pseudoexfoliation, peripheral anterior synechiae, abnormal pigmentation).
Diurnal intraocular pressure measurement: Multiple measurements at different times of day. Inpatient morning and evening measurements or outpatient measurements at different times are used5).
Seasonal variation assessment: Consider the tendency for higher intraocular pressure in winter and lower in summer5).
Remission phase of Posner-Schlossman syndrome: History of past episodes of elevated intraocular pressure
Secondary open-angle glaucoma: Exclude exfoliation glaucoma, pigmentary glaucoma, etc., based on anterior segment findings
Non-glaucomatous Optic Neuropathies
Intracranial compressive lesions: Pituitary adenoma, internal carotid artery aneurysm, etc., may present with glaucoma-like optic disc cupping2, 3). Visual field defects respecting the vertical meridian suggest compressive lesions 2)
Superior segmental optic nerve hypoplasia (SSOH): Prevalence 0.3% in the Tajimi Study. Differentiated by superior-to-nasal retinal nerve fiber layer defect, upward displacement of the cup and central retinal artery and vein origin
Sequelae of optic neuritis: Optic disc cupping due to past inflammation
When atypical course (rapid unilateral progression, visual acuity loss, visual field defect along the vertical meridian) is observed, imaging studies to exclude intracranial lesions are recommended 2, 3).
During follow-up after diagnosis, intraocular pressure measurement, visual field testing, and OCT are combined to assess progression. For visual field testing, it is recommended to perform multiple tests at intervals of 3 to 4 months in the early stage to establish a reliable baseline 5). Longitudinal changes in retinal nerve fiber layer thickness measured by OCT can detect structural progression before visual field abnormalities become apparent, providing a basis for early intervention. Fundus photography is useful for year-to-year comparison of optic disc findings, tracking the presence of disc hemorrhages, enlargement of peripapillary atrophy, and changes in the neuroretinal rim 5). It is desirable to integrate structural and functional test results and reconsider treatment strategy when either shows a change.
QIs brain MRI necessary for diagnosing normal-tension glaucoma?
A
Routine neuroimaging is not recommended for all patients with normal-tension glaucoma 2). However, if atypical progression patterns (rapid unilateral deterioration, visual acuity loss, visual field defects respecting the vertical meridian) are observed, brain MRI/MRA (magnetic resonance angiography) is necessary to rule out compressive lesions such as pituitary adenoma2) or internal carotid artery aneurysm 3).
In normal-tension glaucoma, the only treatment with established evidence is intraocular pressure (IOP) lowering therapy 5). Other interventions (neuroprotection, blood flow improvement) are promising but have limited evidence compared to IOP lowering.
Collaborative Normal-Tension Glaucoma Study (CNTGS)5, 11): This is a landmark multicenter study on normal-tension glaucoma. In the group that achieved a 30% or greater reduction in IOP from untreated baseline, progression of visual field damage was significantly suppressed compared to the untreated group. In the CNTGS follow-up analysis, after censoring for cataract development, progression of visual field damage was reported in 12% of the treated group and 35% of the control group (evidence level 1B). However, to achieve a 30% or greater IOP reduction, filtration surgery was performed in more than half of the cases, and postoperative cataract progression sometimes led to visual function decline 5).
Early Manifest Glaucoma Trial (EMGT)6): This trial included POAG, NTG, and exfoliation glaucoma, and showed that lowering IOP by approximately 25% reduced the relative risk of progression by 50%. It holds an important position as a study including NTG.
According to the 5th edition of the Glaucoma Clinical Practice Guidelines, drug treatment for normal-tension glaucoma should follow that for primary open-angle glaucoma (narrow sense), and prostaglandin FP receptor agonists are recommended as first-line therapy (evidence level 1B) 5).
Generic Name
Concentration
Dosage
Latanoprost
0.005%
Once daily instillation
Travoprost
0.004%
Instill once daily
Tafluprost
0.0015%
Instill once daily
Bimatoprost
0.03%
Instill once daily
FP receptor agonists lower intraocular pressure mainly by increasing aqueous humor outflow through the uveoscleral pathway. Known side effects include conjunctival hyperemia, corneal epithelial damage, hypertrichosis of the eyelashes and eyelids, iris and eyelid pigmentation, and deepening of the upper eyelid sulcus, collectively referred to as prostaglandin-associated periorbitopathy (PAP) 5).
