Over the past decade, the use of glaucoma drainage devices (GDDs) in glaucoma management has increased significantly1). Glaucoma drainage devices consist of a synthetic tube and a plate; the tube drains aqueous humor to the area around the plate posterior to the equator, lowering intraocular pressure1). They are also referred to as “tube surgery”.
The two most widely used glaucoma drainage devices are the Ahmed Glaucoma Valve (AGV, 184 mm²) and the Baerveldt Glaucoma Implant (BGI, 350 mm²). In Japan, both are covered by health insurance. Several large RCTs (ABC study, AVB study) have compared these two types, showing that BGI provides better intraocular pressure reduction but has more postoperative complications, while AGV has fewer complications but less pressure reduction2).
The Paul Glaucoma Implant (PGI, Advanced Ophthalmic Innovations, Singapore) is a new valveless glaucoma drainage device designed to overcome these drawbacks. It features a reduced tube diameter to protect the corneal endothelium and a plate shape designed to reduce the risk of strabismus. However, literature evaluating its efficacy and safety is still limited.
QHow is PGI different from Ahmed or Baerveldt?
A
The Paul Glaucoma Implant (PGI) is a valveless glaucoma drainage device with tube inner diameter (0.127 mm) and outer diameter (0.467 mm) significantly smaller than those of the Ahmed and Baerveldt implants. This reduces the contact area with the corneal endothelium, theoretically lowering the risk of endothelial damage. The shorter width of the end plate reduces the area under the rectus muscles, also decreasing the risk of diplopia. The plate area (342.1 mm²) is slightly smaller than that of the Baerveldt (350 mm²) but significantly larger than that of the Ahmed (184 mm²).
Material: Medical-grade silicone. Highly flexible and easy to implant.
Tube diameter: Inner diameter 0.127 mm, outer diameter 0.467 mm, significantly smaller than Ahmed and Baerveldt. Reduced contact area with corneal endothelium is expected to lower the risk of endothelial cell damage.
Occlusion maneuver: The lumen can be easily occluded with a 6/0 or 7/0 stent. Baerveldt requires a 3/0 polypropylene stent.
Exposure risk: The extraocular portion is smaller, reducing the risk of tube exposure and erosion.
End Plate Characteristics
Dimensions: Width 21.9 mm × Length 16.11 mm
Surface area: 342.1 mm². Slightly smaller than Baerveldt (350 mm²) but significantly larger than Ahmed (184 mm²).
Shape: The anteroposterior diameter is larger than that of Baerveldt, allowing the plate to reach further posteriorly. The width (wingspan) is shorter, reducing the area under the rectus muscles.
Strabismus risk: The reduced width theoretically lowers the risk of postoperative strabismus and diplopia.
The basic technique for glaucoma drainage device surgery is similar to that for the Baerveldt implant. The conjunctiva is incised over at least one quadrant, and anesthesia is administered under Tenon’s capsule. The plate is fixed to the sclera 1 mm posterior to the extraocular muscle insertion. Viscoelastic material is injected into the anterior chamber, a 23G needle is used to create a tract 1.5–2 mm posterior to the limbus, and the tube is inserted into the anterior chamber. The tube is sutured to the sclera and covered with preserved sclera.
Since the PGI is non-valved, a stent is inserted at the tube base to temporarily occlude it in order to prevent early postoperative overfiltration.
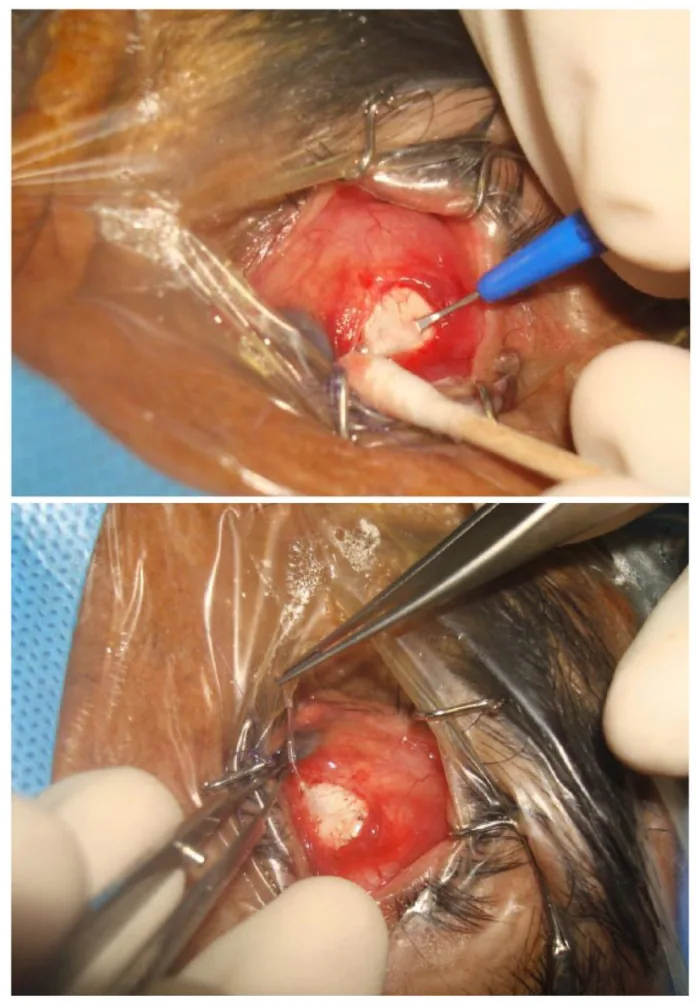
Bryan Chin Hou Ang; Sheng Yang Lim; Bjorn Kaijun Betzler; et al. Recent Advancements in Glaucoma Surgery-A Review. Bioengineering. 2023 Sep 19. Figure 3. PMCID: PMC10525614. License: CC BY.
