Laser trabeculoplasty is a procedure that applies relatively low laser energy to the trabecular meshwork to improve aqueous humor outflow. It is classified as a type of outflow reconstruction surgery. There are two types: argon laser trabeculoplasty (ALT) using an argon laser, and selective laser trabeculoplasty (SLT) using an Nd:YAG laser (532 nm Q-switched frequency-doubled).
ALT was introduced by Wise and Witter in 1979. In the Glaucoma Laser Trial (GLT) from 1990 to 1995, 360-degree ALT showed greater intraocular pressure reduction compared to timolol monotherapy in newly diagnosed primary open-angle glaucoma (9 mmHg vs 7 mmHg)2). It also demonstrated equal or better efficacy in preserving visual field and optic nerve head2). However, due to the decline in effect over time and the emergence of prostaglandin analogs, the use of ALT became limited.
ALT causes significant tissue damage to the trabecular meshwork, and the treated areas become fibrotic, making retreatment at the same site impossible.
In 1995, Latina reported SLT. SLT can selectively irradiate only pigmented cells of the trabecular meshwork, and is less invasive with fewer side effects compared to ALT. It has become widespread because it achieves intraocular pressure reduction equivalent to ALT. Although it is said to cause less thermal damage to tissue and can be repeated, its safety and long-term outcomes remain unclear.
In the LiGHT trial (Laser in Glaucoma and Ocular Hypertension trial, a multicenter RCT of 718 patients), SLT demonstrated efficacy as a first-line treatment for untreated open-angle glaucoma and ocular hypertension1)7)8). At 3 years, 74.2% of patients were managed without eye drops 7), and at 6-year follow-up, 69.8% of eyes maintained target intraocular pressure without additional medication or surgery 1). Based on these results, the EGS 6th edition 3) and AAO PPP 2) recommend SLT as an initial treatment option, and the UK NICE recommends it as a first-line treatment 10).
Glaucoma, the main target disease of laser trabeculoplasty, has a prevalence of 5.8% in individuals aged 40 years and older (Tajimi Study). The prevalence of primary open-angle glaucoma (broad definition) is 3.9%, of which normal-tension glaucoma accounts for 3.6%. Exfoliation syndrome is found in about 4% of people aged 70 years and older, and 20–40% of them have glaucoma.
QWhich is better, SLT or ALT?
A
The intraocular pressure-lowering effect is equivalent. However, SLT has advantages over ALT: less tissue invasion, milder postoperative inflammation, and the possibility of repeat irradiation. ALT cannot be repeated on the same site because the irradiated area becomes organized. The pulse width of SLT (3 nanoseconds) is much shorter than the thermal relaxation time of melanin, selectively photolyzing only pigmented cells without damaging non-pigmented structures. Due to this characteristic, SLT is now the mainstream.
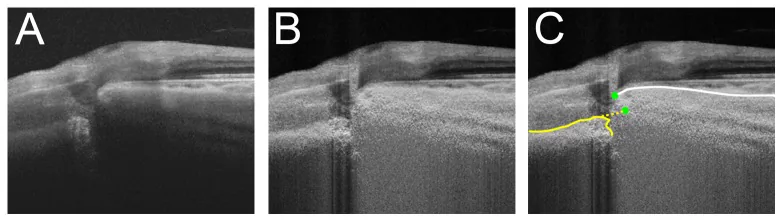
Lee KM, et al. Anterior lamina cribrosa insertion in primary open-angle glaucoma patients and healthy subjects. PLoS One. 2014. Figure 3. PMCID: PMC4273977. License: CC BY.
SS-OCT image of an eye with acquired pit; A: unlabeled, B: after adaptive compensation, C: measurement line indicated by yellow dashed line, showing separation of the lamina cribrosa. This corresponds to optic disc cupping discussed in the section “2. Indications and Contraindications”.
Primary angle-closure glaucoma after laser iridotomy: cases with open angle
Mixed-type glaucoma
When target intraocular pressure cannot be achieved with medication, or when medication cannot be continued for some reason, it is used as an alternative treatment for patients with poor adherence to eye drops (2B)4).
In the 6th edition of the EGS, it is stated that it can be presented as an initial treatment for open-angle glaucoma (evidence level: moderate, strength of recommendation: strong)3). However, evidence of efficacy in severe glaucoma and pigmentary glaucoma is insufficient3).
In advanced stages of glaucoma, the impact of postoperative intraocular pressure spikes is significant, so this procedure is not performed unless there is a special reason. If no effect was obtained in one eye, performing it on the contralateral eye is also a relative contraindication.
QHow many times can laser trabeculoplasty be performed?