If the effect is insufficient or contraindicated, beta-blockers (e.g., timolol maleate 0.5%), carbonic anhydrase inhibitors (e.g., dorzolamide hydrochloride 2%, brinzolamide hydrochloride 1%), alpha-2 adrenergic receptor agonists (e.g., brimonidine tartrate 0.2%), Rho kinase inhibitors, or EP2 receptor agonists (e.g., omidenepag isopropyl 0.002%) may be added or substituted 5).
Setting a target intraocular pressure (IOP) is fundamental to glaucoma treatment. The basic goal is a 20–30% reduction from the untreated IOP, and the target is individually determined based on disease stage, risk factors, age, life expectancy, and the condition of the fellow eye 5).
The 5th edition of the Glaucoma Practice Guidelines proposes target IOP levels by disease stage: ≤19 mmHg for early stage, ≤16 mmHg for moderate stage, and ≤14 mmHg for advanced stage 5). In normal-tension glaucoma, baseline IOP is often in the low teens, and IOP-lowering treatment may have limitations. Flexible target setting that prioritizes the patient’s quality of life, rather than rigid numerical goals, is recommended.
The intraocular pressure-lowering effect of laser trabeculoplasty (ALT/SLT) is considered relatively small in normal-tension glaucoma, and it is not actively recommended 5). However, it may be an option in cases of poor adherence to medication.
If sufficient intraocular pressure reduction cannot be achieved with eye drops, or if the progression is rapid, filtering surgery should be considered 5). Trabeculectomy (with mitomycin C) is the standard, and minimally invasive glaucoma surgery (MIGS) has recently become an option. In the CNTGS, filtering surgery was performed in more than half of the cases to achieve the target pressure, but postoperative cataract progression caused visual function decline at a certain frequency, requiring careful judgment regarding surgical indications 5).
In addition to intraocular pressure-lowering treatment, therapies to improve optic nerve blood flow and neuroprotective treatments have been studied 5).
Low-Pressure Glaucoma Treatment Study (LoGTS)5, 6, 10): This was a multicenter, double-blind, randomized trial involving 178 glaucoma patients with intraocular pressure ≤21 mmHg, comparing brimonidine tartrate 0.2% eye drops with timolol maleate 0.5% eye drops. Over a 48-month observation period, both drugs had equivalent intraocular pressure-lowering effects, but Kaplan-Meier survival analysis showed a significantly lower rate of visual field progression in the brimonidine group (9.1%) compared to the timolol group (39.2%) (evidence level 2B) 5, 10). This result suggests that brimonidine may have neuroprotective effects beyond its intraocular pressure-lowering effect. However, the dropout rate was high, requiring caution in interpreting the results, and currently there is no established neuroprotective drug with evidence for normal-tension glaucoma 5).
Interventions aimed at improving ocular blood flow, such as calcium channel blockers (nilvadipine), cassis anthocyanins, and Ginkgo biloba extract, have been attempted, but the evidence is insufficient 5).
The 5th edition of the Glaucoma Clinical Practice Guidelines positions the management of systemic progression factors as adjunctive therapy 5). Specific targets include CPAP therapy for obstructive sleep apnea syndrome, review of antihypertensive medications causing nocturnal hypotension, and management of migraines 5, 9).
In patients receiving antihypertensive therapy, excessive nocturnal blood pressure reduction may decrease ocular perfusion pressure, so it is necessary to consider adjusting the target blood pressure and medication timing in collaboration with the primary care physician. If nocturnal hypotension is confirmed by 24-hour blood pressure monitoring, adjustments such as avoiding antihypertensive medication before bedtime or reducing the dose are considered useful. Obstructive sleep apnea syndrome can affect ocular circulation through nocturnal hypoxia and hemodynamic fluctuations, so sleep testing is recommended in patients with findings such as snoring, excessive daytime sleepiness, or obesity.