Intraoperative photograph showing placement of the Paul glaucoma implant. The image illustrates the positional relationship where the plate and tube are positioned under the superior conjunctiva.
Outcomes in Adult Glaucoma
Koh et al. (multicenter prospective study, 74 eyes, 12 months): Failure rate 5.4%. Mean IOP decreased from 23.1 to 13.2 mmHg. Number of medications decreased from 3.3 to 0.3. Main complications: shallow anterior chamber (11 eyes), hypotony requiring intervention (7 eyes), tube obstruction (5 eyes).
Vallabh et al. (retrospective, 99 eyes, 6 months): Failure rate 9.3%. Mean IOP decreased from 28.1 to 13.6 mmHg. Main complications: hyphema (4 eyes), hypotony (2 eyes).
Jose et al. (retrospective, 24 eyes, 12 months): Complete success rate 33%, qualified success rate 75%. Mean IOP decreased from 31.4 to 12.5 mmHg. No hypotony requiring intervention.
Tan et al. (retrospective, 45 eyes, 24 months): Mean IOP decreased from 19.8 to 13.9 mmHg. Number of medications decreased from 3.2 to 0.29. Shallow anterior chamber (10 eyes), clinically significant hypotony (4 eyes).
Outcomes in Pediatric Glaucoma
Elhusseiny et al. (case series, 3 eyes, 9 months): All 3 eyes had postoperative IOP <15 mmHg. No major intraoperative or postoperative complications.
Vallabh et al. (retrospective, 25 eyes, 24 months): Mean IOP decreased from 30.9 to 13.2 mmHg (12 months) and to 11.8 mmHg (24 months). Qualified success rate was 84% at final follow-up. 11 eyes (48%) achieved success without medications.
QCan PGI be used for pediatric glaucoma?
A
Small studies have reported efficacy for pediatric glaucoma. In a study of 25 eyes by Vallabh et al., the limited success rate was 84%, with 48% successful without eye drops. However, the number of cases is limited, and long-term safety data are lacking. In children, the Ahmed glaucoma valve (96 mm² pediatric model) has more extensive usage experience.
QWhat is the risk of postoperative hypotony?
A
Since PGI has no valve, there is a theoretical risk of early postoperative hypotony. In a study by Koh et al., hypotony requiring intervention occurred in 7 of 82 eyes (8.5%). However, in a study by Jose et al. of 24 eyes, no hypotony required intervention. Stent occlusion at the tube base controls early postoperative overfiltration, but intraocular pressure may be elevated until the stent dissolves.
PGI is a relatively new device, and no direct comparative RCTs with other glaucoma drainage devices (Ahmed, Baerveldt) exist yet. Current evidence is mainly limited to single-arm studies and retrospective studies 1).
Future challenges include the following:
Direct comparative RCTs with existing glaucoma drainage devices
Long-term evaluation of corneal endothelial cell loss rate
Verification of postoperative strabismus and diplopia incidence
Accumulation of long-term safety data in pediatric glaucoma
Glaucoma drainage devices are an important option for refractory glaucoma where trabeculectomy is ineffective 3). The TVT study showed that BGI had a higher 5-year success rate in eyes with failed trabeculectomy or with IOL implantation 2). How PGI will contribute to this evidence awaits future research.
Pazos M, Traverso CE, Viswanathan A; European Glaucoma Society. European Glaucoma Society - Terminology and guidelines for glaucoma, 6th Edition. Br J Ophthalmol. 2025;109(Suppl 1):1-212. doi:10.1136/bjophthalmol-2025-egsguidelines. PMID:41026937.
Gedde SJ, Vinod K, Wright MM, et al. Primary Open-Angle Glaucoma Preferred Practice Pattern. Ophthalmology. 2021 Jan;128(1):P71-P150. doi:10.1016/j.ophtha.2020.10.022. PMID:34933745.