A
ALT cannot be repeated at the same site due to tissue organization at the treatment area. If the effect is insufficient after 180-degree treatment, it is possible to add the remaining 180 degrees. SLT is considered repeatable because it causes less thermal damage to the tissue. In the LiGHT trial, 90% of the SLT group achieved a drop-free state for 6 years with a maximum of 2 SLT sessions 1). However, the long-term safety and outcomes of repeat treatment remain unclear.
To prevent transient postoperative intraocular pressure elevation, apraclonidine hydrochloride is instilled 1 hour before and immediately after the procedure 4). The procedure is performed under topical anesthesia 4). A gonioscopy lens is placed to assess the degree of angle opening and pigmentation.
Attach a gonioscopy lens and irradiate 180 degrees, centering on the inferior angle, which often has a wide angle and heavy pigmentation. Focus on the center of the pigment band of the trabecular meshwork, leaving a gap of about 1–2 spot diameters to avoid overlapping spots. The appropriate irradiation energy varies depending on the amount of pigment in the trabecular meshwork. The appropriate intensity is such that the pigment at the irradiated site slightly blanches, and adjust the power to just before small bubbles appear. Irradiating too posteriorly increases the risk of inflammation, pigment dispersion, and peripheral anterior synechiae (PAS) 2). Since 360-degree irradiation increases the incidence of intraocular pressure spikes, 180 degrees is usually sufficient 2). The irradiated site becomes organized, so re-irradiation of the same site is not performed.
Use an SLT-specific lens. Since the spot size covers the entire width of the trabecular meshwork, precise placement is not as necessary as with ALT 3). Start at about 0.6 mJ and irradiate at an intensity that does not produce bubbles. For angles with heavy pigmentation, start at 0.4 mJ; for angles with light pigmentation, set to about 0.8–1.0 mJ 3).
In pigmentary glaucoma, the trabecular meshwork has heavy pigmentation, so it is necessary to start at a lower power than usual 4). The intraocular pressure response is highly variable 4).
In the LiGHT trial protocol, 100 non-overlapping shots (25 per quadrant) were applied to 360 degrees of the trabecular meshwork with energy of 0.3–1.4 mJ 6).
Intraocular pressure (IOP) should be measured 1 to 3 hours after surgery to check for transient IOP elevation 4). If necessary, administer carbonic anhydrase inhibitors or hyperosmotic agents 4). Postoperative inflammation often resolves spontaneously, but depending on the degree of inflammation, corticosteroids may be administered 4).
After ALT, topical steroids are typically prescribed for 4 to 7 days 2). For SLT, postoperative anti-inflammatory medications are often not prescribed, but the SALT trial (2018) showed that anti-inflammatory drugs after SLT do not reduce the laser effect.
This is the most common complication. For SLT, an elevation of 5 mmHg or more has been reported in 4.5% to 27% of cases 2). ALT has a similar frequency. Prophylactic administration of an alpha-2 agonist (apraclonidine hydrochloride) reduces the risk. Rarely, persistent IOP elevation may require trabeculectomy.
In the 6-year data from the LiGHT trial, IOP elevation (≥5 mmHg) related to SLT occurred in only 1.0% (10 procedures) of all SLT procedures, and only one eye required treatment 1). No vision-threatening complications were reported over the 6 years 1).
Mild iritis may occur after surgery. Compared to ALT, SLT results in less postoperative inflammation and a lower risk of peripheral anterior synechiae (PAS) formation.
Cases of acute corneal edema and corneal subepithelial opacities after SLT have been reported. Nijs et al. reported three middle-aged women who developed corneal edema after bilateral simultaneous SLT5). All three had high myopia, and corneal stromal opacities appeared within 24–48 hours postoperatively 5). Corneal edema resolved with dexamethasone eye drops, but hyperopic shift and changes in corneal astigmatism were observed 5). Among 86,634 SLT procedures, 36 cases of corneal edema were reported, indicating a very low incidence 5).
QAre complications of laser trabeculoplasty common?
A
Serious complications are rare. The most common is a transient intraocular pressure spike, which can be reduced by prophylactic apraclonidine hydrochloride eye drops. In the 6-year data from the LiGHT trial, vision-threatening complications were zero, and IOP spikes occurred in only 1.0% of all procedures 1). SLT has even less postoperative inflammation and peripheral anterior synechiae formation compared to ALT, making it safer. Corneal edema is an extremely rare complication.
The IOP-lowering effect of ALT and SLT is equivalent. Maintenance of ≥20% IOP reduction is achieved in about 60% at 1 year and about 20–30% at 5 years, with the effect diminishing over time.
Trial name
Population
Primary outcome
GLT (1990–95) 2)
Newly diagnosed POAG: ALT vs timolol
IOP reduction greater with ALT than timolol (9 vs 7 mmHg)
The LiGHT trial is a multicenter RCT of untreated open-angle glaucoma and ocular hypertension6). 718 patients were randomized, 692 completed 3-year follow-up 7), of which 633 (91.5%) participated in the 6-year extension, and 524 (82.8%) completed 6-year follow-up 1).