The frequency of clinic visits after starting treatment is individually determined based on disease stage, progression rate, and treatment response. Generally, for stable cases, intraocular pressure measurement and fundus evaluation every 3 to 6 months, and visual field testing and OCT examination every 6 to 12 months are standard 5). For progressive cases, after treatment changes, or immediately after detection of disc hemorrhage, the follow-up interval should be shortened. Since treatment is continued throughout life, long-term management including confirmation of medication adherence, evaluation of side effects, and response to life changes (relocation, new onset of systemic diseases) is important.
QIs intraocular pressure-lowering treatment also performed for normal-tension glaucoma?
A
Yes. The CNTGS study showed that lowering intraocular pressure within the normal range by 30% or more reduced the progression rate of visual field damage from 35% to 12% 5, 11). The EMGT study also showed that lowering intraocular pressure by about 25% reduced the relative risk of progression by 50% 6). Even in normal-tension glaucoma, intraocular pressure is the most important modifiable risk factor, and intraocular pressure reduction is the only evidence-based treatment 5).
The biomechanical theory of the optic nerve head suggests that intraocular pressure-related stress and strain on connective tissue affect the lamina cribrosa, peripapillary sclera, axons, glial cells, and vascular endothelium. The lamina cribrosa is a structural key point through which axons of retinal ganglion cells pass, and deformation or damage here is the starting point of axonal damage. In normal-tension glaucoma, even with intraocular pressure within the statistically normal range, axonal damage can occur due to individual structural vulnerability of the lamina cribrosa.
Axonal Transport Impairment and Retinal Ganglion Cell Death
The main cause of retinal ganglion cell death in glaucoma is axonal damage, and the site of onset is considered to be the lamina cribrosa of the optic nerve head. The “neurotrophic factor deprivation hypothesis” has been proposed, in which axonal transport impairment blocks the supply of neurotrophic factors to the cell body, triggering an apoptotic pathway involving accumulation of abnormal mitochondria in the cell body. The apoptotic pathway involves the Bcl-2 family, caspase cascade, and others.
The actual pressure load on the optic nerve head is understood as the difference between intraocular pressure and retrolaminar cerebrospinal fluid pressure (translaminar pressure gradient) 4). Even with the same intraocular pressure, if the cerebrospinal fluid pressure is low, the translaminar pressure gradient becomes larger, increasing the stress on the lamina cribrosa. In normal-tension glaucoma, it has been suggested that a decrease in cerebrospinal fluid pressure, rather than an increase in intraocular pressure, may cause an increase in the translaminar pressure gradient 4). Elevated levels of L-PGDS (lipocalin-type prostaglandin D synthase) in the cerebrospinal fluid of patients with normal-tension glaucoma suggest systemic abnormalities in cerebrospinal fluid dynamics 4).
Circulatory Disturbance and Vascular Dysregulation
In normal-tension glaucoma, vascular dysregulation at the optic nerve head is involved in the pathology. Optic disc hemorrhages are frequently observed in normal-tension glaucoma, and the progression of visual field damage accelerates after the appearance of disc hemorrhages 5). Optical coherence tomography angiography (OCTA) reveals loss of intrapapillary capillaries and dropout of radial peripapillary capillaries corresponding to retinal nerve fiber layer defects in glaucomatous eyes.
Systemic hypotension, fluctuations in ocular perfusion pressure due to nocturnal blood pressure drops, abnormalities in vascular tone regulation by endothelin-1, and primary vascular dysregulation are thought to be involved in the pathology. In patients with migraine, Raynaud’s phenomenon, or cold extremities, peripheral vascular autoregulation is impaired, supporting the hypothesis that this contributes to glaucomatous optic neuropathy through fluctuations in ocular circulation 9).
In recent years, it has been suggested that neuroinflammation, microglial activation, and reactive changes in astrocytes are also involved in glaucomatous optic neuropathy. Remodeling of the supporting tissue around the lamina cribrosa is a chronic response to mechanical stress and may worsen the environment supporting axons. Autoantibody reactions and involvement of the complement system have also been reported, and immune mechanisms in normal-tension glaucoma are an important area for future research. Immune, inflammatory, circulatory, and mechanical stress factors are not independent but interact to form the pathology, and therapeutic interventions targeting a single factor often fail to completely suppress disease progression.
The onset and progression of normal-tension glaucoma are understood as a complex imbalance of (1) individual lamina cribrosa tolerance, (2) translaminar pressure gradient (difference between intraocular pressure and cerebrospinal fluid pressure), (3) optic nerve head circulation (ocular perfusion pressure and autoregulation), (4) neurotrophic factor support, (5) immune and neuroinflammatory factors, and (6) genetic predisposition. Clinically modifiable factors are limited to intraocular pressure and systemic circulation (blood pressure, OSA, migraine management), so optimization of both is central to treatment 5, 9).
He and Chopra (2023) reported two cases of normal-tension glaucoma patients whose Humphrey Field Analyzer 24-2 results were within normal range, but paracentral scotomas were first detected with the Humphrey Field Analyzer 10-2 1). One case was an Asian woman with a history of migraine and hypotension, and the other was an African American man. Both had normal intraocular pressure and were diagnosed with normal-tension glaucoma after exclusion by retinal specialists and neuro-ophthalmologists. Comprehensive visual field assessment including Humphrey Field Analyzer 10-2 is recommended for suspected normal-tension glaucoma.
Cheng et al. (2023) reported a case of a 65-year-old man with normal-tension glaucoma complicated by a nonfunctioning pituitary adenoma (3.1×2.3×2.8 cm) 2). Visual field testing revealed a nasal step associated with bitemporal hemianopia related to the vertical meridian, and MRI was performed due to suspicion of intracranial lesion. The bitemporal defect disappeared after tumor resection.
Ashok et al. (2024) reported a case of a 72-year-old woman who had been managed as normal-tension glaucoma for several years but developed rapid unilateral visual field deterioration, leading to the discovery of a giant left internal carotid artery-ophthalmic artery aneurysm (16×8 mm) 3). After treatment with platinum coils, bilateral thinning of the retinal nerve fiber layer progressed, suggesting coexistence of normal-tension glaucoma and compressive lesion.
Cerebrospinal Fluid Dynamics and Neurodegenerative Diseases
Killer and Pircher (2021) discussed the possibility that impaired cerebrospinal fluid dynamics in patients with normal-tension glaucoma may share common mechanisms with other neurodegenerative diseases such as Alzheimer’s disease and Parkinson’s disease 4). The hypothesis has been proposed that compartmentalization of the optic nerve sheath locally impairs cerebrospinal fluid circulation and contributes to the pathogenesis of normal-tension glaucoma. Systemic assessment of cerebrospinal fluid dynamics may lead to future exploration of biomarkers and therapeutic targets.
Re-evaluation of Evidence for Systemic Factors through Meta-Analysis
In an umbrella review by Shen et al. (2024) 9), 36 systematic reviews and meta-analyses were integrated, evaluating 87 factors for glaucoma. Ocular perfusion pressure, obstructive sleep apnea syndrome, migraine, and hyperlipidemia were classified as suggestive evidence, and therapeutic interventions targeting these systemic factors (revision of antihypertensive drugs, CPAP therapy, migraine management) are attracting attention as future treatment targets. Corneal hysteresis was positioned as a highly suggestive evidence predictor of progression. These systemic factors complement the traditional intraocular pressure-centered glaucoma care model, and the possibility of personalized treatment incorporating ocular perfusion pressure monitoring and systemic risk scores is being discussed for the future.
Research trends in neuroprotection and gene therapy
As therapeutic targets other than intraocular pressure reduction, neuroprotection, neuroregeneration, and gene therapy are being explored in basic and clinical research. Molecular targets for optic nerve protection include Brn-3 transcription factor, BDNF (brain-derived neurotrophic factor), and CNTF (ciliary neurotrophic factor), with promising results reported in animal models. The intraocular pressure-independent visual field protective effect of brimonidine tartrate demonstrated in LoGTS 10) suggested the possibility of neuroprotection via α2 receptors, but large-scale follow-up studies are limited. For gene therapy, interventions targeting glaucoma-related genes such as MYOC and OPTN, and gene transfer to restore aqueous humor outflow function are under investigation. All of these still have many challenges before clinical introduction and are not established treatments.