Key results at 6 years are as follows 1):
Medication-free rate: 69.8% of eyes in the SLT group maintained target IOP without additional medication or surgery. 90% of medication-free eyes achieved this with a maximum of 2 SLT sessions, and 55.5% with only one SLT session.
Disease progression rate: SLT group 19.6% vs eye drop group 26.8% (P=0.006). Significantly less progression in the SLT group.
Trabeculectomy: SLT group 13 eyes (2.4%) vs eye drop group 32 eyes (5.8%) (P<0.001). In the first 3 years, no eyes in the SLT group required trabeculectomy.
Cataract surgery: 57 eyes in SLT group vs 95 eyes in eye drop group (P=0.03). The eye drop group required approximately 1.7 times more cataract surgeries than the SLT group.
Intraocular pressure at 72 months: SLT group 16.3 mmHg vs eye drop group 15.4 mmHg (P<0.001). Although slightly higher in the SLT group, there were no significant differences in visual field MD (-4.0 vs -3.9 dB) or visual acuity (logMAR 0.1 vs 0.1).
Safety: Zero serious adverse events related to SLT. Intraocular pressure elevation (≥5 mmHg) occurred in 1.0% of all SLT procedures. No corneal changes related to SLT were observed over the 6-year period.
In the eye drop group, more ocular adverse events were reported over 6 years compared to the SLT group (1,470 events vs 897 events)1). Cosmetic side effects (eyelash growth, periorbital pigmentation, iris color change) were also significantly more frequent in the eye drop group (164 events vs 31 events)1).
In the 6th edition of the EGS, the position of laser trabeculoplasty is further strengthened3). For open-angle glaucoma and ocular hypertension, it is recommended to start intraocular pressure-lowering treatment with monotherapy, and laser trabeculoplasty is also considered a good first-line option (evidence level: high, strength of recommendation: strong)3).
Exfoliation glaucoma: ALT and SLT are known to be relatively effective in exfoliation glaucoma, and greater intraocular pressure-lowering effects have been reported compared to primary open-angle glaucoma (1B)4). However, long-term effects cannot be expected. It should be positioned as a bridge to surgery or an emergency measure when surgery is not possible for some reason. In exfoliation glaucoma, many cases have high intraocular pressure and advanced visual field damage at the time of discovery, so surgical treatment should be considered early in cases with insufficient intraocular pressure reduction or large fluctuations.
Pigmentary glaucoma: Due to heavy pigmentation of the trabecular meshwork, treatment should be started at a lower energy than usual4). The intraocular pressure response is highly variable4).
When realistically considering medication adherence with eye drops, laser trabeculoplasty demonstrates higher cost-effectiveness than eye drops 2)3). The LiGHT trial showed that SLT was cost-effective at 3 years 7), and this advantage was maintained at 6 years 1). Generic prostaglandin analogs are cost-effective under optimal adherence, but under real-world adherence, SLT is superior 2).
QIs SLT more effective than eye drops?
A
In the LiGHT trial, the intraocular pressure-lowering effect of SLT and eye drops was equivalent. However, 69.8% of eyes treated with SLT were managed without drops for 6 years 1), and disease progression was significantly lower in the SLT group (19.6% vs 26.8%) 1). The need for trabeculectomy was also significantly lower in the SLT group (13 eyes vs 32 eyes) 1). SLT was also superior in terms of cost-effectiveness 1). Although intraocular pressure was slightly higher in the SLT group, disease progression was less, suggesting that SLT may have protective effects beyond lowering intraocular pressure1).
The exact mechanism of action of laser trabeculoplasty is not fully understood. The goal is to apply relatively low-energy laser to the trabecular meshwork to reduce resistance to aqueous humor outflow through the main pathway from the trabecular meshwork to Schlemm’s canal. The following theories have been proposed.
Mechanical Theory and Cellular Theory
Mechanical theory: In ALT, laser energy causes contraction and scarring of the trabecular meshwork, stretching the surrounding untreated meshwork and facilitating flow into Schlemm’s canal.
Cellular theory: After ALT irradiation, DNA replication and cell division increase, stimulating cell repopulation of the trabecular meshwork.
Biochemical Theory
Cytokine release: Both ALT and SLT release chemical mediators such as IL-1, IL-8, and TNF-α after laser irradiation.
Macrophage recruitment: Leads to remodeling of the extracellular matrix and improved outflow facility.
Schlemm’s canal permeability: When culture medium from SLT-treated trabecular meshwork is added to Schlemm’s canal endothelial cells, fluid permeability increases fourfold.