Artificial intelligence for progression prediction
Approaches to predict progression risk by analyzing retinal nerve fiber layer thickness and visual field data using deep learning are also being studied. Attempts to predict future progression from early normal-tension glaucoma cases may lead to personalized target intraocular pressure settings and optimization of follow-up intervals. However, clinical application requires external validation in multicenter settings, and at present, it does not replace clinical decision-making in routine practice.
He JZ, Chopra V. Unusual Presentations of Low-Tension Glaucoma. Case reports in ophthalmology. 2023;14(1):115-120. doi:10.1159/000529666. PMID:36968809; PMCID:PMC10035547.
Cheng AM, Schecter S, Komotar RJ, Tsai J, Gupta SK. Pituitary Macroadenoma with Optic Cupping Masquerading as Normal Tension Glaucoma. International medical case reports journal. 2023;16:419-423. doi:10.2147/IMCRJ.S422426. PMID:37469851; PMCID:PMC10353559.
Ashok S, Pilling A, Lee-Kwen P, Guterman LR, Weiner A. Normal-Tension Glaucoma Complicated by a Giant Internal Carotid-Ophthalmic Artery Aneurysm. Case reports in ophthalmological medicine. 2024;2024:3878152. doi:10.1155/2024/3878152. PMID:38765219; PMCID:PMC11101248.
Killer HE, Pircher A. Are Generalized Reduced Cerebrospinal Fluid Dynamics and Optic Nerve Sheath Compartmentation Sequential Steps in the Pathogenesis of Normal-Tension Glaucoma? Eye Brain. 2021;13:157-158.
Pazos M, Traverso CE, Viswanathan A; European Glaucoma Society. European Glaucoma Society - Terminology and guidelines for glaucoma, 6th Edition. Br J Ophthalmol. 2025;109(Suppl 1):1-212. doi:10.1136/bjophthalmol-2025-egsguidelines. PMID:41026937.
European Glaucoma Society. European Glaucoma Society Terminology and Guidelines for Glaucoma, 5th Edition. Br J Ophthalmol. 2021 Jun;105(Suppl 1):1-169. doi:10.1136/bjophthalmol-2021-egsguidelines. PMID:34675001.
Gedde SJ, Vinod K, Wright MM, et al. Primary Open-Angle Glaucoma Preferred Practice Pattern. Ophthalmology. 2021 Jan;128(1):P71-P150. doi:10.1016/j.ophtha.2020.10.022. PMID:34933745.
Shen RY, Zhang Y, Chen LJ, Cheung CY, Liang Y, Tham CC, et al. Ocular and Systemic Risk Factors and Biomarkers for Primary Glaucoma: An Umbrella Review of Systematic Reviews With Meta-Analyses. Investigative ophthalmology & visual science. 2025;66(12):35. doi:10.1167/iovs.66.12.35. PMID:40956021; PMCID:PMC12448150.
Krupin T, Liebmann JM, Greenfield DS, Ritch R, Gardiner S, Low-Pressure Glaucoma Study Group. A randomized trial of brimonidine versus timolol in preserving visual function: results from the Low-Pressure Glaucoma Treatment Study. American journal of ophthalmology. 2011;151(4):671-81. doi:10.1016/j.ajo.2010.09.026. PMID:21257146.
Comparison of glaucomatous progression between untreated patients with normal-tension glaucoma and patients with therapeutically reduced intraocular pressures. Collaborative Normal-Tension Glaucoma Study Group. Am J Ophthalmol. 1998;126(4):487-497. doi:10.1016/S0002-9394(98)00223-2. The effectiveness of intraocular pressure reduction in the treatment of normal-tension glaucoma. Collaborative Normal-Tension Glaucoma Study Group. Am J Ophthalmol. 1998;126(4):498-505. doi:10.1016/S0002-9394(98)00272-4.
Copy the article text and paste it into your preferred AI assistant.
Article copied to clipboard
Open an AI assistant below and paste the copied text into the chat box.