Electron microscopy findings show that in ALT-treated eyes, thermal destruction of trabecular beams, cell necrosis, and collagen shrinkage are observed. In contrast, in SLT-treated eyes, the general structure of the trabecular meshwork is preserved. The pulse duration of SLT (3 nanoseconds) is much shorter than the thermal relaxation time of melanin (1 millisecond), selectively photolyzing only pigmented cells. This avoids collateral damage to non-pigmented structures. This histological difference is the basis for the repeatability of SLT.
The 6-year data from the LiGHT trial showed that SLT provides better disease control than eye drops in the long-term management of open-angle glaucoma and ocular hypertension1).
Notably, although the SLT group had slightly higher intraocular pressure at 6 years (16.3 vs 15.4 mmHg) than the eye drop group, disease progression was significantly less 1). This suggests that SLT may have protective effects beyond lowering intraocular pressure1).
Another important finding is that SLT can delay or avoid the need for trabeculectomy. Given that the average life expectancy after initial glaucoma diagnosis is 9–13 years and the average time to trabeculectomy is about 10 years, initial treatment with SLT may offer many patients the possibility of avoiding surgery for a lifetime 1).
In the SLT group, 55.5% of patients maintained no need for eye drops with only one SLT session over 6 years, making it a particularly useful treatment option for patients with limited access to healthcare or adherence issues with eye drops 1).
After the publication of the 3-year data from the LiGHT trial, major international guidelines were updated 1).
EGS 6th edition3): Positioned SLT as an option equivalent to medication for initial treatment of open-angle glaucoma (strength of recommendation: strong)
AAO PPP2): Listed SLT as an initial treatment option
UK NICE10): Recommended SLT as first-line treatment
In the future, accumulation of data on the long-term safety of repeat SLT and evidence on its efficacy in severe glaucoma and pigmentary glaucoma will be needed 3).
Gazzard G, Konstantakopoulou E, Garway-Heath D, et al. The Laser in Glaucoma and Ocular Hypertension (LiGHT) Trial. Six-year results of primary selective laser trabeculoplasty versus eye drops for the treatment of glaucoma and ocular hypertension. Ophthalmology. 2023;130(2):139-151. doi:10.1016/j.ophtha.2022.09.009.
Gedde SJ, Vinod K, Wright MM, et al. Primary Open-Angle Glaucoma Preferred Practice Pattern. Ophthalmology. 2021 Jan;128(1):P71-P150. doi:10.1016/j.ophtha.2020.10.022. PMID:34933745.
Pazos M, Traverso CE, Viswanathan A; European Glaucoma Society. European Glaucoma Society - Terminology and guidelines for glaucoma, 6th Edition. Br J Ophthalmol. 2025;109(Suppl 1):1-212. doi:10.1136/bjophthalmol-2025-egsguidelines. PMID:41026937.
Nijs J, Vandewalle E, Stalmans I, Lemmens S. Acute corneal edema and residual subepithelial haze after bilateral selective laser trabeculoplasty: A case series. Saudi journal of ophthalmology : official journal of the Saudi Ophthalmological Society. 2024;38(4):396-400. doi:10.4103/sjopt.sjopt_152_24. PMID:39943961; PMCID:PMC11811399.
Gazzard G, Konstantakopoulou E, Garway-Heath D, et al. Laser in Glaucoma and Ocular Hypertension (LiGHT) trial. A multicentre, randomised controlled trial: design and methodology. Br J Ophthalmol. 2018;102(5):593-598.
Gazzard G, Konstantakopoulou E, Garway-Heath D, et al. Selective laser trabeculoplasty versus eye drops for first-line treatment of ocular hypertension and glaucoma (LiGHT): a multicentre randomised controlled trial. Lancet. 2019;393(10180):1505-1516. doi:10.1016/S0140-6736(18)32213-X.
Katz LJ, Steinmann WC, Kabir A, Molineaux J, Wizov SS, Marcellino G. Selective laser trabeculoplasty versus medical therapy as initial treatment of glaucoma: a prospective, randomized trial. J Glaucoma. 2012;21(7):460-468. doi:10.1097/IJG.0b013e318218287f.
Leske MC, Heijl A, Hussein M, Bengtsson B, Hyman L, Komaroff E; Early Manifest Glaucoma Trial Group. Factors for glaucoma progression and the effect of treatment: the Early Manifest Glaucoma Trial. Arch Ophthalmol. 2003;121(1):48-56. doi:10.1001/archopht.121.1.48.
Glaucoma: diagnosis and management. . 2022. PMID:35438885.
Copy the article text and paste it into your preferred AI assistant.
Article copied to clipboard
Open an AI assistant below and paste the copied text into the chat box.